Low potassium food list
Download your free low potassium food list A one-page patient handout with two p...
Last Updated: August 3, 2026
SOAP stands for Subjective, Objective, Assessment, and Plan – a documentation framework developed by Dr Lawrence Weed in the 1960s.
Each of the four SOAP components serves a distinct clinical function, from capturing patient-reported symptoms to outlining the treatment plan.
SOAP notes are used across nursing, physiotherapy, mental health, general practice, and aesthetics – not just in hospital settings.
UK clinicians are expected to maintain records that meet CQC, GMC, NMC, and HCPC standards – SOAP structure supports compliance with all four.
Digital clinic management platforms allow SOAP notes to sit inside the same workflow as scheduling, consent forms, and billing.
Clinical notes that drift between formats, skip key findings, or can’t be reconstructed for an audit expose a clinic to failed inspections, malpractice claims, and care-continuity gaps the moment a different clinician opens the chart. SOAP notes were designed to close those gaps with a single, repeatable four-part structure: Subjective, Objective, Assessment, Plan.
An AMA-supported time-and-motion study in the Annals of Internal Medicine found that for every hour US physicians spend on direct patient care, they spend nearly two more hours on EHR and documentation tasks (Sinsky et al., 2016). The format of those notes decides whether that time produces a usable clinical record or just defensive paperwork.
SOAP was developed by Dr. Lawrence Weed in the 1960s as part of his Problem-Oriented Medical Record (POMR) system, first described in his 1968 New England Journal of Medicine paper “Medical records that guide and teach”. Weed’s argument was simple: notes written without structure are hard to audit, hand over, or use as a legal record, and a consistent four-part format fixed all three at once.
That logic still holds. A well-structured clinical note is the primary mechanism by which one clinician communicates the encounter to every clinician who follows, which is why SOAP outlasted every alternative format proposed alongside it.
Each section of a SOAP note performs a different function in the documentation of a patient encounter. Understanding what belongs in each section is the first step toward writing notes that are both clinically useful and defensible under scrutiny.
The Subjective section captures what the patient reports. This includes the chief complaint, the history of present illness, relevant symptoms described in the patient’s own words, pain scores, and any contextual information the patient offers about how the condition developed or changed. The key distinction is that Subjective data cannot be independently measured – it represents the patient’s experience as they communicate it.
For example, a patient presenting at a physiotherapy clinic might report: “Pain in the lower back, started three weeks ago after lifting, worse in the morning, rated 6/10.” None of that can be confirmed by clinical observation alone – it comes directly from the patient. Documenting it accurately creates the foundation for everything that follows in the note.
The Objective section records measurable, observable clinical findings. Vital signs, physical examination findings, range of motion measurements, test results, and any data the clinician collects through direct assessment all belong here. Unlike the Subjective section, Objective data can be replicated – another clinician performing the same assessment should arrive at the same findings.
In a dermatology or skin clinic setting, the Objective section might include photographs, lesion measurements, skin texture observations, and the results of any diagnostic tools used during the consultation. In a mental health context, it might include clinician observations of affect, behaviour, and cognition gathered during the session.
The Assessment section is where clinical reasoning happens. This is the clinician’s interpretation of the Subjective and Objective data – the working diagnosis, differential diagnoses, and clinical impressions. It is the most intellectually demanding part of the note because it requires the clinician to synthesise information and reach a defensible conclusion.
Assessment entries vary significantly by specialty. A GP’s Assessment might list a confirmed diagnosis alongside two differentials. A physiotherapist’s Assessment might describe a functional movement pattern and its likely cause. An aesthetic practitioner’s Assessment might note skin type, condition severity, and treatment suitability based on contraindication review. The format is consistent; the clinical content reflects the specialty.
The Plan section documents what happens next. This includes prescribed treatments, referrals, follow-up appointments, patient instructions, medications considered or prescribed, and any safety netting advice given. It also captures what the patient was told and whether consent was discussed – particularly relevant for aesthetic and elective procedures, and the same documented reasoning supports issuing a medical clearance letter when a patient must be confirmed fit to proceed.
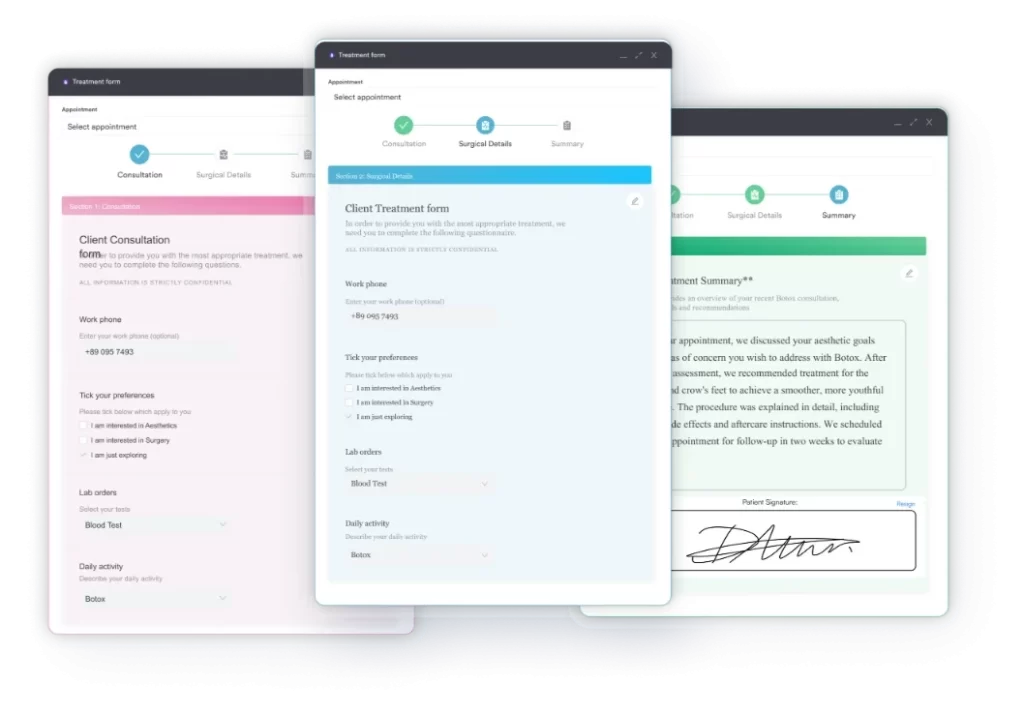
A complete Plan section protects both the patient and the clinician. If a patient returns with a complaint or an adverse event, the Plan entry is the primary evidence of what was recommended, what was communicated, and what the patient agreed to. Clinics using digital consent and documentation tools can attach consent records directly to the Plan section, creating a single auditable record of the encounter.
SOAP notes are not confined to any single profession or setting. According to the Nursing and Midwifery Council (NMC) record-keeping guidance, nurses are expected to maintain clear, accurate, and complete records of patient care – and the SOAP structure is one of the most widely used frameworks for meeting that standard. Similar expectations appear in the HCPC standards for allied health professionals and the GMC’s good medical practice guidance.
In mental health practice, SOAP notes take on additional complexity. The Subjective section often contains detailed accounts of mood, thought patterns, and interpersonal dynamics reported by the client. The Objective section captures clinical observations of behaviour, cognition, and affect. The Assessment requires careful differential consideration – particularly when symptoms overlap across diagnostic categories. The Plan must address therapeutic interventions, medication if applicable, risk management, and safeguarding considerations.
Mental health practitioners sometimes supplement or replace SOAP notes with alternative formats such as DAP notes (Data, Assessment, Plan) or BIRP notes (Behaviour, Intervention, Response, Plan). Each format has its own strengths. DAP combines the Subjective and Objective data into a single section, which some therapists find more natural for session-based documentation. SOAP remains preferred in settings that require a clear separation between patient-reported and clinician-observed information.
Physical therapists use SOAP notes to track functional progress across treatment episodes. The Objective section is particularly data-rich in physical therapy – range of motion measurements, strength assessments, gait analysis, and outcome measure scores all belong there. The Assessment section tracks whether the patient is progressing toward functional goals. The Plan documents the exercise programme, manual therapy approach, and frequency of sessions.
Consistent SOAP documentation across a treatment episode creates a longitudinal record that is invaluable for clinical decision-making. If a patient plateaus, the note history reveals when progress stalled and what interventions preceded that point. That information directly informs whether to modify the treatment approach, refer on, or discharge.
In nursing, SOAP notes document patient care across ward rounds, community visits, and specialist nursing clinics. The NMC is explicit that records must be written contemporaneously, must reflect the care provided, and must be attributable to the clinician who wrote them. SOAP structure supports all three requirements – the four-section format makes it clear what was observed, what was assessed, and what was planned at each encounter.
Community nurses in particular benefit from SOAP discipline because their notes often serve as the primary communication tool between care settings. A district nurse visiting a patient with a wound will document wound measurements and condition in the Objective section, their clinical assessment of healing progress in the Assessment, and the dressing change protocol and next visit date in the Plan. That note may be the only direct clinical record reviewed before the next visit.
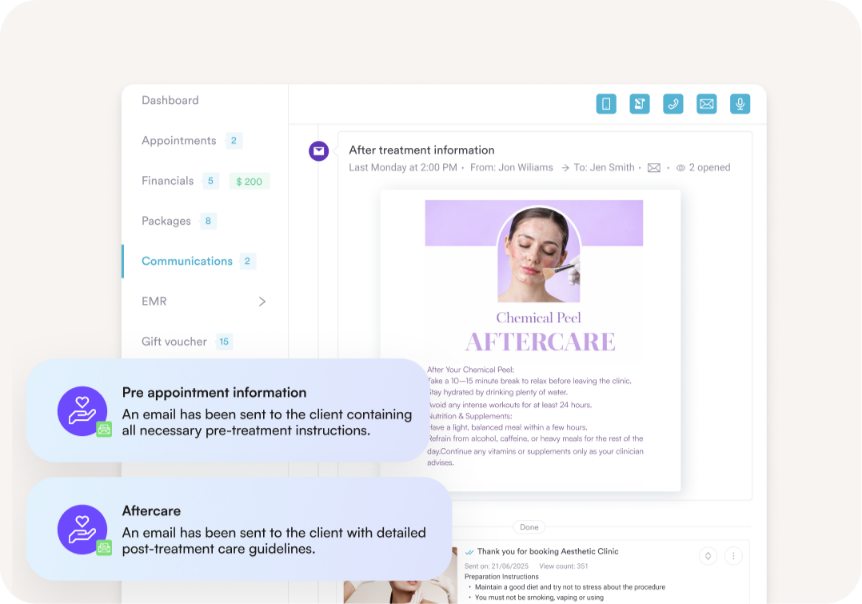
Pabau gives clinics a single platform to document patient encounters, manage digital consent forms, and run scheduling and billing workflows without switching between tools.

Most documentation errors in SOAP notes fall into one of four categories. Recognising them is the first step to avoiding them in day-to-day clinical practice.
The most frequent mistake is mixing Subjective and Objective content. A note that reads “patient reports pain 7/10 and appeared distressed during examination” has merged patient-reported data with clinical observation. Keeping the sections clean matters because it affects how the note reads in an audit, a handover, or a medico-legal review. Subjective content that is verifiable will be challenged; Objective content that is actually opinion will be dismissed.
Under-documentation in the Assessment section is equally common. Writing “lower back pain – treat as before” is not an assessment. It provides no clinical reasoning, no differential consideration, and no evidence that the clinician engaged with the patient’s current presentation. Regulators reviewing records – whether CQC inspectors or professional conduct panels – specifically look for evidence of clinical thinking. A one-line Assessment provides none.
Incomplete Plan sections create a different kind of risk. If the Plan does not document what was communicated to the patient, what was agreed, and what the follow-up arrangement is, the note cannot serve as a record of informed consent or continuity of care. For clinics where practitioners change between appointments – a common scenario in med-spa and multi-practitioner clinic settings – an incomplete Plan leaves the next clinician without the information they need to continue care safely.
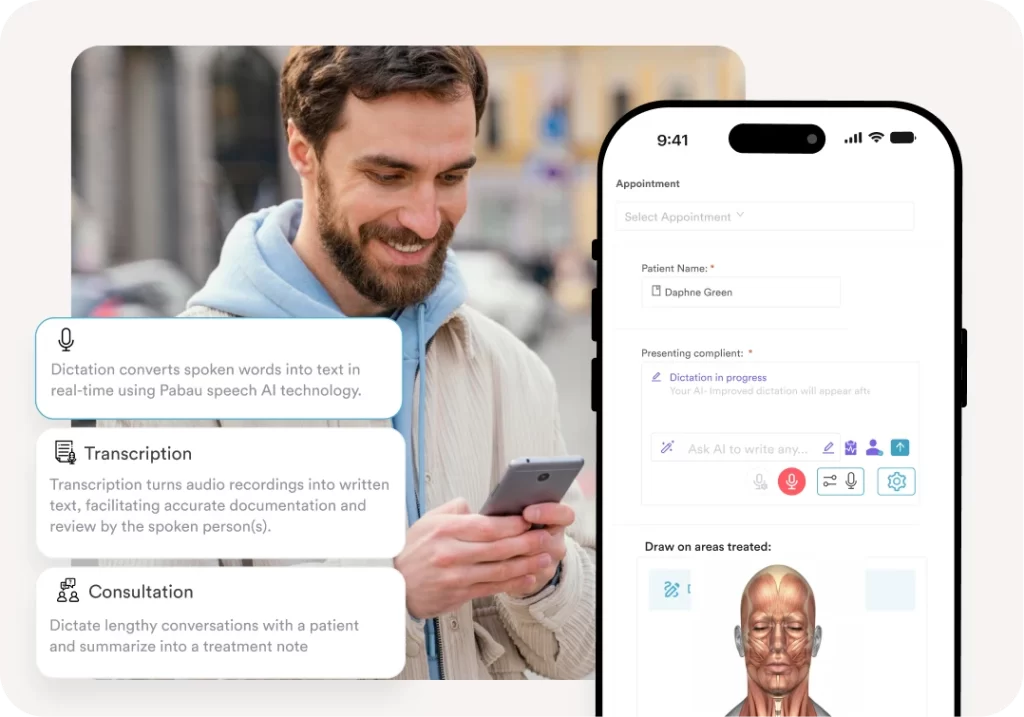
Finally, retrospective documentation – writing notes hours or days after the encounter – undermines the clinical record in two ways. The detail deteriorates with time, and the note no longer reflects what the clinician actually knew and thought at the point of care. Both the GMC and NMC require that records be written contemporaneously. Clinics that use AI-assisted clinical documentation tools can capture notes in real time during consultations, reducing the risk of retrospective documentation becoming a habit.
Audit a random sample of ten SOAP notes from the past month across your clinic. Check specifically whether the Assessment section contains clinical reasoning (not just a diagnosis label) and whether the Plan section documents what was communicated to the patient. Those two sections are the most commonly underdocumented and the most scrutinised in CQC inspections and fitness-to-practise proceedings.
The SOAP notes format works on paper. It also works better in a digital system – not because the format changes, but because of what a digital system can do around the note that paper cannot.
Paper SOAP notes have a structural problem: they are isolated. The note from Tuesday’s appointment has no automatic connection to the consent form signed at the initial consultation, the before-and-after photos taken during treatment, or the follow-up reminder sent to the patient last week. Each of those records sits in a different folder, if it exists at all. In a CQC inspection, assembling a complete picture of a patient’s care from paper records takes significant time and creates room for gaps.
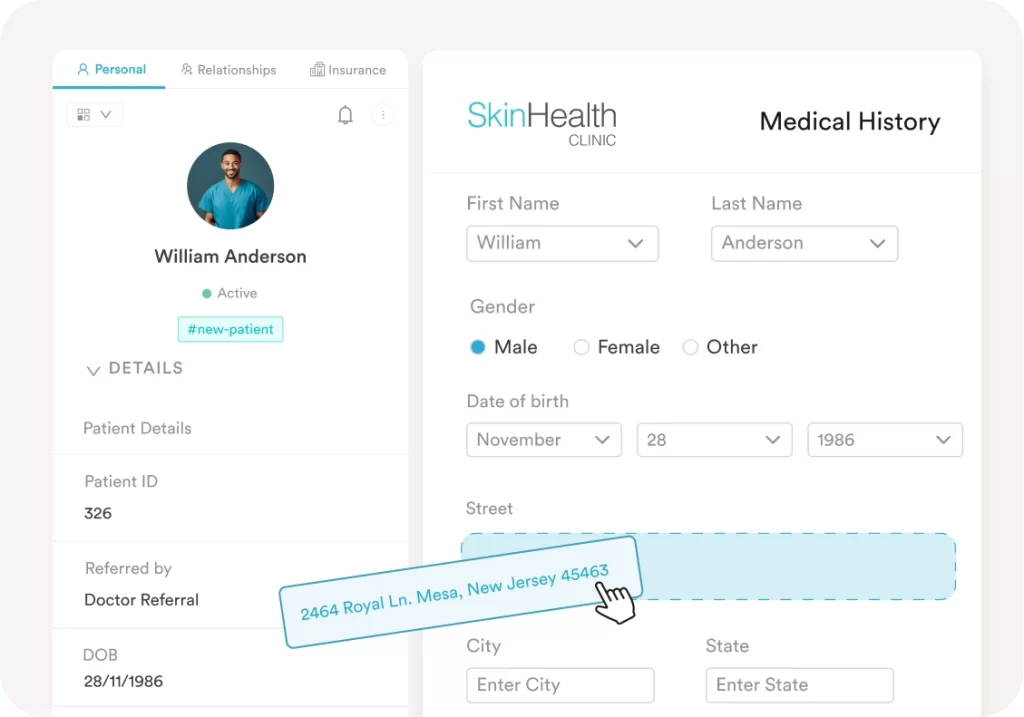
Digital client record systems connect the SOAP note to everything else in the patient’s file. A clinician reviewing a returning patient’s record sees the previous SOAP notes, the consent documents, the treatment history, and any outstanding Plan items from the last visit – all without leaving the note-writing screen. That context makes every subsequent SOAP note more accurate and more complete.
Digital systems also address the UK GDPR and Data Protection Act 2018 requirements that apply to clinical records. The Information Commissioner’s Office (ICO) guidance on healthcare data requires that patient records be stored securely, accessed only by authorised personnel, and retained for the required period. Paper systems make all three requirements difficult to enforce consistently. Electronic records with role-based access controls, audit trails, and automated retention policies address each requirement by design.
For clinics operating across multiple locations, the argument for digital SOAP documentation is even stronger. A patient who attends a different clinic site should not require the treating clinician to work from memory or a phone call to the original site. A multi-location practice management platform makes the complete patient record available at every site, in real time, without additional administrative effort.
The shift toward paperless clinical records in UK private practice has accelerated over the past decade. Practices that made the transition report significant reductions in time spent on administration and on the risk of records being lost, damaged, or accessed inappropriately, freeing time that private clinics can reinvest in growth work such as healthcare lead generation strategies for private clinics.
The regulatory case for structured clinical documentation is explicit. The Care Quality Commission (CQC) evaluates record-keeping as part of its Key Lines of Enquiry under both the Safe and Well-Led domains. Inspectors look for evidence that records are complete, contemporaneous, and attributable – criteria that SOAP structure directly supports.
That same complete, contemporaneous record is also what makes quality measurement workable, and our guide to quality-based care programs shows how point-of-care documentation feeds the metrics behind sustainable quality improvement.
The GMC’s good medical practice guidance requires doctors to “keep clear and accurate patient records” that include “relevant clinical findings,” “decisions made,” “information given to patients,” and “any drugs prescribed or other investigation or treatment.” That is, in effect, a description of the Assessment and Plan sections of a SOAP note. SOAP format gives clinicians a structural prompt to ensure none of those elements are omitted.
For aesthetics and cosmetic medicine practitioners, the medico-legal significance of SOAP notes is particularly high. Clinical negligence claims in elective procedures frequently turn on what was documented in the pre-treatment consultation and the post-treatment follow-up. A well-constructed SOAP note – with a thorough Subjective section capturing patient expectations and concerns, an Objective section documenting clinical findings and contraindication checks, an Assessment section recording the clinical basis for proceeding, and a Plan section confirming what was agreed and communicated – provides the evidence base that any legal or regulatory review will require. For clinics managing compliance documentation across multiple practitioners, having that structure built into every consultation is not optional.
Digital SOAP notes stored in an EMR (see our roundup of the best EMR software) must also comply with UK GDPR under the Data Protection Act 2018. Patient data must be stored securely, retained for the required period (typically a minimum of eight years from the date of last treatment for adults in private practice in England, with shorter minimum periods in Scotland), and deleted appropriately when retention periods expire. Clinics that have not formalised their data governance around clinical records are operating at regulatory risk regardless of how well their SOAP notes are written.
Looking for a SOAP note template tailored to social work documentation? SOAP Notes for Social Work: A Complete Guide to Writing Effective Clinical Notes covers the specific documentation requirements and clinical note format used in social care settings.
Need guidance on what good clinical notes look like across specialties? Safer Clinical Notes provides a practical framework for writing notes that are both clinically rigorous and medico-legally sound.
Managing a physical therapy practice and want to streamline documentation? Physical Therapy EMR Software covers how clinic management tools support documentation, scheduling, and compliance in physiotherapy settings.
Want to understand how AI is changing clinical note generation? AI Scribes and Their Impact on Patient Care explores how automated documentation tools are reshaping note-writing workflows in clinical practice.
The hard part of SOAP documentation isn’t the four sections. It’s making sure every encounter actually gets one, that the right detail lands in the right box, and that the note is still legible to the next clinician six months later.
That’s where a unified clinical record platform earns its place. Pabau locks SOAP structure into every appointment type, and Pabau Scribe drafts the Subjective and Objective sections from your consultation audio so clinicians stop writing notes after hours.
Book a demo with Pabau to see how SOAP documentation, consent, scheduling, and follow-up sit inside one workflow.
SOAP stands for Subjective, Objective, Assessment, and Plan. The acronym describes the four-part structure used to document patient encounters in clinical practice. Subjective captures patient-reported symptoms, Objective records measurable clinical findings, Assessment contains the clinician’s diagnosis or clinical interpretation, and Plan documents the agreed treatment and follow-up approach.
Progress notes is a broader term for any clinical documentation that records ongoing patient care. SOAP notes are one specific format for writing progress notes. Other formats include DAP notes (Data, Assessment, Plan) and BIRP notes (Behaviour, Intervention, Response, Plan). SOAP is the most widely used structure because it separates patient-reported information from clinician-observed findings, which aids clinical reasoning and medico-legal clarity.
Yes. SOAP notes remain the dominant clinical documentation format across nursing, physiotherapy, general practice, mental health, and allied health disciplines in the UK and internationally. While alternative formats exist for specific settings, SOAP’s four-component structure is embedded in clinical training, regulatory guidance, and electronic health record systems globally.
SOAP notes create a structured, auditable record of every patient encounter. They support continuity of care by ensuring that any clinician reading the note has access to both the patient’s reported experience and the treating clinician’s findings and reasoning. They also provide the documentation basis for CQC inspections, fitness-to-practise proceedings, and clinical negligence reviews – making them a fundamental risk management tool as well as a clinical one.
A simple example for a physiotherapy appointment: Subjective – “Patient reports right knee pain rated 5/10, worsening after prolonged sitting, onset six weeks ago.” Objective – “Range of flexion 110 degrees, mild effusion noted, McMurray test negative.” Assessment – “Patellofemoral syndrome, likely aggravated by sedentary work pattern.” Plan – “Commence quadriceps strengthening programme, review in two weeks, advised to take regular movement breaks during working day.”
The Care Quality Commission evaluates record-keeping under its Safe and Well-Led Key Lines of Enquiry. Inspectors look for records that are complete, contemporaneous, and attributable to the clinician who wrote them. SOAP format directly supports all three requirements by providing a structured four-section template that prompts clinicians to document clinical findings, reasoning, and the agreed plan at every encounter.