HCPCS code A4210: Needle-free injection device billing guide 2026
HCPCS code A4210 is the Level II supply code for a needle-free injection device,...
July 21, 2026
CPT code 96161 bills the administration of a caregiver-focused health risk assessment instrument (such as a depression inventory) for the benefit of the patient, with scoring and documentation, per standardized instrument. It is most often used for postpartum or caregiver depression screening at a pediatric well-baby visit, billed under the child’s patient ID. Billing is per completed instrument rather than by time, unlike time-based specialties such as anesthesia, where a charge builds from base and time units under CPT Code 00140 anesthesia guidelines.
CPT code 96161 covers administration of a caregiver-focused health risk assessment instrument, with scoring and documentation, per standardized instrument.
Billing is per instrument completed, not time-based. Practice expense must be incurred to administer the tool.
96161 differs from 96160 in one critical way: 96160 is patient-focused, while 96161 is caregiver-focused. Confusing the two is one of the most common denial triggers.
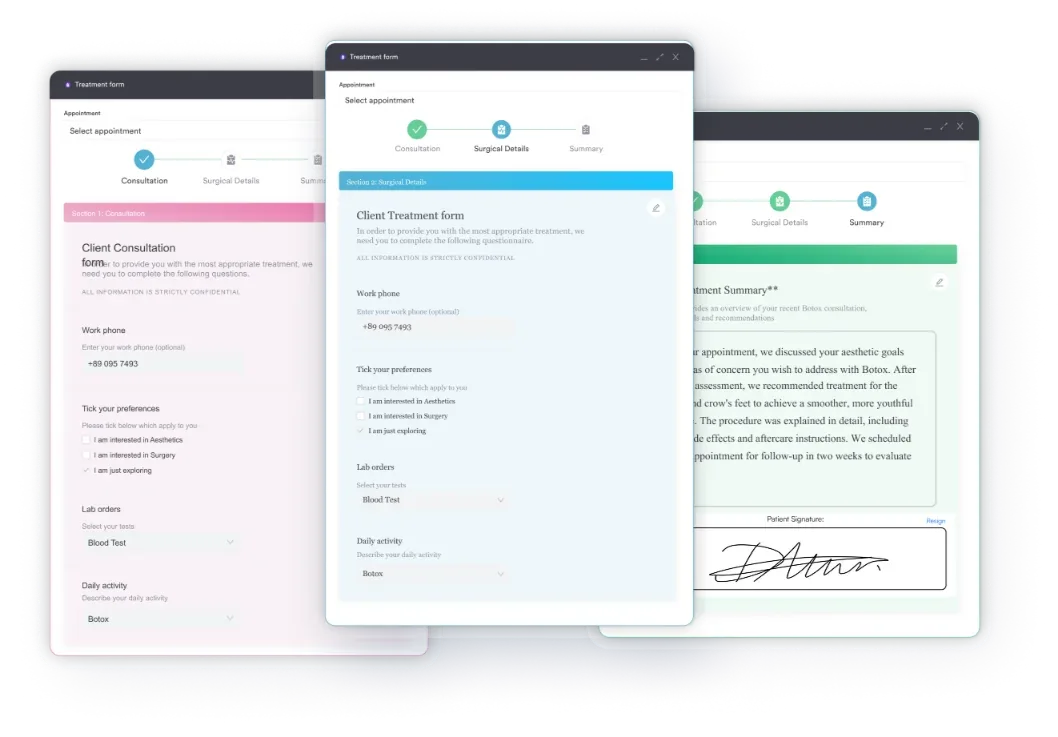
Pabau’s digital forms and claims management software help practices capture caregiver screening data, auto-populate scores, and submit 96161 claims without manual rework.
CPT code 96161 has the following official descriptor as defined by the American Medical Association (AMA) and referenced by the AAP and AAFP:
Administration of caregiver-focused health risk assessment instrument (eg, depression inventory) for the benefit of the patient, with scoring and documentation, per standardized instrument.
This code took effect January 1, 2017, replacing older coding structures that did not differentiate caregiver-completed assessments from patient-completed ones. The code applies when a clinician or qualified staff member administers a standardized tool to a caregiver (typically a parent, guardian, or primary caregiver), and the results are scored and documented as part of the patient’s care. The most common clinical context is maternal or caregiver depression screening at a well-child or well-baby visit.
Common instruments billed under this code include the Edinburgh Postnatal Depression Scale (EPDS), the Patient Health Questionnaire (PHQ-9 or PHQ-2) administered to a caregiver, and depression inventories completed by caregivers at pediatric visits. The Asthma Control Test (ACT), when completed by a caregiver on behalf of a pediatric patient, also falls within scope.
The difference between these two codes comes down to who completes the assessment. Mixing them up is a fast route to denials.
Both codes follow the same structural billing logic, but the respondent determines which one applies. A caregiver screening at a well-baby visit where the parent answers the questions is 96161, not 96160. Billing 96160 in that context misrepresents who completed the instrument and is a common audit flag. For practices that also screen adult patients, ADHD screening CPT codes follow a similar per-instrument billing logic and face analogous documentation requirements.
Incomplete documentation is the most common reason 96161 claims are denied or downcoded on audit. The code has specific requirements that go beyond simply noting that a screening occurred.
According to the AAPC Codify CPT reference, the following elements must be present in the medical record to support a valid 96161 claim:
Practices using paper forms that staff then manually enter into an EHR face the highest risk of documentation gaps. Structured patient intake and screening forms that auto-capture caregiver responses and timestamps reduce this risk and create an audit-ready record from the moment the caregiver completes the tool. Maintaining HIPAA-compliant documentation practices is especially important when caregiver mental health data is part of a child’s clinical file.
Document the specific instrument name, the numerical score, and the clinical response in every 96161 encounter note. Payers auditing this code look for all three elements. A note that says “depression screen administered” without a score or instrument name does not meet the documentation standard.
The most common clinical scenario for CPT code 96161 is postpartum or caregiver depression screening at a well-baby visit. This creates a billing nuance that confuses many practices: the service benefits the child (the patient), but the caregiver completes it. The claim goes under the child’s patient ID, not the caregiver’s.
According to guidance from the Centers for Medicare and Medicaid Services (CMS) coding resources and supporting AAFP clinical billing guidance, well-baby practices should observe these billing rules:
The EP modifier signals to Medicaid that the service was provided as part of an EPSDT preventive visit. Not all states require it, and commercial plans do not use it, but failing to append it where required is a denial trigger in those Medicaid plans. Verify the specific requirement with each state Medicaid plan where you practice. Pediatric and primary care practices running maternal depression screening programs benefit from automated clinical workflows that flag the appropriate modifier based on the patient’s insurance type at time of scheduling.
Bundling is one of the highest-risk areas for CPT code 96161 claims. Per the American Academy of Pediatrics (AAP) Coding News (April 2023), CPT code 96161 is bundled with CPT code 96110 (developmental screening with scoring and documentation) when both are billed on the same date of service.
CPT 96110 covers developmental milestone screening, such as the Ages and Stages Questionnaire (ASQ), administered to assess the child’s development. CPT 96161 covers a separate instrument administered to the caregiver about the caregiver’s own health. Despite being conceptually distinct, the NCCI (National Correct Coding Initiative) and AAP coding guidance treat them as bundled when billed together.
For practices working through high-volume pediatric schedules, practices involved in autism spectrum disorder ICD-10 coding and developmental screenings will encounter the 96110/96161 bundling question regularly. A claims management system that applies real-time NCCI edits before submission prevents the denial before it happens rather than requiring a corrected claim workflow afterward.
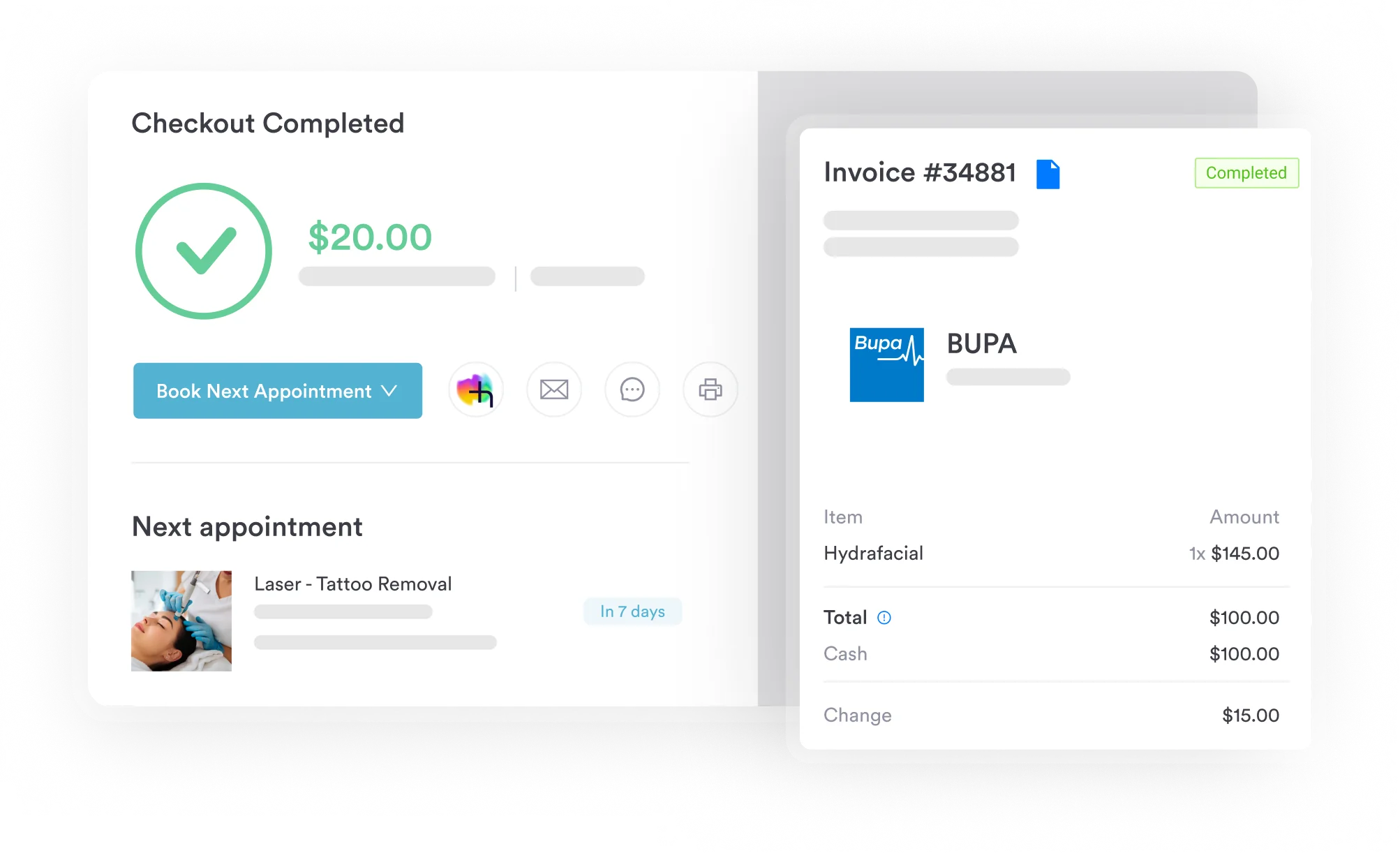
Pabau's claims management tools apply real-time coding rules and NCCI edits to flag bundling issues, missing modifiers, and incomplete documentation before submission. Fewer denials, less rework.

CPT code 96161 does not commonly require modifiers in most commercial billing contexts, but specific payer and program settings do require them. Using the wrong modifier (or omitting a required one) affects both reimbursement and audit risk.
The EP modifier warrants special attention. Some state Medicaid plans require it on all preventive services billed at EPSDT well-child visits, including 96161. Others do not. There is no universal rule, so practices billing across multiple state Medicaid plans need plan-specific modifier rules documented in their billing setup. Check state-specific Medicaid provider manuals or tip sheets before assuming EP is or is not required.
CPT code 96161 must be paired with an appropriate ICD-10-CM diagnosis code to support medical necessity. The correct diagnosis depends on the clinical context: screening of a caregiver with known risk factors differs from routine preventive screening at a well-child visit.
Verify current codes using the CDC/NCHS ICD-10-CM web tool for the current fiscal year. The following codes are commonly paired with 96161:
When screening is routine and preventive, Z-codes (Z13 series) are appropriate. When the caregiver has a confirmed or suspected diagnosis, use the specific depressive disorder or postpartum code. Many payers accept both on the same claim (Z-code as primary, F-code as secondary) when there is both a screening and a known condition. For practices managing screening workflows alongside anxiety and adjustment disorder ICD-10 codes, the same preventive vs diagnostic distinction applies and creates similar payer-specific variability.
When in doubt on ICD-10 pairing, default to the Z-code for screening (Z13.30 or Z13.89) as primary. If the screening returns a positive result and you document a clinical impression, add the specific depressive disorder code as secondary. Some payers require the specific diagnosis for reimbursement beyond the screening rate.
Reimbursement for CPT code 96161 varies by payer, geographic locality, and whether the service is classified as preventive or diagnostic. The CMS Physician Fee Schedule lookup tool provides the Medicare facility and non-facility rates for this code by locality. Always verify current rates before assuming reimbursement levels from previous years.
General reimbursement context for CPT code 96161:
For practices using claims management software, attaching the correct fee schedule rate to 96161 claims and flagging payer-specific rules at the point of claim creation reduces preventable underpayments and denials. Practices offering wellness services alongside preventive screening benefit from reviewing health and wellness coaching CPT codes, where similar preventive vs diagnostic classification issues arise.
CPT code 96161 faces more payer variability than most screening codes because it sits at the intersection of pediatric care, maternal mental health, and preventive benefits. The most common denial patterns and their causes:
Practices operating across multiple states or payer types need a payer-rule reference that is updated annually. For mental health practice management, the same payer-specific documentation and modifier requirements apply across the screening code family and benefit from a centralized billing rule reference within the practice management system.
Here is how the rules above come together in a common scenario: a mother completes the Edinburgh Postnatal Depression Scale (EPDS) at her infant’s well-baby visit. The steps below follow the documentation, ICD-10, bundling, and modifier rules described earlier in this guide.
No reimbursement figures are assumed here: confirm the current locality-adjusted rate through the CMS Physician Fee Schedule lookup and each payer’s policy before submitting the claim.
CPT code 96161 is a billing tool for a specific and clinically meaningful service: screening a caregiver’s health, for the benefit of the patient, using a standardized instrument. Getting the code right requires understanding who completes the tool, whose ID it bills under, what modifiers apply by payer, and how it interacts with codes like 96110. These are not complex rules once they are documented and built into a practice’s billing workflow.
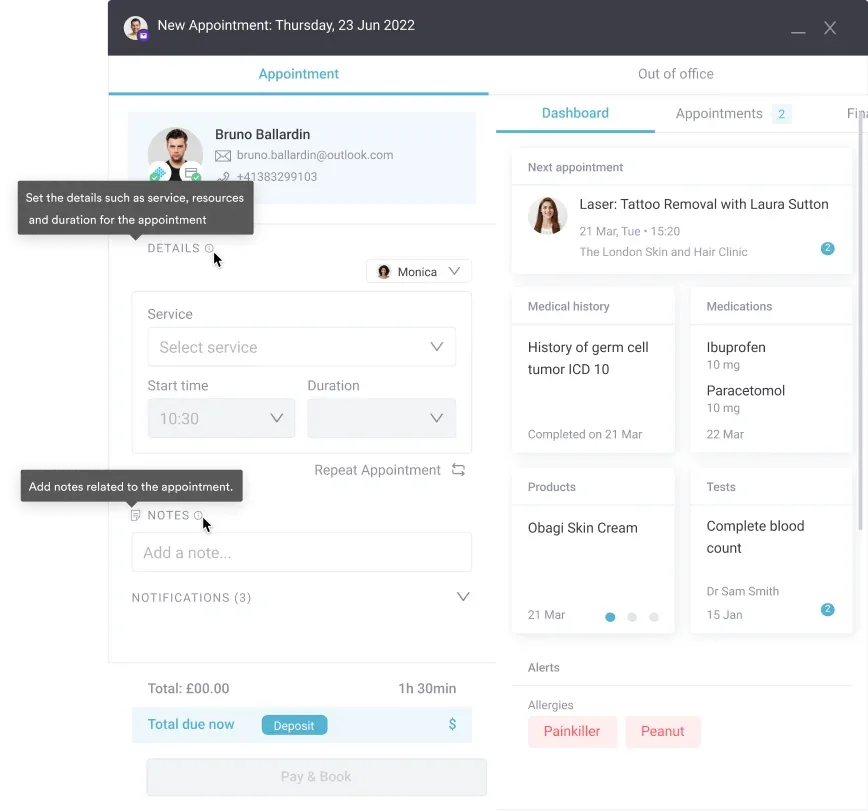
Pabau’s medical record management and digital forms tools help practices capture caregiver screening data at the point of care, with structured scoring fields that meet documentation standards for 96161 out of the box. To see how Pabau handles preventive screening documentation and claim submission workflows, book a demo.
Need a reference for related neurological and behavioral ICD-10 codes? Intraparenchymal hemorrhage ICD-10 codes walks through the neurological code family structure for clinical reference.
Managing preventive care CPT codes across multiple service lines? IVF CPT codes covers another preventive and specialty care code set with similar documentation and payer complexity.
Looking for a mental health and behavioral health EMR that supports screening workflows? Mental health practice management software from Pabau supports structured screening, documentation, and billing in one platform.
CPT code 96161 is used to bill for the administration of a caregiver-focused health risk assessment instrument, with scoring and documentation, per standardized instrument. The most common use is postpartum or caregiver depression screening at a pediatric well-baby or well-child visit, where a parent or guardian completes the screening tool for the benefit of the child.
CPT 96160 is completed by the patient; CPT 96161 is completed by the caregiver. Both codes cover health risk assessment instrument administration with scoring and documentation, but 96161 specifically applies when a parent, guardian, or caregiver answers the questions on behalf of the patient, and the results are for the patient’s benefit.
Yes. Many Medicaid plans specifically support 96161 for postpartum depression screening at well-baby visits. The claim must be billed under the child’s patient ID, not the caregiver’s. Some state Medicaid plans allow up to six screenings before the child reaches 13 months of age. Coverage under commercial plans varies by payer.
The EP modifier is used when billing 96161 at an EPSDT (Medicaid well-child) visit, but only where the state Medicaid plan specifically requires it. Not all states mandate EP for this code. Modifier 25 may be appended to a same-day E&M code (not to 96161 itself) when a significant, separately identifiable evaluation and management service was also provided.
The AMA’s CPT descriptor for 96161 does not specify an age limit for the patient. The code applies any time a caregiver completes a standardized health risk assessment for the patient’s benefit. Individual payer policies may impose age restrictions, so verify coverage with each payer for patients outside the typical well-child visit age range.
For Medicare, G0444 is the code used for annual depression screening of the patient; 96161 is caregiver-focused and its Medicare coverage should be verified with the relevant Medicare Administrative Contractor. For Medicaid, coverage varies by state plan but many have adopted 96161 for postpartum depression screening at well-baby visits, with varying frequency limits. Always verify current rates using the CMS Physician Fee Schedule lookup.