CPT Code 00147: Anesthesia for iridectomy billing guide 2026
CPT Code 00147 covers anesthesia for iridectomy: base units, 2026 Medicare rates...
July 24, 2026
CPT code 99305 covers an initial nursing facility E/M visit requiring moderate medical decision making (MDM) or at least 35 minutes of total time on the date of encounter.
Post-2023 AMA guidelines eliminated mandatory history and physical exam components as level-determining factors; MDM complexity or documented time now solely determines code selection.
99304-99310 may each only be reported once per day, per beneficiary, per provider, per CMS RAC Topic 0061, making duplicate billing a top audit trigger.
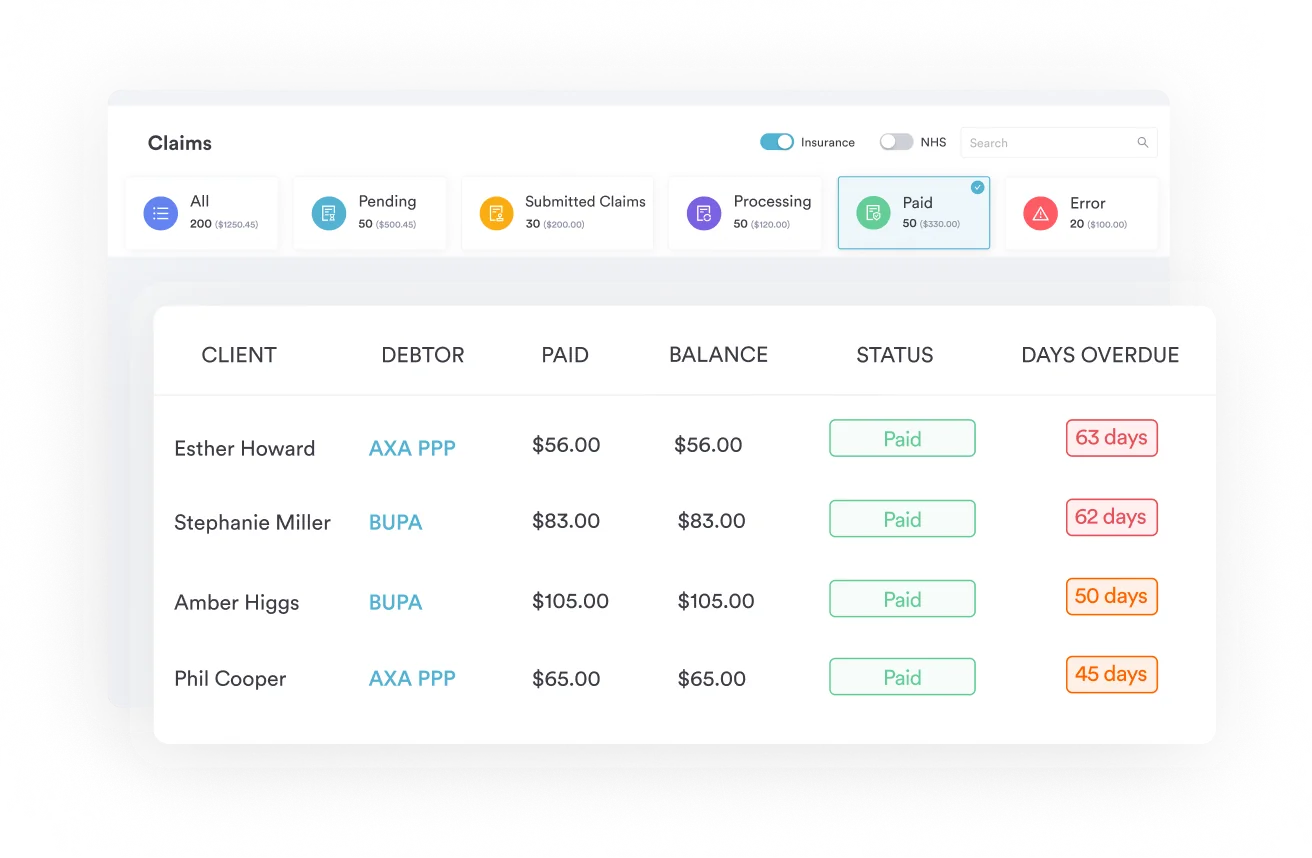
Pabau’s claims management software supports structured nursing facility E/M documentation and billing workflows to reduce claim errors and denial risk.
CPT code 99305 reports initial nursing facility care, per day, for a patient requiring moderate-complexity medical decision making or at least 35 minutes of total time on the encounter date. It applies to new and established patients seen for the first time in a nursing facility, and may be billed only once per day.
Most nursing facility billing denials trace back to a single problem: documentation that doesn’t support the code selected. CPT code 99305 is one of the most audited codes in the initial nursing facility care family, and getting the level wrong in either direction costs practices real money.
The American Medical Association (AMA) defines CPT code 99305 as: Initial nursing facility care, per day, for the evaluation and management of a patient, which requires moderate medical decision making or 35 minutes total time on the date of the encounter. It applies to both new and established patients being seen for the first time in a nursing facility setting.
This article covers the documentation requirements, MDM criteria, time thresholds, code comparisons (99304/99305/99306), reimbursement benchmarks, and the billing errors that trigger Recovery Audit Contractor (RAC) reviews. Use this reference to reduce denials and stay audit-ready for initial nursing facility E/M visits.
Since January 2023, the AMA’s updated E/M guidelines for nursing facility codes no longer require a comprehensive history and physical exam as level-determining components. What matters now is either the complexity of medical decision making or the total time spent on the encounter date.
That said, documentation must still support the MDM or time claim you’re making. Sparse notes with no clinical reasoning do not justify 99305, even if you spent 35 minutes with the patient.
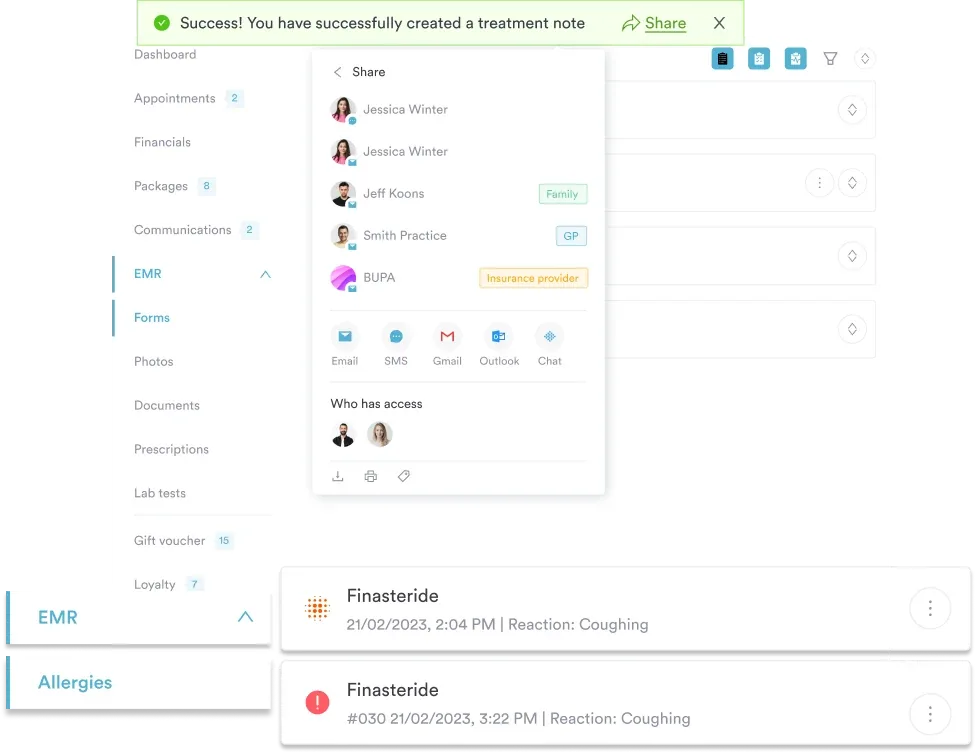
Maintaining HIPAA-compliant clinical documentation at nursing facilities requires structured note templates that capture each of these elements consistently. Many billing errors originate from incomplete templates, not from intentional miscoding.
Medical decision making for 99305 must reach the moderate threshold across all three MDM components. Two of the three components must meet or exceed moderate complexity. One component falling below moderate does not automatically disqualify the code if the other two components clearly support it.
The AAFP’s E/M time and MDM reference tables provide a useful summary of the exact thresholds for each level across the nursing facility code set.
Copying and pasting prior notes: Clone-and-carry documentation is a top RAC audit finding. The MDM must reflect what was clinically assessed on that specific encounter date.
Documenting time without detailing activities: If you’re billing on time, noting “35 minutes” alone is insufficient. The note should describe what that time included, such as reviewing outside records, coordinating with family, and updating the care plan.
Underdocumenting prescription drug management: Initiating or adjusting a prescription medication is a moderate-risk MDM element. If you adjusted a resident’s hypertension regimen or started a new psychotropic, document that decision explicitly. It’s the clearest path to moderate MDM for many nursing facility encounters.
Review your initial nursing facility notes against the AMA’s two-of-three MDM rule before submitting the claim. Document each MDM element separately in the note, not as a single narrative paragraph. Structured documentation using a template cuts review time and makes audit defense straightforward.
Under post-2023 AMA guidelines, providers may bill 99305 on time alone when the total time on the date of encounter reaches 35 minutes. Time includes face-to-face time with the patient and family, plus non-face-to-face time on the same date: reviewing records before the visit, documenting the note, ordering tests, and coordinating care.
Time and MDM are alternative pathways, not additive requirements. Choose the one that better supports the clinical encounter. If your visit involved complex prescription changes for a patient with unstable diabetes and heart failure, MDM will almost always be easier to document and defend.
Using structured documentation workflows at the point of care reduces the risk of time being undercounted or MDM elements being omitted. Practices that rely on narrative-only notes consistently underdocument time-intensive activities that would justify a higher-level code.
The three initial nursing facility care codes share the same clinical setting and patient population. What separates them is the complexity of the encounter, measured through MDM or total time.
Pabau's claims management software gives your team structured documentation templates, automated claim workflows, and audit-ready records for nursing facility E/M visits.

Use 99304 when the encounter involves a patient with stable, well-controlled chronic conditions requiring minimal clinical decision-making. The time threshold is 25 minutes. A common scenario: a new resident admitted from home with controlled hypertension and type 2 diabetes, no acute concerns, and a straightforward medication review.
Use 99305 when the encounter involves one or more chronic conditions with exacerbation, a new problem with uncertain prognosis, or decisions requiring prescription drug management. The time threshold is 35 minutes. A typical 99305 scenario: a resident admitted with decompensated heart failure and cognitive decline, requiring review of outside cardiology records, adjustment of diuretics, and coordination with the facility nursing staff.
Use 99306 when the encounter involves high-complexity MDM or 45 minutes of total time. High complexity means at least one acute or chronic illness posing a threat to life or bodily function, or decisions involving drug therapy requiring intensive monitoring. A 99306 scenario: a resident admitted post-stroke with aspiration pneumonia, hemodynamic instability, and a decision to initiate IV antibiotics and implement comfort care orders.
The most common upcoding error seen in RAC reviews is billing 99306 for encounters that clearly meet 99305 criteria. The second most common: billing 99305 when the resident is stable enough that 99304 is the correct code. Both directions carry audit risk. The AAPC Codify CPT code lookup provides the official code descriptors and guidelines for the full 99304-99306 range.
Medicare reimbursement for CPT code 99305 varies by geographic region, facility type, and the Medicare Physician Fee Schedule (MPFS) applicable to the calendar year. National average non-facility reimbursement rates in recent years have typically ranged from approximately $115 to $140 per encounter, though locality-adjusted rates can differ significantly.
Use the CMS Physician Fee Schedule lookup to find the exact rate for your MAC jurisdiction and the current calendar year. Always verify against the current year’s MPFS before quoting rates to billing staff, because both RVU values and conversion factors change annually.
The FastRVU 2026 RVU lookup tool provides current Work, Practice Expense, and Malpractice RVU components for 99305, which you can apply to your locality’s geographic adjustment factors (GAFs) for a precise estimate.
CPT 99305 is reported with Place of Service (POS) code 32 for skilled nursing facilities (SNFs) or POS 54 for custodial care facilities. The facility rate applies when the practice expense component is covered by the facility, which is typically the case in SNFs. Using the wrong POS code reduces reimbursement and triggers edit rejections from Medicare Administrative Contractors (MACs).
Medicaid rates for 99305 vary considerably by state and managed care plan. Some state Medicaid programs follow MPFS percentages (often 80-90% of Medicare rates), while others use fee-for-service schedules that may be substantially lower. Billing staff working across state lines should maintain separate fee schedule references for each state’s Medicaid program. Building these into your time-saving clinical workflows prevents repeated lookups during the billing cycle.
Pull your practice’s 99305 allowed amounts directly from your Medicare remittance advice for the past 12 months. Compare against the current MPFS for your locality. Any consistent underpayment pattern could indicate POS coding errors or modifier omissions worth reviewing before next submission cycle.
The modifier most often relevant to CPT 99305 is modifier AI (Principal Physician of Record). The admitting or attending physician appends modifier AI to the initial nursing facility care code (99304–99306) to identify themselves as the clinician overseeing the patient’s overall care. Every other physician who performs an initial evaluation on the same patient reports their E/M code without modifier AI to signal specialty care.
Modifier AI is informational and does not change the allowed amount for 99305. However, if the principal physician omits it, a Medicare Administrative Contractor (MAC) may deny same-date initial E/M claims from other specialties, because the system cannot distinguish the attending physician from consultants. Correcting this usually requires resubmission or a claim reopening to append the modifier. This guidance follows CMS Medicare Claims Processing Manual (IOM Pub. 100-04, Ch. 12) and MAC instruction (Noridian).
For a 99305 furnished by synchronous audio-video telehealth where the payer permits it, append modifier 95 and report the telehealth place-of-service code (POS 02 or 10) rather than the standard nursing facility POS. Initial-visit telehealth coverage varies, so confirm the current policy with the specific payer before billing.
CMS RAC Topic 0061 identifies nursing facility services as a high-risk area for excessive units. Per official CMS guidance, CPT codes 99304 through 99310 may each be reported only once per day, per beneficiary, per provider, per date of service. Billing any of these codes more than once on the same date is an automatic overpayment and a RAC priority target.
Practices using claims management software with built-in claim edits catch many of these errors before submission. A pre-submission scrub that flags duplicate dates, POS mismatches, and missing care plan indicators significantly reduces denials for SNF billing. Pairing this with digital intake forms that capture MDM elements at the point of care creates an audit-defensible documentation trail from the first encounter.
When a 99305 encounter extends significantly beyond the 35-minute threshold, prolonged service add-on codes may be billable. According to CMS Manual System Transmittal R1489CP, CPT codes 99356 and 99357 may be billed with nursing facility services including 99305.
99356 covers the first 30 minutes of prolonged face-to-face service beyond the base code’s time range, and 99357 covers each additional 30-minute increment. These add-on codes require clear documentation of the additional time and the reason the encounter extended beyond typical duration.
After the initial encounter billed with 99304-99306, follow-up visits are coded with the subsequent nursing facility care series. The 2023 coding changes also deleted CPT 99318 (the annual nursing home exam code) and rolled annual exams into the subsequent visit codes 99307-99310. Practices still using 99318 in their charge capture workflows are submitting an invalid code.
Managing the transition from initial to subsequent care codes across a nursing facility patient panel requires clinical records that clearly flag encounter type and track previous billing dates. Miscoding a subsequent visit as an initial visit (99305 instead of 99307-99310) is another common compliance error. Your practice management software should flag when an initial code is submitted for a patient who already has an encounter on record at the same facility.
For practices managing patients across multiple facilities, mental health practice management tools that support multi-location tracking help ensure the right encounter type is selected regardless of which facility the visit occurs at. Encounter-type logic should be built into your billing workflow, not left to individual coder judgment.
CPT code 99305 billing errors almost always trace back to two root causes: documentation that doesn’t clearly support moderate MDM, and charge capture workflows that don’t enforce encounter-type logic. Both are process problems, not clinical ones.
Pabau’s automated billing workflows and structured clinical record templates give nursing facility billing teams the tools to capture MDM elements at the point of care, apply the correct code, and submit clean claims the first time. To see how Pabau supports nursing facility E/M billing, review our primary care compliance resources or book a demo to walk through the claims workflow directly.
Need a full nursing facility compliance checklist? ADHD screening CPT code billing guide covers parallel E/M documentation standards you can adapt for nursing facility workflows.
Looking for structured billing workflows for your team? HIPAA compliance for medical offices explains documentation retention and audit-readiness requirements that apply to nursing facility E/M records.
Want to reduce claim denials across your practice? Pabau’s claims management software helps practices submit cleaner claims with built-in code edits and documentation prompts.
CPT code 99305 bills an initial E/M visit in a nursing facility requiring moderate medical decision making or at least 35 minutes of total time on the encounter date. It applies to both new and established patients seen for the first time at a nursing facility.
All three cover initial nursing facility care but differ by complexity: 99304 requires low-complexity MDM or 25 minutes; 99305 requires moderate-complexity MDM or 35 minutes; 99306 requires high-complexity MDM or 45 minutes. MDM is determined by problem severity, data reviewed, and risk of complications.
At least 35 minutes of total time on the encounter date, including both face-to-face and non-face-to-face time such as reviewing records, coordinating care, and completing documentation.
No. Per CMS RAC Topic 0061, codes 99304–99310 may only be reported once per day, per beneficiary, per provider. Billing 99305 twice on the same date is an overpayment and a flagged audit trigger.
Documentation must support moderate MDM across at least two of three MDM elements (problem complexity, data reviewed, risk of complications), or document a minimum of 35 total minutes of clinician time. A care plan is also required.
National average Medicare reimbursement typically ranges from $115 to $140 per encounter at the facility rate, varying by MAC locality and the current MPFS conversion factor. Use the CMS Physician Fee Schedule lookup or FastRVU for current figures.