HCPCS code J0636: Calcitriol injection billing guide
HCPCS code J0636 covers injection, calcitriol, 0.1 mcg, billed per unit under Me...
Last Updated: August 7, 2026
CPT code 99350 is a home or residence visit code for established patients requiring high complexity medical decision making (MDM), or total time of 60 minutes or more on the date of service — there’s no upper time cap.
Post-2023 AMA guidelines: total time includes pre- and post-encounter work on the same date of service, but excludes travel time to and from the patient’s home.
Missing a time attestation statement, treating the time threshold as a capped range instead of an open-ended minimum, or using the wrong place of service code are common audit triggers for 99350 claims.
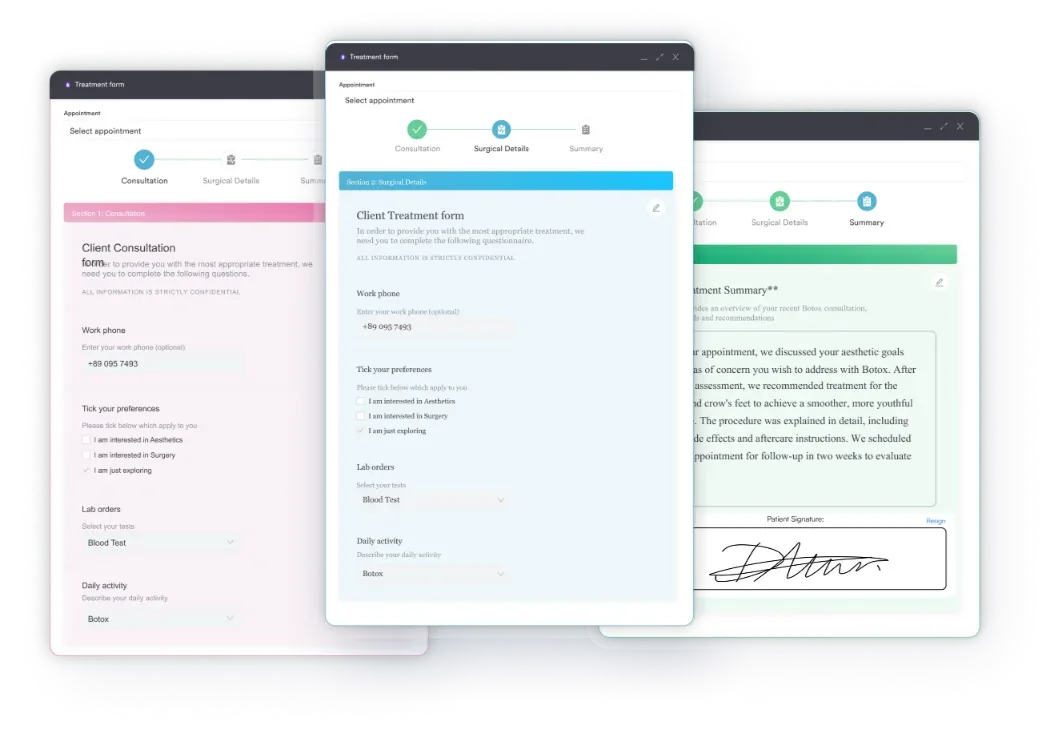
Pabau’s digital intake forms and treatment-note templates help home-visit practices document MDM detail and time attestations consistently, keeping records audit-ready — Pabau’s own claims tools are built for UK private-insurance billing, not US Medicare claims submission.
Home visit billing gets denied more often than almost any other E/M category. Claims examiners scrutinize CPT code 99350 closely because it sits at the top of the established-patient home visit hierarchy, and upcoding audits for this code appear regularly in the HIPAA-compliant documentation practices space.
If you’re billing house calls or residence-based care — common for GP practices — getting the selection criteria right is non-negotiable.
This reference guide covers CPT code 99350 selection criteria, MDM thresholds, time-based billing rules, 2026 fee schedule data, documentation requirements, and the most common errors that trigger claim denials and OIG audit flags.
CPT code 99350 describes a home or residence visit for an established patient who is unstable, has developed a significant new problem requiring additional workup, or requires high complexity care.
The American Medical Association (AMA), which owns and publishes the CPT code set, defines an established patient as one who has received professional services from the same physician (or a qualified clinician in the same practice) within the past three years.
Two selection pathways qualify a visit for CPT code 99350:
One pathway is sufficient. The clinician documents whichever applies, not both.
CPT code 99350 applies when a visit involves clinical complexity that clearly exceeds the moderate-complexity threshold of CPT 99349. Three clinical scenarios commonly qualify.
Practices focused on geriatric care, functional medicine and home-based care, and post-acute transitions will encounter these scenarios frequently. The key is matching the documentation to the complexity of the decision made, not the complexity of the patient’s overall history.
High complexity MDM requires meeting threshold criteria in at least two of three MDM elements. The AMA revised these criteria effective 2021 for office visits, with the same framework applied to home visit codes from 2023 onward.
Meeting two of three elements at the high complexity level supports CPT code 99350. The note must document the specific problems addressed, the data reviewed, and the risk level of the management decisions. Stating “high complexity MDM” without supporting detail is an audit red flag.
Document the risk element explicitly. The phrase ‘decision regarding hospitalization considered but deferred given patient preference’ captures the high-complexity risk threshold in one sentence and survives MAC review. Vague language like ‘complex visit’ does not.
When time is the basis for CPT code 99350, the clinician must spend 60 minutes or more in total time on the date of service. Unlike the deleted pre-2023 model, there’s no upper cap here — 60 minutes is a floor, not a range. This is where many practices still apply the old rules incorrectly.
Post-2023, “total time” includes all time on the date of service directly related to the patient encounter: reviewing records before the visit, the face-to-face encounter itself, ordering tests, documenting the note, and communicating results or referrals afterward.
Travel time to and from the patient’s home does not count, even though it still adds to the cost of home-visit care. Time spent on the same date of service by clinical staff under the supervising clinician’s direction doesn’t count either.
For time-based selection decisions across the 99347-99350 series, use this quick reference — each figure is a minimum, not a range:
Once total time runs well beyond the base threshold, don’t just absorb the extra minutes into the base code — report the additional time separately using a prolonged-services add-on code.
CPT +99417 covers each additional 15 minutes for most payers, while Medicare uses HCPCS G0318 instead, reportable once total time reaches 110 minutes or more for CPT 99350 (140 minutes or more for the new-patient equivalent, CPT 99345).
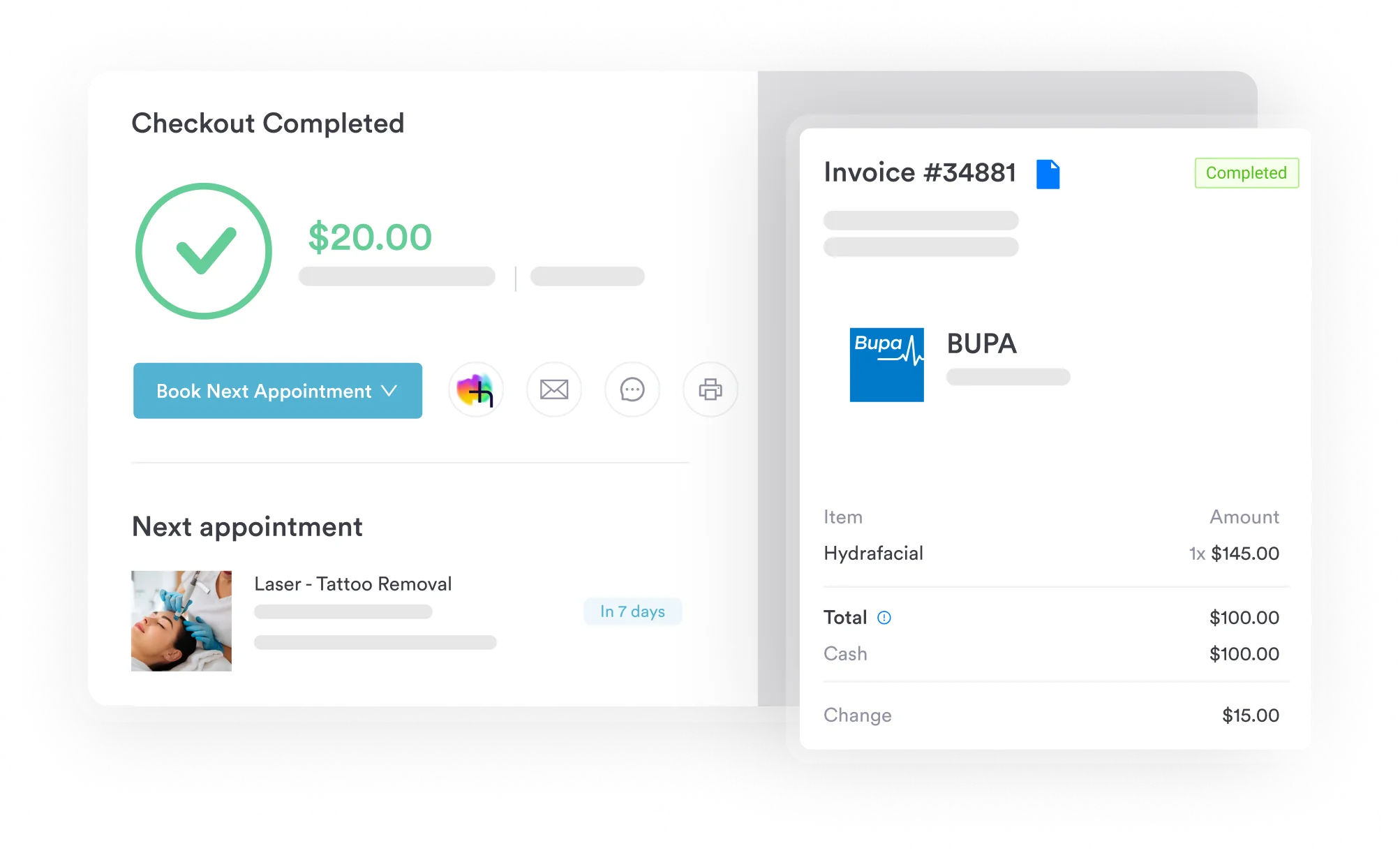
Pabau helps home visit practices capture total time, track MDM complexity, and submit cleaner claims. See how billing workflows built for high-complexity visits can reduce your denial rate.

Insufficient documentation is the leading cause of CPT code 99350 claim denials and overpayment demands on audit. The record must support whichever selection pathway was used: MDM or time.
Use digital intake forms and clinical documentation to capture required elements consistently at the point of care. Below is the minimum documentation checklist for a compliant 99350 claim.
Place of service (POS) determines the reimbursement rate. POS 12 applies when the visit occurs in the patient’s private residence. POS 14 applies for group homes or assisted living facilities. Using POS 12 for a visit that took place at an assisted living facility is a coding error that can result in overpayment recovery.
Medicare reimburses CPT code 99350 based on its relative value units (RVUs) multiplied by the annual conversion factor, then adjusted by the geographic practice cost index (GPCI) for the practice’s location. The CMS Physician Fee Schedule lookup tool allows clinicians to verify current rates for their specific MAC jurisdiction and locality.
Based on the 2026 Medicare Physician Fee Schedule, CPT code 99350 carries a total non-facility RVU of approximately 5.78, which works out to roughly $193 nationally once multiplied by the 2026 conversion factor (before geographic adjustment).
Rates vary by geographic locality, so verify the exact figure for your location using the FastRVU lookup tool before publishing or communicating rates to patients.
Private payer rates for CPT code 99350 typically follow Medicare as a benchmark but vary by contract. Some commercial payers reimburse 100-150% of Medicare rates for home visit codes; others apply flat fee schedules. Always verify rates against your individual payer contracts.
The diagnosis code submitted with CPT code 99350 must reflect the clinical reason for the visit’s high complexity. The ICD-10 code should be the condition driving the MDM decision, not a background chronic condition if a new problem is the primary reason for the encounter.
Common ICD-10-CM diagnoses paired with 99350 include unstable or exacerbating chronic conditions, new problems that need urgent workup, and diagnoses tied to palliative or end-of-life care planning. The diagnosis should always match the clinical reason for the visit’s complexity, not just a background condition sitting on the patient’s chart.
ICD-10-CM codes update annually on October 1. Verify all codes against the current year’s tabular list. MAC Local Coverage Determinations (LCDs) in your jurisdiction may specify which diagnoses support medical necessity for home visit billing. Check your MAC’s LCD library before assuming coverage.
The 99341-99350 series covers all physician and qualified clinician home and residence visits. Effective 2023, the former domiciliary and rest home codes (99324-99337) were retired and merged into this unified series, which now applies to private residences, assisted living facilities, group homes, and rest homes alike.
That same 2023 revision deleted CPT 99343, so the new-patient side of the series now has four levels — 99341, 99342, 99344, and 99345 — mirroring the four established-patient levels, 99347-99350.
The distinction between 99349 and 99350 comes down to a single MDM level: moderate vs high complexity. Both codes apply to established patients.
If a patient with stable chronic conditions has a routine medication review and no new problems, that is 99349 territory regardless of how long the visit runs. Spending 65 minutes with a stable patient does not automatically qualify for 99350 unless the MDM genuinely reaches the high complexity threshold.
When time is the selection basis, 99349 requires 40 minutes or more and 99350 requires 60 minutes or more — both thresholds are open-ended minimums, not ranges. If the clinician spent 58 minutes, that supports 99349, not 99350, since the 60-minute threshold for 99350 hasn’t been met. Document the actual time and bill accordingly.
Review your 99350 claim volume as a percentage of all home visit claims quarterly. A rate above 25-30% of established patient home visits may attract MAC scrutiny. National data consistently shows 99350 is the highest-intensity code in the series and should not be the most frequently billed level.
The Office of Inspector General (OIG) has identified home visit E/M codes as a recurring focus area for billing compliance audits. CPT code 99350 carries heightened scrutiny because it carries the highest reimbursement in the established-patient home visit series.
Practices billing high-complexity home visit codes should also confirm the diagnosis on the claim genuinely supports the MDM level billed, since medical necessity for high-complexity E/M codes is a recurring OIG Work Plan audit target.
Home visit billing has more moving parts than office-based E/M coding: clinicians travel between locations, time tracking is manual, MDM documentation happens away from a desktop, and claim submission is often delayed. Each of these factors adds to the conditions for the errors listed above.
Reviewing practice management software features designed for mobile clinical workflows, alongside broader practice automation strategies, can reduce these risks. Specifically, look for tools that handle three functions well:
Pabau’s structured clinical documentation — digital intake and consent forms, plus treatment-note templates — helps home-visit providers capture MDM detail and time attestations consistently at the point of care, so the note supports whichever selection pathway gets billed. Combined with automated workflows, practices can cut the manual handoffs that cause CPT code 99350 errors without adding administrative headcount.
Pabau doesn’t submit US Medicare claims itself — its claims-management tools are built around Healthcode for UK private-insurance billing — but the documentation it captures is exactly what a biller needs to support a compliant 99350 claim, whichever system processes it.
For practices exploring these options, the AAPC Codify CPT lookup also provides coding guidance and crosswalk tools that complement billing software workflows.
CPT code 99350 is the highest-intensity established-patient home visit code in the series, and it demands the most rigorous documentation. The two most preventable failures are missing time attestations and MDM notes that state complexity without supporting it.
Practices billing home visit codes regularly benefit from structured documentation workflows that enforce compliance at the point of care, an area worth building into any practice business plan. Pabau’s built-in clinical forms and documentation tools are designed to capture exactly the data that supports a compliant 99350 claim.
To see how it works in practice, book a demo with the Pabau team.
Need a compliance overview for your home visit practice? HIPAA compliance guide covers the documentation and data security requirements that affect home-based clinical operations.
Managing billing across multiple clinicians or locations? Multi-location practice management outlines the workflow controls that keep billing consistent when clinicians operate across sites.
Want to understand how practice management tools reduce claim errors? Simplifying practice management explains how integrated software tightens the documentation and billing workflow behind fewer denials.
CPT code 99350 is used to bill home or residence visits for established patients requiring high complexity medical decision making, or total time of 60 minutes or more on the date of service (there’s no upper cap). It applies to patients who are unstable, have a significant new problem requiring additional workup, or are receiving terminal care.
CPT 99349 requires moderate complexity MDM or 40 minutes or more of total time; CPT 99350 requires high complexity MDM or 60 minutes or more. Both time thresholds are open-ended minimums, not ranges. The distinction is the MDM level: a stable patient with routine chronic disease management typically supports 99349, while an unstable patient or one requiring a hospitalization decision supports 99350.
Yes. When total time on the date of service reaches 60 minutes or more, a clinician may select CPT code 99350 based on time rather than MDM — there’s no upper limit on the base code, though time well beyond 60 minutes should be reported separately using a prolonged-services add-on code (CPT +99417, or HCPCS G0318 for Medicare once total time reaches 110 minutes or more). The note must include an explicit attestation of the total time spent and a description of the activities, including pre- and post-encounter work performed on the same date. Travel time doesn’t count toward the total.
Use POS 12 for visits in a patient’s private home and POS 14 for visits at an assisted living facility or group home. Using the wrong POS code is a common billing error that can result in overpayment recovery requests from Medicare Administrative Contractors.
The 2026 national average Medicare non-facility rate for CPT code 99350 is approximately $193, based on a total non-facility RVU of about 5.78 and the 2026 conversion factor of roughly $33.40-$33.57. The exact rate varies by MAC jurisdiction and geographic locality, so verify it using the CMS Physician Fee Schedule lookup tool or a current RVU calculator.
Commonly paired ICD-10-CM codes include I50.9 (heart failure), J44.1 (COPD with acute exacerbation), E11.65 (type 2 diabetes with hyperglycemia), and Z51.5 (encounter for palliative care). The diagnosis should reflect the condition driving the high complexity of the visit, not simply a background chronic condition.