HCPCS code A4210: Needle-free injection device billing guide 2026
HCPCS code A4210 is the Level II supply code for a needle-free injection device,...
July 21, 2026
CPT Code 97165 describes a low complexity occupational therapy evaluation, introduced in January 2017 to replace the retired CPT code 97003.
Documentation must include an occupational profile, medical and therapy history, and performance analysis using low complexity medical decision-making.
97165 is commonly billed alongside modifier GO to indicate occupational therapy services under a Medicare Part B therapy plan of care.
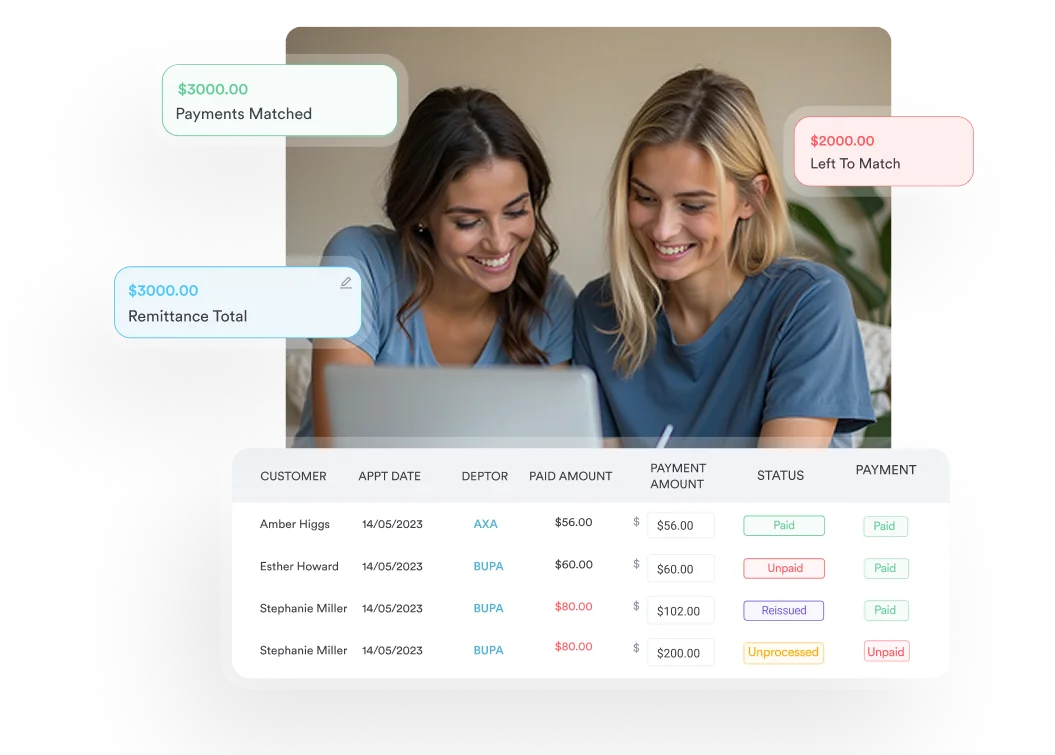
Pabau’s claims management software helps occupational therapy practices track documentation requirements, submit claims, and reduce denial rates across payer types.
CPT code 97165 is the billing code for a low complexity occupational therapy evaluation. It applies when a patient presents with one to three performance deficits, no comorbid conditions affecting occupational performance, and low complexity clinical decision-making. The evaluation typically takes about 30 minutes face-to-face and is reported once per episode.
This guide covers the 97165 CPT code description, the three documentation components payers expect, the modifiers to append, and how Medicare reimbursement works, so evaluations get coded correctly the first time and denials stay low.
Official descriptor (AMA CPT Manual): “Occupational therapy evaluation, low complexity, requiring these components: An occupational profile and medical and therapy history, which includes a brief history including review of medical and/or therapy records and client/patient/caregiver interview; an assessment(s) that identifies 1-3 performance deficits (i.e., relating to physical, cognitive, or psychosocial skills) that result in activity limitations and/or participation restrictions; and clinical decision making of low complexity, which includes an analysis of the occupational profile, analysis of data from problem-focused assessment(s), and consideration of a limited number of treatment options. Patient presents with no comorbid conditions that affect occupational performance. Typically, 30 minutes are spent face-to-face with the patient and/or family.”
CPT Code 97165 falls under the Physical Medicine and Rehabilitation Evaluations subsection of the American Medical Association’s CPT code set. It is one of three complexity-tiered OT evaluation codes (97165, 97166, 97167) introduced on January 1, 2017, replacing the previously retired CPT code 97003. A fourth code, 97168 (OT re-evaluation), completes the set for follow-up assessments when significant changes occur during a plan of care.
Practices billing OT evaluations for occupational therapy software users will recognize this code as the entry point for straightforward cases: patients presenting with one to three performance deficits, no comorbid conditions affecting occupational performance, and straightforward clinical decision-making.
Selecting the wrong complexity tier is one of the most common audit triggers in OT billing. The three evaluation codes share the same structural components but differ on the number of performance deficits identified, the presence of comorbidities, and the level of clinical decision-making required.
The time components listed above are typical, not mandatory. The code selection must be driven by the documented clinical components, not by time alone. Billing CPT Code 97165 because an evaluation happened to last 30 minutes, without meeting all three required documentation components, will not withstand a payer audit.
For practices also billing physical therapy evaluations, note that PT uses a parallel set (97161, 97162, 97163) with similar complexity tiers. The two sets are not interchangeable. Use the OT modifier GO (not the PT modifier GP) to distinguish OT claims from PT claims on the same date of service.
The three required components are non-negotiable. Missing even one is grounds for claim denial or post-payment audit recoupment.
This component requires a brief review of the patient’s medical and therapy records plus a client, patient, or caregiver interview. The therapist must document the patient’s occupational roles, meaningful activities, and how current deficits limit participation. A generic “patient reports difficulty with ADLs” entry does not satisfy this requirement. The documentation should name specific activities the patient values and connects deficits to those activities.
The evaluation must identify between one and three performance deficits across physical, cognitive, or psychosocial skill domains. These deficits must result in activity limitations or participation restrictions. Common assessments used in low complexity evaluations include manual muscle testing, range of motion measurements, standardized ADL screens such as the Katz Index of Independence in Activities of Daily Living or the Barthel Index, and basic cognitive screening tools like the Mini-Mental State Examination.
If the evaluating therapist identifies four or more deficits during what was expected to be a low complexity encounter, the documentation and billing should reflect 97166 (moderate complexity) rather than 97165. The number of identified deficits drives the code selection.
Clinical decision-making for CPT Code 97165 involves analyzing the occupational profile, interpreting data from the problem-focused assessments, and considering a limited number of treatment options. The patient must present with no comorbid conditions that affect occupational performance. A patient with a single diagnosis (such as a post-surgical shoulder repair with no secondary conditions) typically qualifies for low complexity.
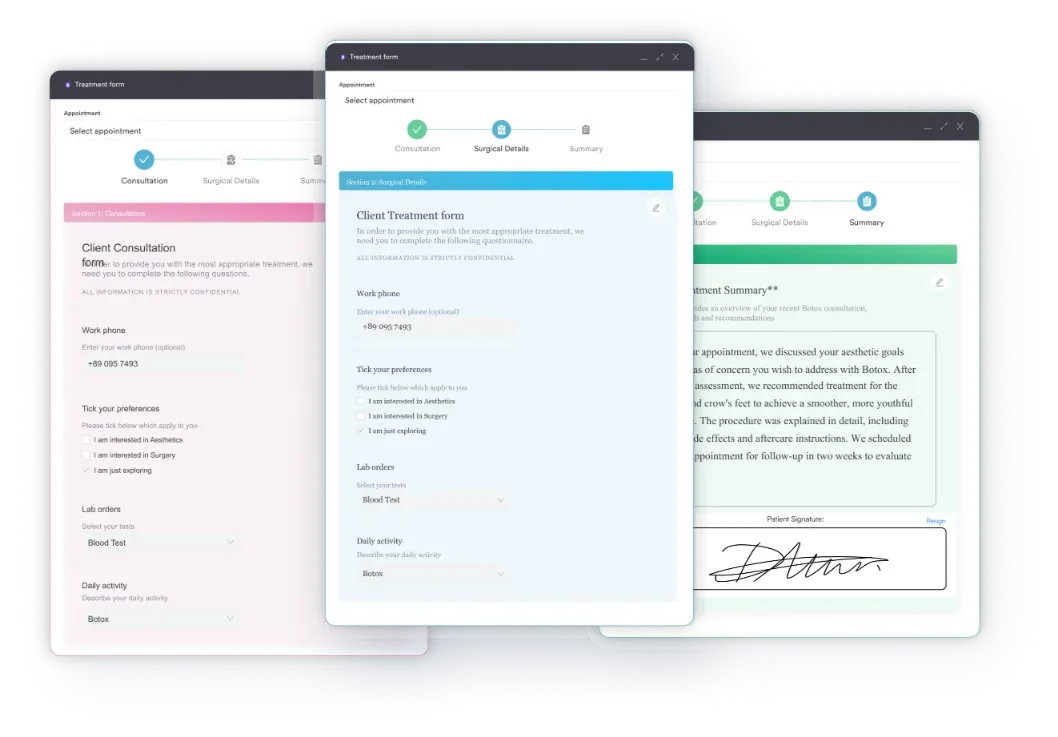
Good digital intake forms capture this information before the therapist enters the room, reducing documentation burden and helping ensure all three components are addressed systematically during every evaluation.
Before submitting a 97165 claim, run a three-point documentation check: (1) Is the occupational profile documented with named activities and interview findings? (2) Are exactly 1-3 performance deficits identified and linked to participation restrictions? (3) Does the note confirm low complexity decision-making with no comorbidities affecting occupational performance? A five-minute review at this stage prevents weeks of denial management later.
Only a licensed occupational therapist (OT/OTR) may perform and bill CPT Code 97165. A Certified Occupational Therapy Assistant (COTA) cannot independently bill this code because initial evaluations require the professional judgment of a licensed OT.
Under Medicare Part B, COTAs may assist with portions of the evaluation but the supervising OT must be present, involved, and responsible for the documentation. Some commercial payers and state Medicaid programs have different supervision requirements, so verify with each payer’s provider manual before assuming Medicare rules apply universally.
This is a documented compliance risk area. Practices with mixed OT/COTA staffing need clear internal policies on who performs evaluations, how supervision is documented, and which provider is listed on the claim. The therapy clinic compliance documentation framework is a useful reference for building those internal policies.
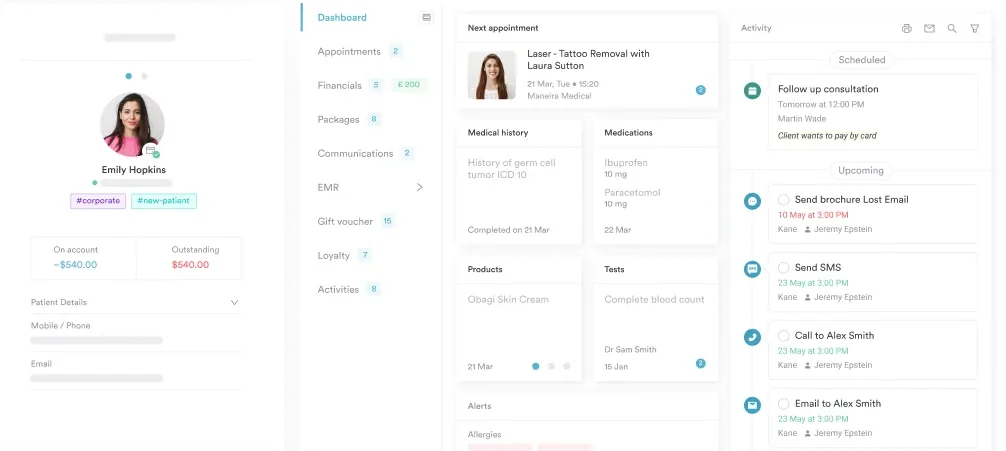
Pabau helps occupational therapy practices manage documentation, track claim status, and reduce administrative time. See how our claims management and digital forms features support accurate CPT coding.

Modifier usage with CPT Code 97165 is payer-specific, but several modifiers appear frequently across payer types.
State Medicaid programs and commercial payers may require additional or different modifiers. Always verify modifier requirements in each payer’s fee schedule before submitting. The claims management software built into Pabau allows practices to set payer-specific billing rules, reducing the risk of modifier errors on submission.
Medicare reimbursement for CPT Code 97165 varies by geographic location, as rates are adjusted by the CMS Geographic Practice Cost Index (GPCI). National averages change annually with each Medicare Physician Fee Schedule update. For current verified figures, use the CMS Physician Fee Schedule search tool and select the current calendar year.
As a general reference point, CPT Code 97165 has historically reimbursed in the range of $85-$115 under Medicare fee-for-service rates (non-facility), though practitioners should verify current rates directly with CMS before relying on any published figure. Commercial payers typically reimburse at a percentage of the Medicare fee schedule or at negotiated contracted rates, which vary by plan and geography.
Unlike timed treatment codes billed in 15-minute units, CPT Code 97165 is an untimed, service-based code. You report it once per evaluation episode regardless of whether the session runs 25 or 40 minutes, so the Medicare rate is a flat per-evaluation amount rather than a per-unit charge.
For practices tracking reimbursement trends across therapy clinic compliance requirements in multiple states, comparing fee schedule data regularly helps identify underpayments before they compound over a billing cycle.
Medicare covers CPT Code 97165 under the Part B outpatient therapy benefit, subject to the following conditions:
Maintenance therapy evaluations are covered under separate criteria. Do not bill CPT Code 97165 for maintenance-only visits without confirming medical necessity documentation meets skilled service thresholds.
Check your MAC (Medicare Administrative Contractor) for region-specific Local Coverage Determinations before billing 97165 for home health or outpatient settings. Noridian, CGS, and other MACs may publish additional guidance beyond the national CMS articles. Billing without consulting the applicable LCD is one of the most avoidable audit triggers in OT practice.
The AAPC’s Codify CPT reference and auditor reports consistently identify the same failure patterns in OT evaluation billing. These are the most frequent errors practices encounter with 97165.
Practices using therapy practice management software with built-in documentation templates can configure evaluation templates to prompt for all required 97165 components before the note is finalized. This prevents incomplete documentation from reaching the billing queue in the first place.
For broader context on how OT CPT codes fit into the larger therapy billing landscape, the OT Potential CPT guide covers practitioner perspectives on the full OT code set and common private-pay considerations.
CPT Code 97165 is used across multiple practice settings, but the billing rules shift depending on where the service is delivered.
Outpatient clinic: The standard setting for 97165. Facility and non-facility rate differences apply depending on whether the OT is employed by a hospital outpatient department or an independent private practice. Independent practices typically bill at the higher non-facility rate.
Home health: LCD L34560 governs Medicare coverage in this setting and includes additional documentation requirements beyond the standard 97165 criteria. The patient must meet homebound status criteria, and skilled service documentation is more strictly reviewed. Practices with home health programs should consult the applicable MAC guidance before billing CPT Code 97165 in this context.
Telehealth: Post-Public Health Emergency, CPT Code 97165 telehealth eligibility depends on the payer. CMS has expanded some telehealth flexibilities permanently, but occupational therapy evaluation codes are subject to ongoing policy review. Verify current telehealth eligibility with CMS and each commercial payer before billing 97165 for a remote encounter. Many commercial payers still require in-person presence for initial evaluations.
For practices running a therapy practice across multiple settings, maintaining a payer-specific billing matrix that tracks setting-level coverage rules for CPT Code 97165 prevents setting-based claim errors from compounding.
Practices looking to tighten their broader billing workflows can also review how other therapy CPT codes interact with evaluation codes under different payer structures, particularly when concurrent services are delivered on the same date.
Accurate client record documentation is the foundation of defensible billing across all settings. Every evaluation note should be written as if an auditor will review it, because occasionally one will.
Most CPT Code 97165 denials are preventable. The code is well-defined, the documentation components are clear, and the modifier requirements are consistent. The gap between knowing the rules and applying them systematically is where practices lose revenue.
Pabau’s claims management software helps occupational therapy practices build documentation workflows that capture all required evaluation components, apply the correct modifiers automatically, and track claim status from submission to payment. To see how it works for OT billing specifically, book a demo.
Looking to reduce claim errors across your billing workflow? Digital forms for therapy intake help capture evaluation components systematically before the therapist begins the assessment.
CPT Code 97165 is used to bill a low complexity occupational therapy evaluation that includes an occupational profile, medical and therapy history, and identification of 1-3 performance deficits with no comorbid conditions affecting occupational performance. It was introduced in January 2017, replacing the retired CPT code 97003, and falls under Physical Medicine and Rehabilitation Evaluations in the AMA CPT Manual.
The three codes differ by the number of performance deficits identified and the presence of comorbidities. CPT Code 97165 covers low complexity evaluations with 1-3 deficits and no comorbidities (typically 30 minutes). CPT 97166 covers moderate complexity with 3-5 deficits and 1-2 comorbidities (typically 45 minutes). CPT 97167 covers high complexity with 5 or more deficits and 3 or more comorbidities (typically 60 minutes). Code selection must be based on documented clinical complexity, not time spent.
Modifier GO is required for all Medicare OT claims, including CPT Code 97165, to identify the service as occupational therapy. Modifier KX is required when billing above the Medicare therapy cap threshold. Modifier 59 applies when 97165 is billed on the same date as another service that would otherwise be bundled. GP (physical therapy) and GN (speech-language pathology) are incorrect for OT claims and cause a claim reject.
No. A Certified Occupational Therapy Assistant (COTA) cannot independently bill CPT Code 97165. Initial OT evaluations require the clinical judgment of a licensed occupational therapist. Under Medicare Part B, a COTA may assist during the evaluation, but the supervising OT must be present, involved, and responsible for the documentation and claim submission. Rules may differ for commercial payers and state Medicaid programs.
Medicare reimbursement for CPT Code 97165 is set annually by the Medicare Physician Fee Schedule and varies by geographic location. Verify current rates using the CMS Physician Fee Schedule search tool for the applicable calendar year and your practice’s locality. Rates typically range from approximately $85 to $115 for non-facility settings, though actual amounts change each year and vary by region.
CPT Code 97165 has a typical face-to-face time of approximately 30 minutes, but time alone does not determine code selection. The code requires documentation of all three clinical components: occupational profile and history, performance analysis identifying 1-3 deficits, and low complexity clinical decision-making. A session shorter or longer than 30 minutes may still qualify for 97165 if the documented complexity level is low.
CPT Code 97165 is a service-based evaluation code, not a time-based one. You report it once per evaluation episode as a single unit, no matter how long the assessment takes. The 30-minute figure in the descriptor is a typical benchmark, not a billing threshold, and the code is never split into 15-minute increments the way therapeutic treatment codes are.