ICD-10 Code M32.9: Systemic lupus erythematosus, unspecified
M32.9 codes SLE when the notes name no organ involvement. Treat it as the fallba...
Last Updated: August 3, 2026
ICD-10 Code M15.3 describes secondary multiple arthritis, a billable diagnosis for polyosteoarthritis arising from an identifiable underlying cause across multiple joints.
Documentation must explicitly identify the causative condition (e.g. post-traumatic origin) to justify M15.3 over the unspecified M15.9, reducing audit and denial risk.
M15.3 differs from M15.0 (primary generalized osteoarthritis) because secondary arthritis has a known etiology, which coders must capture in the clinical record.
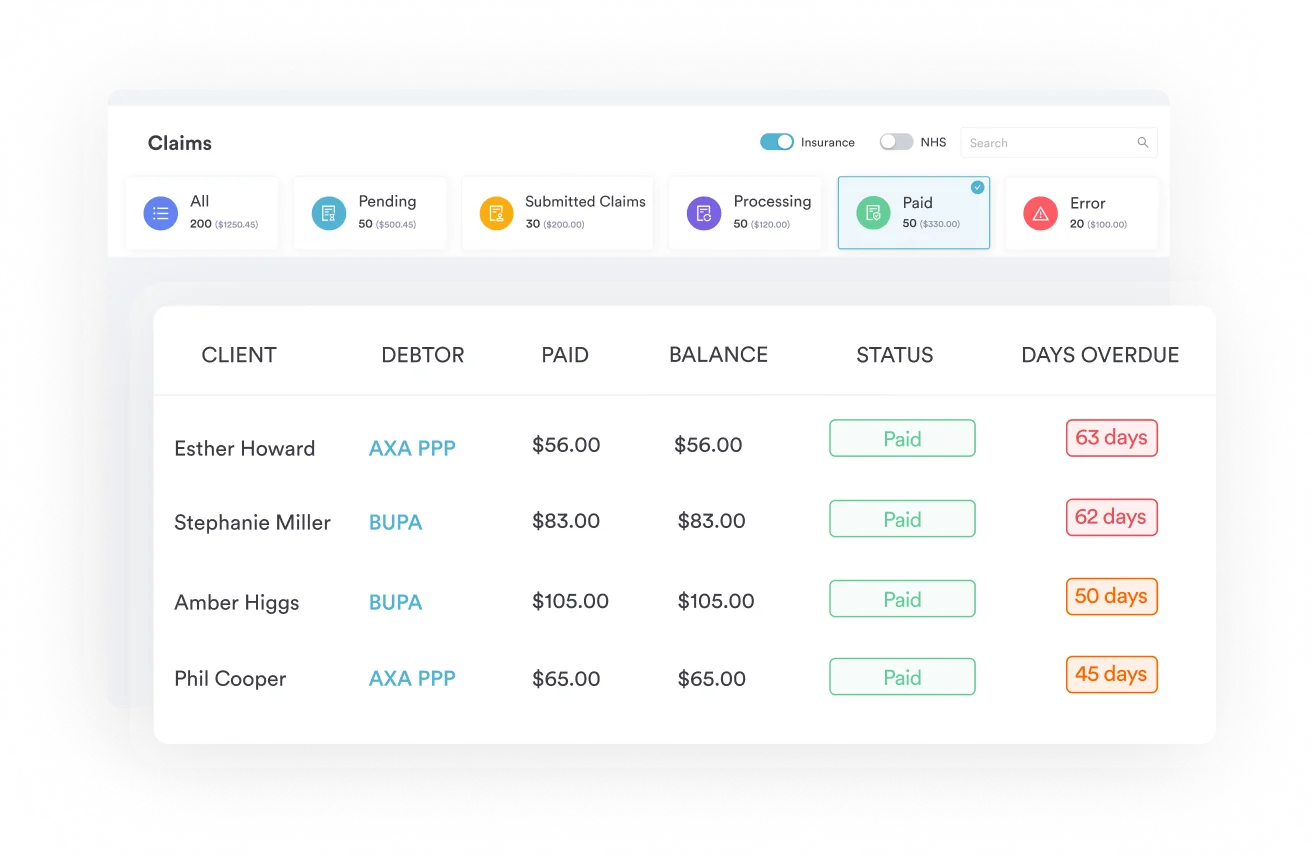
Pabau’s claims management software and AI-powered clinical documentation tools help musculoskeletal practices capture the specificity required to support M15.3 coding.
ICD-10 Code M15.3 is the billable ICD-10-CM code for secondary multiple arthritis: degenerative joint disease across multiple joints with an identifiable underlying cause, such as prior trauma or inflammatory disease. Coders often default to the unspecified M15.9 instead, because the chart doesn’t state the causative condition in the terms payers require.
It is a billable, specific code valid for all fiscal years from 2016 through 2026 and is included in the current CMS tabular list without modification.
As a secondary arthritis ICD-10 code, it sits within the osteoarthritis block (M15-M19) rather than the inflammatory arthropathy chapters.
The term “secondary” is the defining element. It signals that the arthritic degeneration affecting multiple joints arose from an identifiable preceding cause, not from primary idiopathic degeneration. Common causative origins documented under M15.3 include post-traumatic joint injury, prior inflammatory joint disease, metabolic conditions, and structural joint changes attributable to another diagnosis.
“Multiple” requires involvement of more than one joint or joint group. The M15 block formally includes “arthritis of multiple sites,” so single-joint secondary osteoarthritis is captured under M19.x (other osteoarthritis), not under the M15 polyosteoarthritis category. Coders should confirm multi-joint involvement is explicitly stated in the clinical record before assigning M15.3.
Understanding where ICD-10 Code M15.3 sits within the classification tree is essential for accurate code selection and crosswalk work. The code belongs to a clearly delineated three-level hierarchy under the WHO ICD-10 framework as adapted for U.S. clinical use.
The M15 category captures all polyosteoarthritis presentations, meaning those involving multiple joints simultaneously. Coders looking up polyosteoarthritis ICD-10 codes land in this M15 range, where M15.3 is the secondary, multi-joint subcategory.
ICD-10 Code M15.3 is one of seven subcategories within M15, each representing a distinct clinical or etiological presentation. Coders must select the most specific subcategory supported by documentation rather than defaulting to M15.9 (polyosteoarthritis, unspecified).
ICD-10 Code M15.3 is a valid, billable ICD-10-CM diagnosis code confirmed by both the CMS ICD-10 codes page and the AAPC Codify reference. It can be submitted as a primary or secondary diagnosis on professional and facility claims, subject to payer-specific medical necessity requirements.
On facility inpatient claims, M15.3 groups to MS-DRG 553 and 554 (bone diseases and arthropathies, with and without major complication or comorbidity) under MDC 08.
Because the code applies to secondary arthritis, medical necessity documentation must establish two elements clearly: the multi-joint involvement and the identifiable causative condition. Payers auditing claims for M15.3 will look for chart language that explicitly connects prior trauma, metabolic disease, or another specific pathology to the current arthritic presentation.
Practices managing musculoskeletal documentation can reduce denial exposure by using structured intake and clinical note workflows. Claims management software that integrates directly with clinical records helps ensure the required causal language from the provider’s note reaches the claim without manual re-entry errors.
When billing ICD-10 Code M15.3, confirm the chart includes three elements: (1) explicit mention of which joints are affected, (2) documentation of the causative condition or event, and (3) a clear temporal or pathophysiological link between the two. Missing any one element converts a M15.3 case into an M15.9 by default, reducing specificity and audit defensibility.
The most clinically significant distinction in the M15 code range is between M15.0 (primary generalized osteoarthritis) and ICD-10 Code M15.3 (secondary multiple arthritis). Both codes describe multi-joint degenerative joint disease, but their etiologies are fundamentally different, and payers treat them differently for medical necessity and reimbursement purposes.
M15.0 applies when no identifiable cause exists. The arthritic changes are idiopathic, typically age-related, and develop without a specific precipitating condition. Documentation for M15.0 does not require a causal explanation because none exists by definition.
ICD-10 Code M15.3 applies when a causal relationship can be established. Post-traumatic polyosteoarthritis is the most common presentation: a patient with a history of multiple joint injuries develops degenerative changes that the treating clinician links to that trauma history.
Other accepted etiologies include prior inflammatory arthritis, gout-related joint damage, and metabolic conditions that predispose to secondary articular cartilage degeneration.
Coding M15.0 when documentation actually supports M15.3 is a specificity error. It is also a missed opportunity: M15.3 allows the coder to code additional diagnosis codes for the underlying causative condition, providing a fuller clinical picture for risk adjustment and population health reporting.
Physiotherapy clinic compliance requirements frequently reference diagnostic specificity as an audit risk area in musculoskeletal billing.
M15.9 (polyosteoarthritis, unspecified) is the fallback code when documentation does not support a more specific subcategory. Coders should only assign M15.9 after confirming the clinical record lacks the specificity required for M15.3 or another M15 subcategory.
Querying the provider before defaulting to M15.9 is appropriate when chart notes suggest a secondary etiology but do not make it explicit.
Accurate ICD-10 Code M15.3 assignment depends on documentation that satisfies three layers of specificity. Coders working in sports medicine and orthopedics encounter this code frequently in post-traumatic polyosteoarthritis presentations and must know what language makes or breaks the claim.
Practices that use digital intake forms structured around musculoskeletal history gathering capture more of this causative language at the point of patient contact, rather than relying on the provider to add it retrospectively during note review. Structured templates that prompt for prior injury history and prior diagnosis history are particularly effective for secondary arthritis populations.
AI-powered clinical documentation tools can assist by surfacing relevant history from prior encounters and structuring it within the active note, reducing the likelihood that causative language is present in the chart but absent from the visit note that supports the claim.
ICD-10 Code M15.3 is rarely coded in isolation. Secondary multiple arthritis typically co-occurs with the underlying causative condition, associated comorbidities, and therapeutic procedure codes from the physical and rehabilitation medicine range. Understanding the coding ecosystem around M15.3 prevents sequencing errors and strengthens the claim narrative.
When secondary multiple arthritis follows a documented traumatic history, coders may also reference the original injury codes from the S-chapter (S00-S99) to provide historical context, though these are typically coded as additional diagnoses rather than primary. Musculoskeletal EHR systems that link historical encounter data to current visits, backed by built-in compliance management, make this cross-referencing substantially easier at the point of coding.
Patients with secondary polyosteoarthritis often have comorbid spinal conditions worth capturing as an additional diagnosis, such as M47.9, when the record documents it separately from the polyosteoarthritis itself.
Always code the causative condition alongside ICD-10 Code M15.3. For post-traumatic polyosteoarthritis, reference the original injury type in the history documentation even if the acute injury code is no longer the active diagnosis. This creates an auditable causal chain that supports medical necessity and reduces the risk of M15.3 being reclassified as M15.9 on payer review.
The ICD-10-CM Official Guidelines for Coding and Reporting, maintained by CMS and updated annually, govern sequencing and selection for M15 codes. A few specific conventions affect how ICD-10 Code M15.3 is assigned and sequenced in practice.
When the reason for the encounter is treatment of the secondary arthritis itself, M15.3 sequences as the principal diagnosis. The underlying causative condition follows as an additional diagnosis.
When the underlying condition (e.g. gout) is the primary reason for the visit and the polyosteoarthritis is incidental or complicating, the underlying condition sequences first and M15.3 appears as an additional diagnosis.
Practices managing patients with complex comorbidity panels benefit from patient records documentation systems that make historical diagnoses visible alongside the current encounter, reducing sequencing errors when multiple chronic conditions are active simultaneously.
For orthopedic and musculoskeletal specialties that also bill 97124 alongside diagnostic codes, systematizing ICD-10 code validation within the workflow substantially reduces these denial patterns. Embedding code-specific documentation checklists into the clinical note template means coders receive charts that already contain the required language rather than chasing providers for addenda after billing.
Pabau's integrated claims management and digital documentation tools help musculoskeletal practices capture the specificity that supports M15.3 and other diagnostic codes, reducing denials and shortening the revenue cycle.

Practices still maintaining historical records from the ICD-9-CM era, or working with older payer data, may need to crosswalk legacy codes to ICD-10 Code M15.3. Per the CMS General Equivalence Mappings, the approximate ICD-9-CM predecessor is 715.89 (osteoarthrosis involving, or with mention of, more than one site, but not specified as generalized, multiple sites).
ICD-9-CM code 715.09 (osteoarthrosis, generalized, multiple sites) maps forward to M15.0 (primary generalized osteoarthritis) instead, not to M15.3, so it should not be used as the M15.3 crosswalk predecessor.
The crosswalk is not exact. ICD-9-CM did not maintain the same primary/secondary distinction at the multi-joint level that ICD-10-CM formalizes through M15.0 and M15.3.
When converting historical records, coders should review the underlying clinical documentation rather than relying on automated crosswalk tools alone, particularly when the clinical record explicitly documents a secondary etiology that the ICD-9 code may have captured imprecisely.
For research and registry purposes, M15.3 appears in the New York State Department of Health Arthritis Registry Specifications alongside the full M15 code range (M15.0 through M15.9), confirming its inclusion in surveillance and population health datasets.
Coders working across specialties should also track comorbid diagnoses such as M81.6 when the record documents them, particularly in practices participating in quality reporting programs.
The ICD-10-CM alphabetic index maps several clinical presentations directly to ICD-10 Code M15.3. Coders should recognize these synonym entries to avoid missed specificity when the provider uses non-standard terminology in the clinical note.
Searches for post-traumatic osteoarthritis ICD-10 codes also resolve here when multiple joints are involved. When the provider documents any of these terms or clear variants of them, M15.3 is the appropriate code assignment provided multi-joint involvement is confirmed.
If the note says “post-traumatic arthritis” without specifying multiple joints, query the provider before assigning M15.3. A single-joint M19.x code may be more appropriate pending clarification.
M31.6 and other musculoskeletal and systemic condition codes frequently raise the same specificity challenge: the alphabetic index offers multiple entry points, and coders must confirm the clinical documentation supports the chosen code before submission.
Secondary multiple arthritis is a clinically distinct presentation that ICD-10 Code M15.3 captures with precision, provided the clinical record documents the causative etiology and confirms multi-joint involvement. Defaulting to M15.9 when the chart supports M15.3 is a coding specificity error that carries audit and reimbursement consequences.
Pabau’s claims management software and structured clinical documentation tools help musculoskeletal practices build the documentation habits that support specific ICD-10 coding from the point of care. To see how Pabau supports coding workflow accuracy across your practice, book a demo.
Managing a physical therapy or rehabilitation practice? Physical therapy practice management covers the workflow, scheduling, and documentation tools built for musculoskeletal care teams.
Want to reduce claim rework across your billing team? Physiotherapy clinic compliance requirements outlines the documentation standards that reduce denial exposure in musculoskeletal coding.
ICD-10 Code M15.3 is the specific, billable ICD-10-CM diagnosis code for secondary multiple arthritis, classified under category M15 (polyosteoarthritis) in chapter M00-M99 of the musculoskeletal system. It describes degenerative articular changes affecting multiple joints where an identifiable underlying cause, such as prior trauma or inflammatory joint disease, can be documented.
Yes, M15.3 is a valid, billable ICD-10-CM diagnosis code confirmed as billable/specific by CMS and the AAPC Codify reference. It has been continuously valid from FY2016 through FY2026 without modification and can be submitted as a primary or secondary diagnosis on both professional and facility claims.
M15.0 describes primary generalized osteoarthritis with no identifiable cause (idiopathic), while M15.3 describes secondary multiple arthritis where a specific underlying condition, such as post-traumatic joint injury, gout, or prior inflammatory arthritis, caused the degenerative changes. When the clinical record documents a causative etiology, M15.3 is more specific and appropriate than M15.0.
The M15 polyosteoarthritis category covers seven subcategories: M15.0 (primary generalized osteoarthritis), M15.1 (Heberden’s nodes with arthropathy), M15.2 (Bouchard’s nodes with arthropathy), M15.3 (secondary multiple arthritis), M15.4 (erosive osteoarthritis), M15.8 (other polyosteoarthritis), and M15.9 (polyosteoarthritis, unspecified). All require multi-joint involvement.
The ICD-10-CM Official Guidelines require selecting the most specific subcategory of M15 supported by documentation. Assign M15.3 when a secondary etiology and multi-joint involvement are both documented; assign M15.9 only when documentation does not support a more specific code. Always code the underlying causative condition as an additional diagnosis alongside M15.3, and sequence based on the primary reason for the encounter.