ICD-10 Code K25.0: Gastric ulcer, acute with hemorrhage
ICD-10 Code K25.0 is a billable, specific ICD-10-CM code describing a gastric ul...
July 23, 2026
ICD-10 Code S61.122D describes a laceration with foreign body of the left thumb with damage to the nail, coded at a subsequent encounter after active treatment is complete.
The 7th character D signals subsequent encounter – used for ongoing care such as wound checks, dressing changes, and staple or suture removal after initial treatment.
Confusing S61.122D with S61.122A (initial encounter) or S61.122S (sequela) is a common audit trigger – correct 7th character assignment depends on the phase of treatment, not the number of visits.
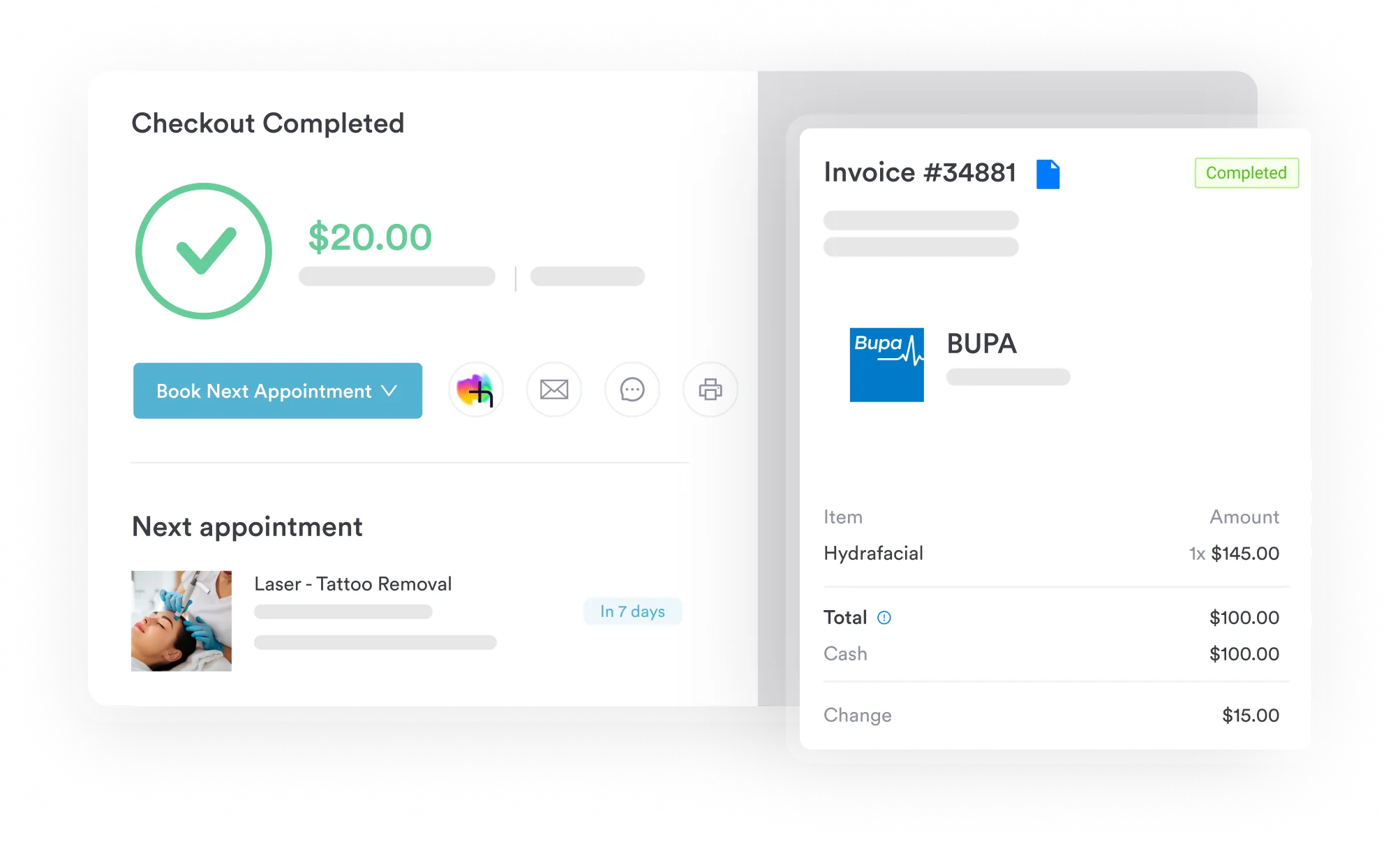
Pabau’s claims management software helps coders and billers track encounter phases, flag 7th character mismatches, and submit cleaner claims for wound care follow-up visits.
ICD-10 code S61.122D is the billable diagnosis code for a laceration with foreign body of the left thumb with damage to the nail, at a subsequent encounter. Coders reach for it when a patient returns for follow-up wound care – a dressing change, a wound check, or suture removal – after the initial treatment is complete.
This reference walks through the 7th character rules that decide when S61.122D applies, the documentation each element needs, the sibling codes across the wider left thumb laceration ICD-10 family, and the CPT pairings that keep subsequent-encounter claims clean.
ICD-10 Code S61.122D designates a laceration with foreign body of the left thumb with damage to the nail, at a subsequent encounter. Four clinical elements have to line up for it to be valid: the wound type (laceration), a foreign body, the laterality (left), and nail damage. The most frequent miscode is keeping A once the encounter has moved into the follow-up phase, where D is correct.
S61.122D sits within Chapter 19 of ICD-10-CM, which covers injury, poisoning, and certain other consequences of external causes (S00-T88). The code is billable for dates of service on or after October 1, 2015, when ICD-10-CM became mandatory for all HIPAA-covered entities. Reimbursement claims submitted before that date required ICD-9-CM codes and will not be accepted with this code.
The full code breakdown reads as follows:
Every component must be present for the code to be valid. Dropping the laterality digit or assigning the wrong 7th character produces an invalid code that payers will reject at clearinghouse level. Physical therapy practices and outpatient wound care clinics are among the most frequent users of S61.x subsequent encounter codes as patients return for dressing changes and suture removal.
The most consequential decision when coding any S61.122 encounter is selecting the correct 7th character. All three options share the same base code – only the final letter changes.
Per the CMS ICD-10-CM coding guidelines, the 7th character is not tied to the number of visits but to the phase of care. A patient can be seen three times under A if active surgical debridement continues across those visits. Conversely, a first follow-up appointment for a routine suture check that was initially treated in the ED transitions to D.
The key distinction: active treatment means the clinician is intervening to repair, debride, or otherwise treat the wound. Subsequent encounter means the wound is healing as expected and the visit focuses on monitoring, dressing changes, or removing closure materials. For ICD-10 subsequent encounter coding across injury chapters, this active-versus-routine distinction is consistent throughout Chapter 19 – not just for S61 codes.
Understanding where S61.122D sits in the classification tree helps coders select the most specific code when clinical documentation supports it. The WHO ICD-10 browser provides the hierarchical framework underlying the CM adaptation used in the US.
Laterality matters for payer validation. Claims submitted with S61.129D (unspecified thumb) when the documentation clearly identifies the left thumb may be flagged for additional documentation or denied outright by payers who require specificity. Always code to the highest level of specificity supported by the clinical record.
Several closely related codes are worth knowing to avoid miscoding when clinical details differ slightly. These represent the broader S61.1 family, which covers all open wounds of the thumb involving nail damage. For a broader view of Chapter 19 injury and trauma codes, the structural logic is consistent across all wound classifications.
The distinction between laceration and puncture wound must come from the clinical note, not the coder’s inference. A cut from a knife is a laceration; a nail gun injury that penetrates the tissue is a puncture wound with foreign body. Using S61.122D when the mechanism was actually a puncture produces a code mismatch that payers may use to justify downcoding or denial. You can verify current code descriptions using the CDC/NCHS ICD-10-CM web tool.
Check whether the foreign body was removed at the initial encounter. If it was, subsequent visits focus on wound healing without active foreign body management – the D code still applies, but clinical notes should confirm removal was completed. Undocumented retained foreign body can create liability and coding discrepancies across encounters.
S61.122D is one code in a wider left thumb laceration ICD-10 family, and the right pick turns on three questions: was a foreign body present, was the nail damaged, and what phase of care is this visit? A patient who ends up on this code but had no foreign body, or an untouched nail, needs a sibling code instead. The table below maps each left thumb laceration presentation to its code at the initial encounter (7th character A). For a subsequent, follow-up encounter, swap the final A for D. For a sequela, use S.
Right thumb injuries follow the same logic with a 1 in the laterality digit instead of a 2. So the ICD-10 code for a right thumb laceration with foreign body and nail damage is S61.121D at a subsequent encounter, mirroring S61.122D on the left. When the note doesn’t state which thumb, the unspecified codes ending in 9 (such as S61.129D) apply, though most payers expect the laterality to be documented whenever the record supports it.
Coding S61.122D accurately requires documentation that supports each clinical element in the code description. Payers – and auditors – match the diagnosis code against the clinical record. Missing even one component leaves the record short of what an auditor expects, which can trigger a request for additional records or a denial. Patient record documentation systems that capture wound assessment details at each visit reduce this risk significantly.
The clinical note must establish all of the following to support S61.122D:
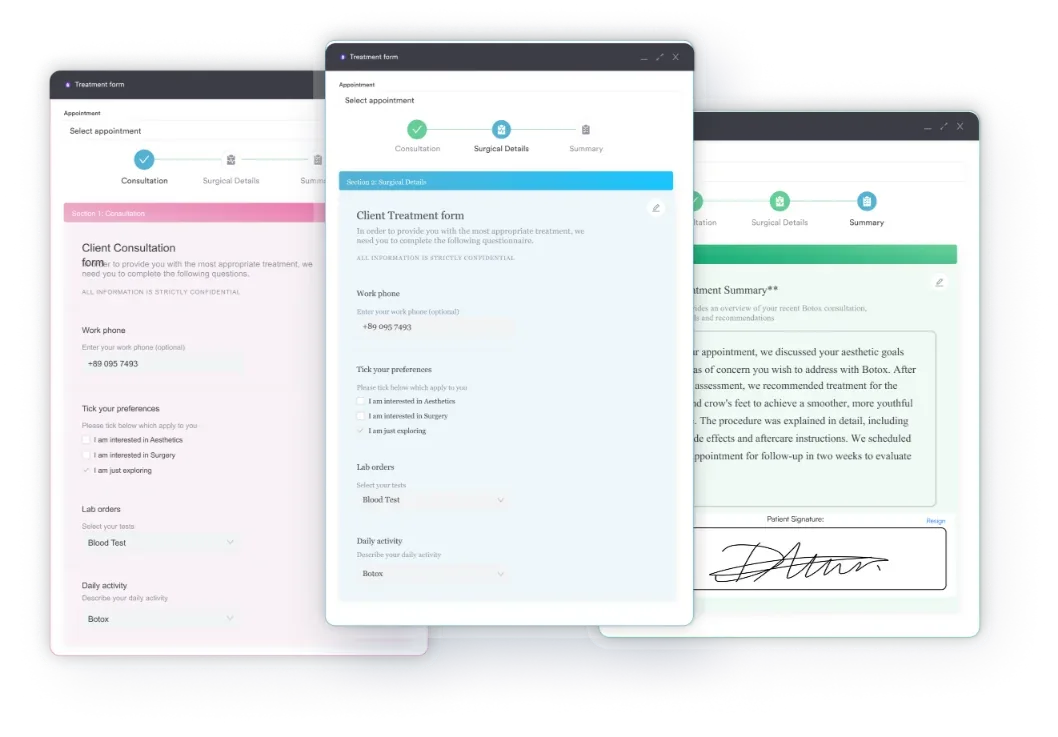
HIPAA-compliant documentation practices require that the record be specific enough to justify the billed service. Providers using digital intake and clinical forms that capture wound assessment fields at each visit create an automatic audit trail supporting the encounter classification. Paper-based or free-text notes frequently omit laterality or nail damage specifics, which are the two details most commonly missing for this code family.
Foreign body documentation deserves particular attention because it’s the element most often assumed rather than recorded. It’s also what separates the foreign body in left thumb ICD-10 codes (the S61.12- and S61.14- groups) from their no-foreign-body siblings, so the object has to be named, not inferred. The initial encounter note must identify the foreign body – glass, wood splinter, metal fragment, plant material, or other material. Subsequent encounter notes should reference whether it was removed and whether any retained material is being monitored.
If the foreign body was removed at the initial encounter and the patient returns for wound care only, S61.122D remains appropriate because the laceration with foreign body (as the injury event) still defines the encounter context. The foreign body element describes the injury, not the current presence of the object. Per the AAPC Codify ICD-10-CM reference, the code applies to the condition as it was initially identified, regardless of current foreign body status at the subsequent visit.
Pabau helps clinics capture encounter-specific clinical notes, track wound care phases, and submit cleaner claims for follow-up visits – reducing denials tied to 7th character mismatches.

S61.122D is a billable ICD-10-CM code, confirmed valid by CMS for the current fiscal year. Subsequent encounter codes in the S61 family are commonly paired with wound care CPT codes. Getting the CPT-to-ICD-10 pairing right is as important as the code itself – payers cross-reference both for medical necessity. Using claims management software that flags encounter-type mismatches at the pre-submission stage prevents a large share of these denials before they reach the clearinghouse.
The following CPT codes are commonly paired with S61.122D at subsequent encounters. Note that CPT code selection depends on what service was actually rendered – the ICD-10 code describes the diagnosis, not the service. Review associated CPT procedure codes guidance to understand how CPT-ICD pairing works across code families.
When submitting subsequent encounter claims, verify that the CPT code’s medical necessity aligns with the diagnosis. A 99213 paired with S61.122D should be supported by a note reflecting clinical assessment of wound healing – not just “patient here for suture removal.” Sparse documentation against a moderate-complexity E/M code is an audit flag. For detailed guidance on clinical documentation best practices, HIPAA-compliant documentation practices outline what constitutes an adequate encounter record for covered entities.
Medicare and most commercial payers accept S61.122D as a valid subsequent encounter diagnosis. However, some payers apply local coverage determination (LCD) policies to wound care services that restrict reimbursement based on wound size, number of visits, or wound type. The ICD List reference database provides additional crosswalk data for this code family that can support LCD compliance reviews.
Workers’ compensation and personal injury carriers may require additional clinical context – mechanism of injury, employer documentation, or prior authorization – beyond what standard Medicare-aligned billing requires. Confirm payer-specific requirements before submitting subsequent encounter claims for workplace hand injuries. The related ICD-10 diagnostic codes framework for coding specificity applies equally here: code to the highest level of specificity the documentation supports, and document that specificity clearly in the record.
Run a pre-submission edit check that flags any S61.12x claim where the 7th character is A but the date of service is more than 30 days after the original injury date. This catches the most common subsequent-encounter miscoding pattern before claims exit your system. Most clearinghouses don’t catch 7th character logic errors – that check has to happen in your practice management system.
Chapter 19 carries specific coding instructions that apply to all S61 codes, including S61.122D. These guidelines are maintained in the official ICD-10-CM coding manual and updated annually. Coders should review the current year’s guidelines through the CDC/NCHS ICD-10-CM tool to confirm no recent updates affect this code’s application. A broader reference for the full code structure across diagnostic categories is available through the ICD-10 subsequent encounter coding guidance applied across Chapter 19 injury codes.
S61 carries a Type 1 Excludes note, meaning these conditions should never be coded simultaneously with S61:
Type 1 Excludes instructions are absolute. If the clinical record describes a traumatic amputation of the thumb, S61.122D cannot be used – even if a wound is also present at the amputation site. The amputation code takes precedence. For additional context on how the ICD-10-CM hierarchy governs excludes logic across diagnostic categories, the Chapter 19 injury and trauma codes framework provides useful context.
ICD-10-CM guidelines recommend – and many payers require – pairing S61.122D with an external cause code (from the V00-Y99 chapter) that identifies how the injury occurred. Common external cause codes for thumb lacerations with foreign body include:
External cause codes do not affect reimbursement directly but support medical necessity documentation and are required for certain payer types and for complete compliance with NCHS guidelines. Workers’ comp and auto-liability payers almost always require external cause codes. The clinical documentation requirements for complete claim submission include external cause coding as a standard best practice for injury-related visits.
Wound care follow-up visits for left thumb lacerations with nail damage are routine – but the coding is not. Getting ICD-10 Code S61.122D right means capturing the correct 7th character, documenting all four clinical elements (laceration, foreign body, laterality, nail damage), and pairing the diagnosis with a CPT code that reflects the actual service rendered.
Pabau’s claims management software supports coders and practice managers with encounter-phase tracking and pre-submission claim edits, helping reduce the S61 denial patterns that most practices don’t catch until an audit. To see how Pabau handles medical documentation workflows from clinical note to submitted claim, book a demo with the team.
Need a structured wound care documentation workflow? Digital intake and clinical forms covers how Pabau captures encounter-specific wound assessment fields at every visit.
Managing multi-encounter injury claims across a practice? Patient record management explains how Pabau structures encounter histories to support audit-ready documentation.
Want context on ICD-10 Chapter 19 injury code structure? Chapter 19 injury and trauma ICD-10 codes provides an overview of how the injury chapter is organized and how 7th characters function across code families.
ICD-10 Code S61.122D is the diagnosis code for a laceration with foreign body of the left thumb with damage to the nail, at a subsequent encounter — used after active treatment is complete and the patient returns for follow-up wound care such as dressing changes or suture removal.
The 7th character D designates a subsequent encounter — routine care during the healing phase after active treatment ends. It refers to the phase of care, not the visit number. Active treatment visits use A; visits for late effects of a healed injury use S.
S61.122A is for initial encounters where active treatment is first provided. S61.122D is for follow-up visits once active treatment has ended. The distinction is treatment phase, not visit count — a patient can have multiple A encounters if active surgical care continues across visits.
Use S61.112D for a subsequent encounter involving a left thumb laceration with nail damage but no documented foreign body. The foreign body element in S61.122D must be supported by clinical documentation — it cannot be assumed.
Use S61.122D. The foreign body element describes the original injury, not current status. As long as the initial injury was a laceration with foreign body and nail damage, S61.122D applies to all subsequent wound care visits even after the foreign body has been removed.
It depends on the wound details. A left thumb laceration with foreign body and nail damage is S61.122A at the initial encounter and S61.122D at follow-up. Without a foreign body it shifts to the S61.112- codes, and without nail damage the S61.01-/S61.02- codes apply. Match the code to what the clinical note documents.
Right thumb codes mirror the left but carry a 1 in the laterality digit instead of a 2. A right thumb laceration with foreign body and nail damage at a subsequent encounter is S61.121D, versus S61.122D on the left side.
CPT describes the service, not the diagnosis. A simple laceration repair on the thumb is reported from the 12001-12007 simple repair range, while follow-up wound care uses codes like 97597 or an established-patient visit such as 99213. Pair whichever service was rendered with the S61.122D diagnosis.