CPT Code 00802: Anesthesia for panniculectomy on the lower abdomen
Most anesthesia claim denials for panniculectomy procedures trace back to the sa...
Last Updated: July 28, 2026
CPT code 00600 describes anesthesia for procedures on the cervical spine and cord, not otherwise specified.
The code carries 10 base units per the VA Community Care Table H and Massachusetts fee schedule.
Use modifier AA when a physician anesthesiologist personally performs the service. QX, QY, or QK apply for CRNA medical direction scenarios.
Pabau’s claims management software helps anesthesia billing teams track modifiers, time units, and claim submissions in one place.
CPT code 00600 is the anesthesia code for surgical procedures on the cervical spine and cord when no more specific code applies. The three most common billing errors on these claims are the wrong code, a missing modifier, and an incomplete anesthesia start-time record.
The official description, as maintained by the American Medical Association (AMA), reads: Anesthesia for procedures on cervical spine and cord; not otherwise specified. The phrase “not otherwise specified” is deliberate.
It signals that this code is the residual option within the 00600-00670 anesthesia range for spine and spinal cord procedures. When a more specific code exists for the same anatomical site and patient position, that code takes precedence. The code remains active and billable under Medicare and most commercial payers.
Degenerative cervical spine conditions are typically mapped on a preoperative MRI of the cervical spine without contrast, and can also prompt a pre-operative bone density workup when osteoporosis is suspected. That scan is billed separately under CPT 77080 and does not change the anesthesia code selected for the spine procedure itself.
Anesthesia billing does not work like standard E/M billing. Payment is calculated using a formula: (Base Units + Time Units + Modifying Units) × Conversion Factor. Each element requires separate documentation.
CPT 00600 carries 10 base units, as confirmed by the VA Community Care Table H and the Massachusetts Anesthesia Service Codes fee schedule. Base units reflect the inherent complexity of the procedure and the anatomical site.
For comparison, CPT 00604 (cervical spine with the patient in the sitting position) carries 13 base units because the sitting position introduces additional hemodynamic risk.
| Code | Description | Base Units |
|---|---|---|
| 00600 | Cervical spine and cord, not otherwise specified | 10 |
| 00604 | Cervical spine and cord, patient in sitting position | 13 |
| 00620 | Thoracic spine and cord, not otherwise specified | 10 |
| 00625 | Thoracic spine, anterior approach without one-lung ventilation | 13 |
| 00626 | Thoracic spine, anterior approach with one-lung ventilation | 15 |
| 00630 | Lumbar spine | 8 |
Source: VA Community Care Table H; Massachusetts Anesthesia Service Codes fee schedule (effective August 1, 2021); Arizona ICA Physicians’ Fee Schedule 2019-2020 (historical reference only; verify current rates with your payer).
Time units are calculated in 15-minute increments. Each 15 minutes of anesthesia time equals one time unit. Anesthesia time begins when the anesthesia provider assumes care of the patient and ends when the provider is no longer in personal attendance. Precise start and end times must appear in the anesthesia record.
A 90-minute cervical spine case yields 6 time units (90 min / 15 = 6). Add those 6 time units to the 10 base units to get 16 total units before applying the conversion factor.
The CMS Physician Fee Schedule publishes the Medicare conversion factor annually. Commercial payers set their own rates by contract. Always verify the current conversion factor with the applicable payer before billing.
Document the exact anesthesia start and end times in the operative record before signing off. Payers routinely audit these timestamps for spine cases, and a discrepancy between the anesthesia record and the surgical log is one of the most common triggers for a retrospective denial.
Modifier selection is where billing teams make the most costly errors on anesthesia claims. The correct modifier depends on who delivered the anesthesia and under what supervision arrangement. Under Medicare, modifier selection also affects payment rate directly.
Physical status modifiers (P1 through P6) are reported by the anesthesiologist to indicate patient condition. P3 and above add modifying units that increase total reimbursement. P1 and P2 add no additional units under most fee schedules.
Qualifying circumstances add-on codes may be reported separately when the clinical situation warrants. These are not modifiers but standalone CPT add-on codes:
These add-on codes carry additional base unit value and require documented clinical justification. Reporting 99140 without chart documentation of an emergency condition is a compliance risk. For anesthesia claims management workflows, tagging cases with qualifying circumstances at the point of care reduces the risk of missed add-on codes at billing time.
The extreme-age criteria behind 99100 apply across the full anesthesia code set, not only spine procedures. CPT 00326 shows the same qualifying circumstance in the airway family, covering anesthesia for infants younger than 1 year.
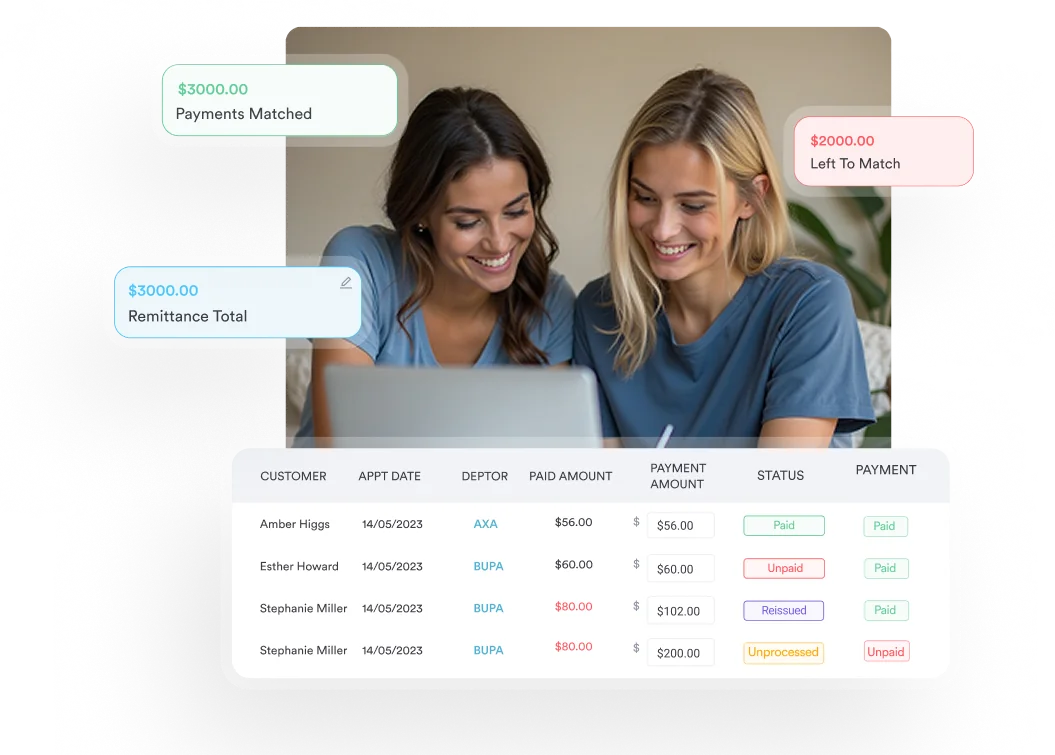
Pabau's claims management tools help surgical and anesthesia practices track modifiers, time units, and claim status in one place, so your billing team spends less time on rework and more time on clean submissions.

Reimbursement for CPT 00600 varies by payer, geography, and contract terms. No single national rate applies across all payers. The following reference points provide a practical baseline for billing teams.
CPT 00600 reimbursement is one piece of a larger process. Pabau’s guide to healthcare revenue cycle management covers how anesthesia charges move from documentation through payment posting.
Medicare pays anesthesia using the formula above. The Medicare conversion factor changes annually. The FastRVU 2026 RVU lookup tool provides current Medicare reimbursement estimates by locality. Because CPT 00600 carries 10 base units, Medicare reimbursement scales directly with the time component of each case. Longer, more complex cervical spine surgeries yield higher reimbursement under this structure.
Medicare billing for anesthesia also involves the HIPAA-compliant submission of Form CMS-1500 or its electronic equivalent. Providers report the elapsed anesthesia time in minutes in field 24G of the CMS-1500. The payer, or Medicare Administrative Contractor, converts those minutes into 15-minute time units during adjudication.
Commercial payers set their own conversion factors and may apply different base unit values. Some payers adopt the ASA Relative Value Guide directly. Others negotiate custom rates.
Always verify CPT 00600 reimbursement against your current fee schedule or remittance advice before quoting patients or projecting revenue. The PGM Billing CPT lookup tool provides a useful free reference using CMS data, though commercial rates will differ.
Practices comparing dedicated billing platforms can review options in Pabau’s best medical billing software comparison.
Workers’ compensation schedules vary by state. The Arizona ICA 2019-2020 fee schedule listed CPT 00600 at $610.00 for 10 units. This figure is historical and cited for orientation only. Current workers’ comp rates require verification with the applicable state schedule. Practices looking to benchmark reimbursement across payers benefit from medical practice management software that integrates payer fee schedules directly.
Clean documentation is the difference between a paid claim and a denial that requires 45 minutes of appeals work. For CPT 00600, payers look for four core documentation elements.
Documentation continuity often extends past the surgical episode itself. Patients recovering from cervical spine surgery frequently need a post-operative physical therapy evaluation, billed separately under CPT 97162.
Spine cases attract closer payer scrutiny than many other surgical categories. Perioperative patient care documentation that captures the full clinical picture reduces the likelihood of medical necessity denials on review. Digital intake and pre-anesthesia forms help standardize what gets captured before the case starts. Pre-procedure digital documentation workflows can automate reminders to complete these records before the case date.
Build a pre-anesthesia documentation checklist into your scheduling workflow. When a cervical spine case is booked, trigger automatic reminders for the pre-anesthesia evaluation, patient history completion, and physical status review. Cases that arrive at billing with complete documentation clear adjudication faster.
CPT 00600 sits within the 00600-00670 anesthesia range for spine and spinal cord procedures. Choosing the wrong code from this family is a common source of incorrect reimbursement. Use the reference below to confirm code selection before billing.
CPT 00604 applies when the patient is placed in the sitting position for a cervical spine or spinal cord procedure. The sitting position carries distinct hemodynamic risks (venous air embolism, hypotension) that justify the higher base unit value of 13.
If the patient is supine or prone, CPT 00600 is correct. If the patient is sitting, CPT 00604 applies. Position documentation in the operative report is essential for supporting whichever code is billed.
CPT 00620 covers thoracic spine and cord procedures not otherwise specified. CPT 00625 and 00626 apply to transthoracic anterior approaches without and with one-lung ventilation, respectively. CPT 00630 covers lumbar spine procedures. CPT 00670 describes extensive spine procedures. Verify payer-specific coverage criteria before reporting it. Each code in this family requires the same documentation standards as CPT 00600.
Anesthesia for spine manipulation performed without open surgical access falls under a separate code. CPT 00640 applies to those manipulation-only cases and should not be confused with 00600 or its surgical-access siblings.
For coders managing a mixed spine caseload, the AAPC Codify CPT lookup tool provides the full 00600-00670 range with descriptor detail and crosswalk information in one view. Practices managing high-volume surgical billing benefit from integrating code reference tools directly into their claim preparation workflow.
The same base-unit-plus-time-unit formula applies outside the spine family too. CPT 00102 uses an identical calculation for head and neck anesthesia, just with a different base unit value.
Cervical spine anesthesia claims are denied for predictable reasons. Most are preventable at the point of documentation rather than the point of appeal.
Practices managing anesthesia billing across multiple surgical sites benefit from centralized practice management workflows that flag incomplete documentation before claims are submitted. Catching denials at the source costs less than working them in appeals.
Wellness practices billing CPT 0591T-0593T follow the same documentation discipline. Precise time capture and a clear clinical justification are required for every billed session.
The relationship between the anesthesiologist and CRNA determines modifier selection and reimbursement level under Medicare. These rules are complex and frequently misapplied.
Medicare’s medical direction rules require the physician anesthesiologist to personally perform seven specific tasks to bill for medically directed services:
If any of these criteria are not met, the claim defaults to supervision rules rather than medical direction, and payment is reduced accordingly.
When a CRNA works without any physician direction (modifier QZ), full payment goes to the CRNA provider. In states that have opted out of physician supervision requirements for CRNAs, QZ billing is the standard arrangement. Verify your state’s opt-out status before defaulting to any specific modifier combination.
Anesthesia practices managing multi-provider billing across different surgical settings benefit from structured practice billing plans that assign modifier rules by provider type and care setting. For practices using surgical specialty EMR software, ensuring modifier workflows are built into the documentation process reduces manual billing errors.
Billing CPT 00600 accurately depends on three things: the right code for the patient position, complete time documentation, and the correct modifier for the care delivery arrangement. Each element is verifiable at the point of documentation, not at the point of appeal.
Pabau’s claims management software helps surgical and anesthesia practices build documentation checkpoints into the workflow before claims are submitted, reducing the manual rework that comes from preventable denials. To see how it fits your billing process, book a demo.
Managing billing across a surgical practice? Time-saving tools for private practices covers the workflows that reduce administrative overhead across scheduling, documentation, and claims.
Want a broader CPT coding reference for specialty procedures? CPT codes for IVF procedures demonstrates how procedure-specific CPT billing follows the same documentation and modifier logic as anesthesia codes.
Evaluating practice management platforms for your anesthesia group? Best medical practice management software breaks down the features that matter most for multi-provider surgical practices.
CPT code 00600 describes anesthesia for procedures on the cervical spine and cord, not otherwise specified. It is used when a more specific anesthesia code within the 00600-00670 range does not apply to the procedure being performed.
CPT 00600 carries 10 base units per the VA Community Care Table H and the Massachusetts Anesthesia Service Codes fee schedule. Base units reflect procedural complexity and are added to time units before multiplying by the payer conversion factor.
The primary modifiers are AA (physician personally performs), QK (medical direction of two to four concurrent cases), QX (CRNA with physician direction), QY (one CRNA directed by one anesthesiologist), QZ (CRNA without physician direction), and AD (supervision of more than four concurrent cases). Physical status modifiers P1-P6 are also reported separately.
Anesthesia time is calculated in 15-minute increments, with each increment equal to one time unit. Time begins when the anesthesia provider assumes care and ends when they are no longer in personal attendance. A 90-minute case produces 6 time units, which are added to the 10 base units before applying the conversion factor.
Use CPT 00604 when the patient is placed in the sitting position for a cervical spine or spinal cord procedure. The sitting position carries additional hemodynamic risks that justify its higher 13 base units. CPT 00600 applies when no sitting position is involved and no other more specific cervical spine code is applicable.