HCPCS code E0239: Hydrocollator unit, portable billing guide
E0239 covers a portable hydrocollator unit. Medicare pays it as DME with a dated...
Last Updated: August 10, 2026
The craniocervical flexion test (CCFT) is a clinical assessment tool that measures deep cervical flexor muscle function using progressive pressure targets from 22-30 mmHg.
The test produces two outcome measures: the activation score (the highest of the five pressure levels, 22-30 mmHg, the patient can achieve and hold with a clean movement pattern) and the performance index, which is calculated only at that achieved level as the pressure increment above the 20 mmHg baseline multiplied by the number of successful 10-second holds (up to 10).
Normative values vary by age and population; most healthy adults maintain pressure at 28-30 mmHg, while patients with cervical dysfunction typically drop to 22-24 mmHg.
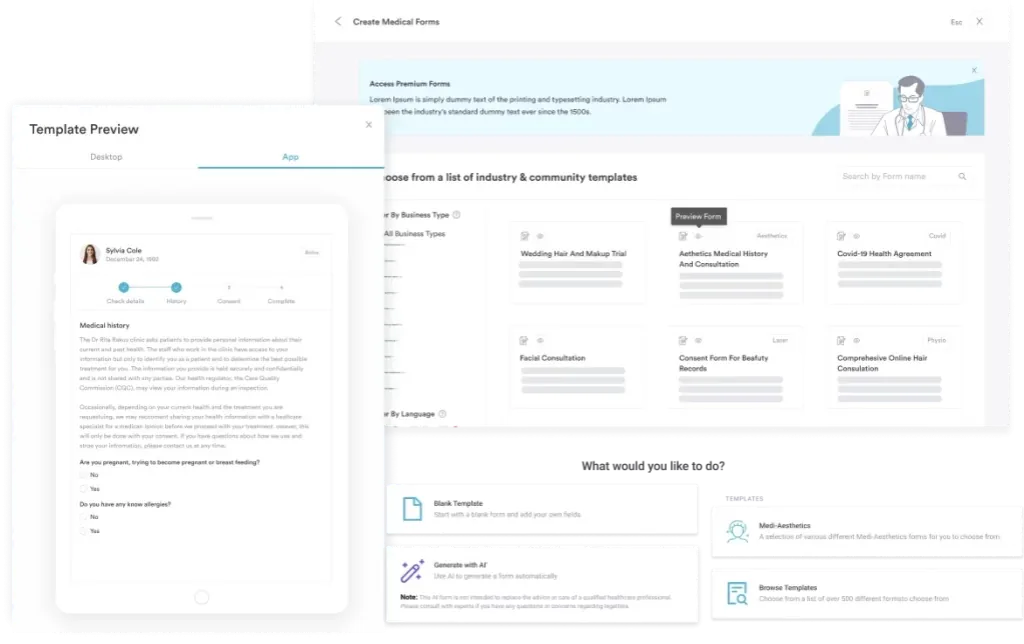
Practice management software like Pabau offers a downloadable CCFT form that integrates the assessment protocol directly into your patient records, so you can store results digitally and track cervical motor control improvements over time.
A standardized assessment form capturing patient positioning, pressure biofeedback inflation, five-stage progression data, hold durations, activation scores, performance indices, and clinical interpretation guidance for deep cervical flexor evaluation.
Download templateThe craniocervical flexion test (CCFT) is a clinical assessment used by physiotherapists, sports medicine practitioners, and manual therapists to evaluate the neuromuscular control of the deep cervical flexor muscles. Unlike broader cervical range-of-motion tests, the CCFT specifically isolates the performance of the longus colli and longus capitis – the muscles responsible for fine motor control in the upper neck.
Understanding how to administer and score the test accurately is essential for identifying cervical motor control deficits in patients with neck pain, cervicogenic headache, whiplash-associated disorder, and post-concussion symptoms.
The craniocervical flexion test is a standardized clinical assessment that measures the ability of the deep cervical flexor muscles to control a gentle nodding motion of the head against progressive resistance.
A pressure biofeedback unit (PBU) – an inflatable pressure sensor placed suboccipitally, behind the upper neck – provides real-time feedback during the test, allowing clinicians to quantify muscle activation levels.
Gwendolen Jull developed the test beginning in the 1990s, publishing the definitive clinical assessment protocol in 2008 (Jull GA, O’Leary SP, Falla DL. Clinical assessment of the deep cervical flexor muscles: the craniocervical flexion test. J Manipulative Physiol Ther. 2008;31(7):525-33). The CCFT distinguishes between the activity of deep cervical flexors and superficial muscles like the sternocleidomastoid and anterior scalene.
Earlier electromyographic (EMG) research established its construct validity separately (e.g., Falla DL et al., 2003, Physical Therapy). That work confirmed the test isolates deep cervical flexor activity rather than superficial muscle substitution.
This differentiation matters because many patients automatically recruit superficial muscles when asked to flex the neck, masking underlying deep cervical flexor weakness. The CCFT’s design forces clinicians to detect this substitution pattern and score only true deep cervical flexor activation.
The deep cervical flexors are a group of small, postural muscles located in the front and side of the neck, deep beneath the larger, more visible muscles. They operate primarily for controlled, low-force movements rather than powerful actions. Understanding their anatomy helps clinicians interpret CCFT results and prescribe targeted rehabilitation protocols.
Patients with chronic neck pain, postural dysfunction, or whiplash injury often show reduced activity of the deep cervical flexors, with compensatory overuse of superficial muscles. The CCFT is sensitive to this substitution pattern. That makes it invaluable for spotting subtle motor control deficits standard range-of-motion testing can miss.
The CCFT is indicated in any patient presentation involving cervical motor control dysfunction or neck-related symptoms. Common clinical scenarios include:
Administering the test correctly is essential for reliable, valid results. The following protocol mirrors the digital form fields in Pabau’s CCFT template, allowing you to capture each step’s data in real time during the assessment.
Two distinct outcome measures are derived from the test, each capturing different information about cervical motor control.
Example: During Stage 1, a patient achieves and holds 24 mmHg cleanly but cannot progress to 26 mmHg without substitution. The activation score is 24 mmHg, a 4 mmHg increment above the 20 mmHg baseline.
In Stage 2, testing only at 24 mmHg, the patient completes 7 successful 10-second holds out of a possible 10. The performance index is the pressure increment multiplied by the successful hold count: 4 x 7 = 28.
Interpreting CCFT scores requires reference to published normative data. Healthy adults without neck pathology typically achieve higher activation scores than patients with cervical dysfunction.
Activation scores below 24 mmHg in otherwise healthy patients warrant investigation into postural habits, stress levels, or previous neck injury. Scores below 22 mmHg indicate significant motor control impairment and typically require targeted rehabilitation documentation and follow-up testing.
Because the performance index is scaled to the level of activation achieved, its absolute value cannot be compared across patients with different activation scores. A performance index of 20 at 22 mmHg is not equivalent to 20 at 28 mmHg.
The most useful application is tracking a patient’s performance index at their own achieved level across visits. An increasing repetition count, or progression to a higher activation level with the endurance test repeated there, both indicate improving deep cervical flexor endurance.
The CCFT has strong psychometric support from peer-reviewed research. Jull et al.’s 2008 study in the Journal of Manipulative and Physiological Therapeutics established the standardized two-stage clinical protocol and reported its reliability.
Separately, earlier electromyographic validation work (e.g., Falla DL et al., 2003, Physical Therapy) confirmed that the test isolates deep cervical flexor activity and excludes superficial muscle substitution.
These values mean that when administered consistently, the CCFT provides reliable baseline measurements for tracking patient progress and justifies its use in clinical practice and research settings.
Clinicians frequently confuse the craniocervical flexion test with the deep neck flexor endurance test. While both assess the same muscle group, they measure different constructs and produce different clinical information. This table clarifies the distinction:
In practice, many clinicians use the CCFT as an initial assessment to identify deep cervical flexor weakness, then progress to the endurance test during rehabilitation to measure functional gains as patients improve their motor control and stamina.
When neck pain radiates into the arm, pairing the CCFT with upper limb tension tests can help confirm whether cervical radiculopathy is also contributing.
While valuable, the CCFT has important limitations that clinicians should recognize when interpreting results:
Pabau’s downloadable craniocervical flexion test template streamlines documentation by mapping the entire assessment protocol into a single, clinic-ready form. Here’s how to use it effectively in your practice:
The form’s structured layout ensures you capture all essential data – patient details, indication, baseline PBU pressure, level-by-level repetition results, visual observations, calculated scores, normative comparison, and clinical summary. This creates a standardized, auditable record suitable for clinical governance, peer review, and third-party payer documentation.
The craniocervical flexion test remains a gold-standard clinical assessment for identifying deep cervical flexor motor control deficits in patients with neck pain, headache, and post-injury dysfunction.
Its high reliability, strong validity evidence, and sensitivity to subtle muscle substitution patterns make it invaluable for baseline assessment and progress tracking.
Using the downloadable template, you can standardize your CCFT administration, ensure consistent scoring, and maintain detailed documentation that supports clinical decision-making and justifies intervention outcomes.
Whether you’re assessing a patient with cervicogenic headache or clearing a return-to-sport athlete, the CCFT provides the objective measurement of deep cervical flexor function that guides effective rehabilitation.
Ready to integrate cervical motor control assessment into your practice? Book a demo to see how Pabau’s downloadable CCFT template and integrated assessment tools streamline patient documentation while maintaining clinical rigor.
Assessing shoulder involvement too? Biceps load test covers a companion special test for differentiating shoulder pathology in patients with combined neck and shoulder symptoms.
Clearing a patient for sport? Personal training questionnaire helps capture fitness goals and exercise history before returning an athlete to full training load.
Need a visual aid for patient education? Knee muscle diagram is a downloadable anatomical reference you can use the same way with patients working through a rehabilitation program.
The craniocervical flexion test (CCFT) assesses deep cervical flexor muscle strength and motor control. It identifies whether patients can activate the deep neck muscles (longus colli and longus capitis) selectively, without over-recruiting superficial muscles. Clinicians use it to detect motor control deficits in patients with neck pain, cervicogenic headache, whiplash injury, and postural dysfunction.
The patient lies supine while a pressure biofeedback unit (PBU) is placed under the upper neck, inflated to a 20 mmHg baseline. In Stage 1, the clinician cues a small nodding motion to progressively inflate the PBU through five pressure levels (22, 24, 26, 28, 30 mmHg), holding briefly at each level to find the highest one the patient can achieve without superficial muscle substitution – this is the activation score. In Stage 2, testing only at that achieved level, the patient performs repeated 10-second holds, up to 10 repetitions, to calculate the performance index.
Healthy adults without neck pathology typically achieve an activation score of 28-30 mmHg. Patients with chronic neck pain average 22-26 mmHg, while acute whiplash patients may score 20-24 mmHg. Scores below 24 mmHg in healthy individuals warrant investigation. The performance index is calculated only at the achieved activation level (pressure increment above the 20 mmHg baseline x number of successful 10-second holds, up to 10), so its value depends on which level a patient reaches – it is best used to track an individual patient’s endurance over repeat testing rather than compared against a single universal cutoff.
The craniocervical flexion test measures the threshold pressure level at which deep cervical flexors activate cleanly (activation score) using a pressure biofeedback unit. The deep neck flexor endurance test measures how long a patient can hold an isometric neck flexion contraction against gravity, without equipment. The CCFT is more selective for deep muscle activation; the endurance test better tracks rehabilitation progress.
Yes. The CCFT has high test-retest reliability (ICC 0.76-0.94) and excellent inter-rater reliability (ICC 0.89-0.96) when clinicians follow the standardized protocol. Electromyographic studies validate that the test isolates deep cervical flexor activation and successfully excludes superficial muscle substitution.
The test assesses the deep cervical flexor muscles: the longus colli (largest and primary), longus capitis, and rectus capitis anterior. These muscles control fine motor movements and stabilization of the upper neck. The test’s design detects substitution by superficial muscles (sternocleidomastoid and anterior scalene), which indicates the deep muscles are not activating adequately.