Two-point discrimination test: Normal values and technique
A normal fingertip reads 2-5 mm, while the forearm needs 30-40 mm. Read more on ...
Last Updated: August 7, 2026
Upper limb tension tests assess neural mechanosensitivity and help diagnose cervical radiculopathy, thoracic outlet syndrome, and peripheral nerve entrapment.
Four ULTT variants target specific nerves: ULTT1 and ULTT2a (median), ULTT2b (radial), and ULTT3 (ulnar) – each requires precise sequencing of shoulder, elbow, and cervical positioning.
Positive criteria include symptom reproduction in the patient’s familiar distribution plus structural differentiation via contralateral cervical side flexion to confirm neural origin.
Practice management software like Pabau lets physiotherapists capture ULTT findings, test variance, contraindication screening, and clinical decision-making in real-time patient records.
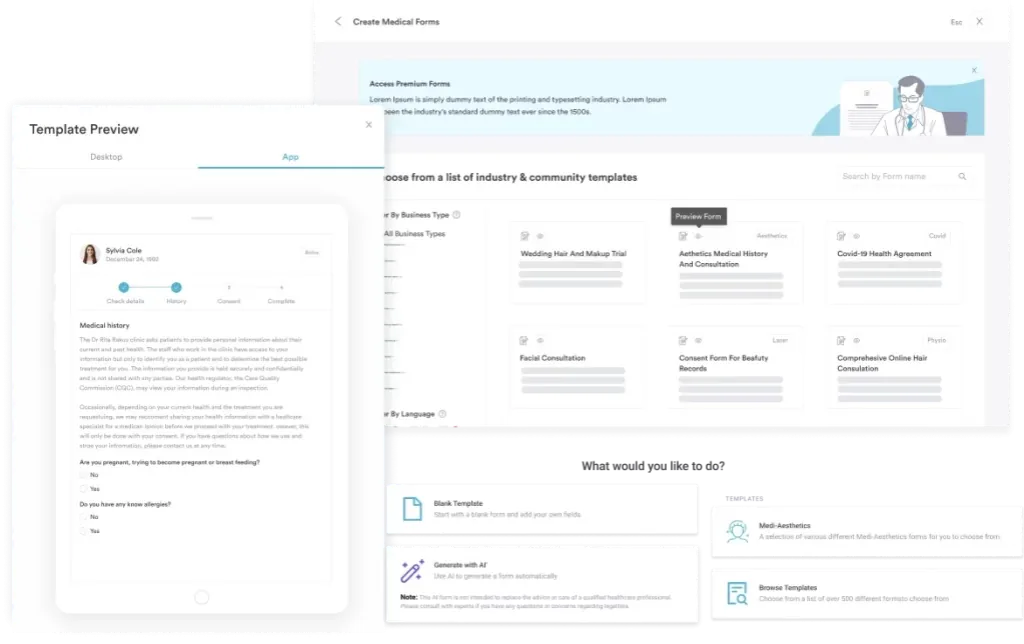
A comprehensive assessment template covering all four ULTT variants (ULTT1, ULTT2a, ULTT2b, ULTT3), step-by-step procedures, positive criteria, contraindication screening, sensitizing movements, and structured documentation fields for clinical notes.
Download templateUpper limb tension tests are specialized neurodynamic assessment techniques used by physiotherapists and allied health professionals to evaluate nerve mobility and identify restrictions in the upper extremity. This practical guide covers the four ULTT variants, how to perform them correctly, how to interpret findings, and how to document results in patient records.
Upper limb tension tests (ULTTs), also called upper limb neurodynamic tests (ULNTs), are assessment techniques that systematically tension specific neural pathways through controlled limb positioning and movement sequences. They help identify adverse neural tension – reduced nerve mobility or mechanosensitivity – which can contribute to arm pain, numbness, tingling, and weakness.
The primary goal is to reproduce the patient’s symptoms while ruling out musculoskeletal causes. Physiotherapists use ULTT findings to diagnose:
Unlike imaging, upper limb tension tests rely on clinical reasoning and patient response. They demand skilled hand positioning, consistent movement sequencing, and sensitive interpretation – exactly why structured digital assessment forms help clinicians standardize their approach and document findings consistently across patient encounters.
Each ULTT variant targets a specific nerve via a unique sequence of movements. The order matters: starting with shoulder depression, moving through abduction and rotation, then progressing to elbow and wrist positioning, and finishing with cervical sensitizing movements. Variation in this sequence can reduce test sensitivity and miss positive findings.
Successful ULTT performance depends on three pillars: consistent positioning, symptom awareness, and structural differentiation.
Positioning: The clinician secures the shoulder girdle (preventing scapular hiking), abducts the arm to near 90 degrees, and sequences elbow, wrist, and cervical movements. The patient lies supine or sits, depending on clinician preference and patient tolerance. Patient positioning must remain stable throughout the sequence to isolate neural tension from muscle tightness.
Symptom reproduction: The goal is to reproduce the patient’s familiar symptoms – pain, tingling, numbness, or heaviness in a dermatome or peripheral nerve distribution. Ask the patient continuously: “Does this feel familiar?” A positive response at a specific movement suggests neural origin. Absence of symptom reproduction suggests the test is negative.
Structural differentiation: Once symptoms appear, move the cervical spine into contralateral side flexion (away from the tested arm). If symptoms reduce with contralateral side flexion, the lesion is neural. If symptoms persist or worsen, the cause may be musculoskeletal or referred pain. This simple maneuver is the clinical linchpin for interpreting ULTT findings.
Record findings in patient records using standardized language: “ULTT1 positive with radicular pain C6 distribution; symptom relief on contralateral cervical side flexion – consistent with cervical nerve root mechanosensitivity.”
A positive upper limb tension test meets two criteria: (1) symptom reproduction in the patient’s familiar distribution, and (2) symptom relief with structural differentiation (contralateral cervical side flexion).
Research shows ULTT1 has high sensitivity (~97%) for cervical radiculopathy but low specificity (~22%), meaning a positive result is moderately predictive of nerve involvement but must be interpreted alongside clinical history, imaging, and other assessment findings. Use ULTT as part of a broader clinical decision-making framework, not in isolation.
Before performing upper limb tension tests, screen for conditions that contraindicate the test. The following are absolute contraindications, meaning you should not perform ULTT at all:
Relative contraindications (proceed with caution and patient consent): chronic pain syndrome, post-surgical patients in weeks two to six after procedures such as those billed under anesthesia codes 01742 or 01830, patients on anticoagulation, and significant anxiety or hypervigilance. In these cases, explain the test clearly, start gently, and stop immediately if symptoms escalate unexpectedly.
Informed consent and safety documentation are always required before proceeding with any relative contraindication.
Accurate ULTT documentation supports continuity of care, clinical decision-making, and medico-legal protection. Structure your notes in five sections:
Use AI-powered clinical documentation to capture these findings in real-time, ensuring consistency and completeness. Structured assessment forms reduce transcription errors and support future audits or clinical review.
This template is designed for physiotherapists, sports physical therapists, occupational therapists, chiropractors, osteopaths, and other allied health professionals conducting upper extremity neurodynamic assessments in private practice and telehealth settings.
It is particularly valuable for practices managing cervical radiculopathy, post-surgical upper limb recovery, thoracic outlet syndrome, and peripheral nerve entrapment cases. The template supports both initial assessment and reassessment at follow-up visits to track changes in neural mechanosensitivity over time.
Consistency: A standardized template ensures every clinician in the practice performs and records ULTT findings in the same way, reducing variation and improving clinical reliability.
Compliance and safety: Built-in contraindication screening and informed consent checkboxes reduce risk of performing ULTT on unsuitable patients and document that safety precautions were followed.
Time efficiency: Pre-populated fields and dropdown menus speed up documentation during and immediately after testing, freeing time for patient education and treatment planning.
Communication: Structured notes are easier for other clinicians (physiotherapists, primary care physicians, specialists) to understand, which improves referral clarity and follow-up coordination across the care team.
Medico-legal protection: Comprehensive documentation demonstrates due diligence, supports clinical reasoning, and provides a clear record if any adverse event or complaint arises.
After a positive ULTT, use your assessment template to document the specific nerve root involved (C5, C6, C7, C8, T1) and the clinical reasoning behind your interpretation. This guides your treatment planning – if median nerve mechanosensitivity is confirmed, nerve mobilization techniques can be prioritized. If musculoskeletal structures are implicated, manual therapy and strengthening take precedence.
ULTT1’s diagnostic accuracy for cervical radiculopathy is well studied: high sensitivity but moderate specificity. That means it is useful for ruling out neural involvement, since a negative result is reassuring, but less useful for confirming a diagnosis on its own.
Sensitivity and specificity data for the other three variants is far more limited, so treat the figures below as illustrative rather than firmly established.
*Sensitivity and specificity figures for ULTT2a, ULTT2b, and ULTT3 come from a smaller, less consistent evidence base than the well-established ULTT1 statistics (Wainner et al., 2003). Treat them as illustrative rather than firmly established values, and weigh them alongside clinical history and other findings.
Clinical reasoning matters more than any single test result. Combine ULTT findings with history (mechanism of injury, pain pattern, neurological deficits), palpation, range of motion, strength testing, and imaging when available.
A positive ULTT in a patient with classic cervical radiculopathy symptoms and imaging findings has strong diagnostic value. A positive ULTT in the absence of other supporting findings warrants further investigation before committing to treatment.
Tracking ULTT results over time helps gauge treatment effectiveness. If neural mechanosensitivity improves (positive ULTT becomes negative, or symptom reproduction moves later in the test sequence), clinical progress is being made.
A positive ULTT result is not a diagnosis – it is evidence of neurodynamic dysfunction that informs treatment direction. Once ULTT positivity is established, the next question is: what is causing the neural restriction?
Cervical spine involvement suggests cervical mobilization, traction, and neural tension release techniques, with nerve root compression typically coded as G55. Peripheral nerve entrapment (carpal tunnel, cubital tunnel) may warrant local decompression maneuvers, splinting, or ergonomic modification. Post-surgical scarring or adhesion responds to gentle neural mobilization and soft tissue release.
Document your clinical reasoning in the assessment template: “ULTT1 positive suggesting C6 nerve root irritation; MRI confirms small disc herniation at C5-C6. Treatment plan: cervical mobilization, home neural tension exercises, and reassessment of ULTT at 2 weeks to monitor mechanosensitivity improvement.”
Linking assessments to treatment plans this way supports evidence-based practice and makes outcomes tracking measurable.
Upper limb tension tests are a cornerstone assessment for physiotherapists and allied health professionals evaluating upper extremity neuromuscular complaints. Mastery requires understanding the anatomy, perfecting the movement sequence, and interpreting findings within the broader clinical context.
The free downloadable template provides a structured framework for consistent, safe, and well-documented ULTT assessment. Use it to standardize your approach across the practice, protect patient safety through contraindication screening, and build a longitudinal record of neurodynamic improvement. Book a demo to see how Pabau’s structured forms and AI-powered clinical documentation can support your practice’s assessment and outcome tracking workflows.
Need a companion outcome measure for upper limb function? Action Research Arm Test scores grasp, grip, and pinch to track functional change alongside ULTT findings.
Need guidance on structured patient intake and history for neurodynamic assessment? Patient scheduling workflows show how to integrate pre-assessment screening into your practice’s digital workflow.
Interested in the broader physiology behind neural tension? Return-to-running assessment protocols cover neurodynamic testing as part of comprehensive lower-limb clearance, with principles that transfer to upper-limb assessment.
ULTT1 and ULTT2a both target the median nerve, but ULTT2a includes radial deviation of the wrist during the test sequence, adding a radial nerve sensitizing component. Use ULTT1 for general median nerve screening; use ULTT2a when radial nerve involvement is suspected.
ULTT findings suggest neural mechanosensitivity but do not diagnose a specific condition. Positive ULTT, combined with history and imaging, may support cervical radiculopathy, thoracic outlet syndrome, or peripheral nerve entrapment (carpal tunnel, cubital tunnel). Clinical interpretation with imaging and specialist referral is needed for definitive diagnosis.
No, ULTT is contraindicated in acute neural irritability, severe pain, and immediately post-surgery (first 6-8 weeks). Always perform contraindication screening using the assessment template before testing. If in doubt, defer the test and consult the referring physician.
Structural differentiation is a technique to confirm neural origin: after symptom reproduction, move the cervical spine into contralateral side flexion (away from the tested arm). If symptoms reduce or resolve, the cause is likely neural. If symptoms persist, the cause may be musculoskeletal or vascular.
Repeat ULTT at least bi-weekly during treatment to track changes in neural mechanosensitivity. Progressive improvement (delayed symptom reproduction or reduced symptom intensity) indicates effective treatment. Static or worsening ULTT findings may signal need for treatment modification or medical referral.