CPT code 20551: Tendon injection billing, rates, and modifiers
CPT code 20551 covers one injection into a tendon origin or insertion. Medicare ...
Last Updated: August 6, 2026
CPT code 12034 covers intermediate repair of wounds on the scalp, axillae, trunk, and extremities (excluding hands and feet), measuring 7.6 cm to 12.5 cm.
Intermediate repair requires single-layer closure of heavily contaminated wounds or closure of deeper subcutaneous or non-percutaneous tissue layers – not just any multi-layer closure.
Multiple wounds in the same repair category and body region are added together for total length; failing to aggregate wound lengths is one of the most common audit triggers for this code.
Practice management software like Pabau links wound measurements, closure technique, and contamination notes to a structured, audit-ready patient record, reducing the documentation gaps that trigger CPT code 12034 errors.
CPT code 12034 covers intermediate repair of wounds on the scalp, axillae, trunk, or extremities measuring 7.6 cm to 12.5 cm. This guide breaks down the official descriptor, what separates intermediate repair from simple and complex closure, 2026 reimbursement rates, applicable modifiers, documentation requirements, the ICD-10 codes that support medical necessity, and the billing errors that trigger the most payer audits.
Claims submitted with the wrong repair-tier code are among the most common wound closure denials in emergency medicine, dermatology, and plastic surgery billing. CPT code 12034 sits at a precise intersection of repair technique, anatomic location, and wound size, and misidentifying any one of those three elements puts the claim at risk.
According to the American Medical Association (AMA) CPT code set, CPT code 12034 describes intermediate repair of wounds on the scalp, axillae, trunk, and/or extremities (excluding hands and feet) when the wound measures 7.6 cm to 12.5 cm.
The AMA’s official short descriptor reads: Repair, intermediate, wounds of scalp, axillae, trunk and/or extremities (excluding hands and feet); 7.6 cm to 12.5 cm. The table below breaks down each component.
Intermediate repair is not simply a two-layer closure. Rather, the AMA defines it as either (a) single-layer closure of a heavily contaminated wound requiring extensive cleaning, or (b) closure of one or more layers of subcutaneous tissue and non-percutaneous deep tissue in addition to the skin closure. In other words, a simple layered skin closure without subcutaneous involvement does not qualify.
Understanding where intermediate sits relative to simple and complex repair is critical for accurate code selection. For instance, misclassifying a simple repair as intermediate constitutes upcoding. Conversely, selecting a simple repair code when deeper tissue closure was performed results in undercoding and revenue loss.
Debridement of necrotic or infected tissue performed before closure is coded separately from the repair itself. For necrotizing soft tissue infections requiring excisional debridement, for example, CPT 11004 covers the debridement, while the repair – once the wound is clean and ready for closure – is billed under the appropriate 120XX code based on size and location.
CPT code 12034 applies to four qualifying body regions: the scalp, axillae, trunk, and extremities. Hands and feet, however, are explicitly excluded. For wounds on the hands, feet, face, ears, eyelids, nose, or lips, coders must use the 12041-12057 series instead.
Wound measurement follows AMA guidelines precisely. When a patient presents with multiple lacerations in the same repair category and the same body region, their lengths are added together to determine the single code that covers the total cumulative measurement. Two 4-cm intermediate repairs on the same patient’s trunk combine to 8 cm total, for example, placing the encounter squarely in the 12034 range. This cumulative measurement rule is one of the most commonly misapplied aspects of wound closure billing.
Reimbursement for CPT code 12034 varies by payer, geography, and facility type. The CMS MPFS lookup tool is the authoritative source for current Medicare allowable rates. Reference the tool annually, since the Medicare Physician Fee Schedule (MPFS) is updated each January.
Based on 2026 Medicare Physician Fee Schedule RVUs, the national non-facility payment for CPT code 12034 is approximately $320-$335 before locality adjustment, and the facility payment is approximately $175-$180. Verify the exact rate for your geographic area using the CMS MPFS lookup tool, since rates vary by Medicare Administrative Contractor (MAC) jurisdiction and are updated annually. Private payer rates are contractual and differ from Medicare allowables.
For a detailed RVU breakdown, FastRVU’s RVU lookup tool provides 2026 work, practice expense, and malpractice RVU components for CPT code 12034 using current CMS data.
Run the CMS MPFS lookup annually in January when the new fee schedule takes effect. Pull CPT 12034 rates for your MAC locality and update your charge master to reflect current allowables before submitting January claims.
Modifier selection for CPT code 12034 is payer-specific. The table below covers the most commonly used modifiers, but always verify applicability with individual payer policies before appending.
Modifier 25 attaches to the E&M code, not to CPT code 12034 itself. A common billing error is appending modifier 25 to the procedure code rather than the evaluation service. Review HIPAA-compliant documentation practices for guidance on maintaining the supporting records needed when modifier 25 is used.
Medical necessity documentation is the foundation of a defensible CPT code 12034 claim. This matters because payers audit wound repair codes closely — the line between repair tiers is defined by technique and contamination level, neither of which is visible on a claim form without supporting notes.
The operative or procedure note must include all of the following elements. Missing even one can trigger a denial or a request for additional documentation. To reduce that risk, consider using digital intake forms integrated with your clinical record to standardize these capture points at the point of care.
Good clinical documentation at the point of care is the single most effective way to prevent post-submission audits. Structured note templates that require mandatory field entry for wound measurement and repair technique eliminate the most common documentation gaps. For practices managing patient data security, ensuring those records are encrypted and access-controlled is an additional compliance requirement.
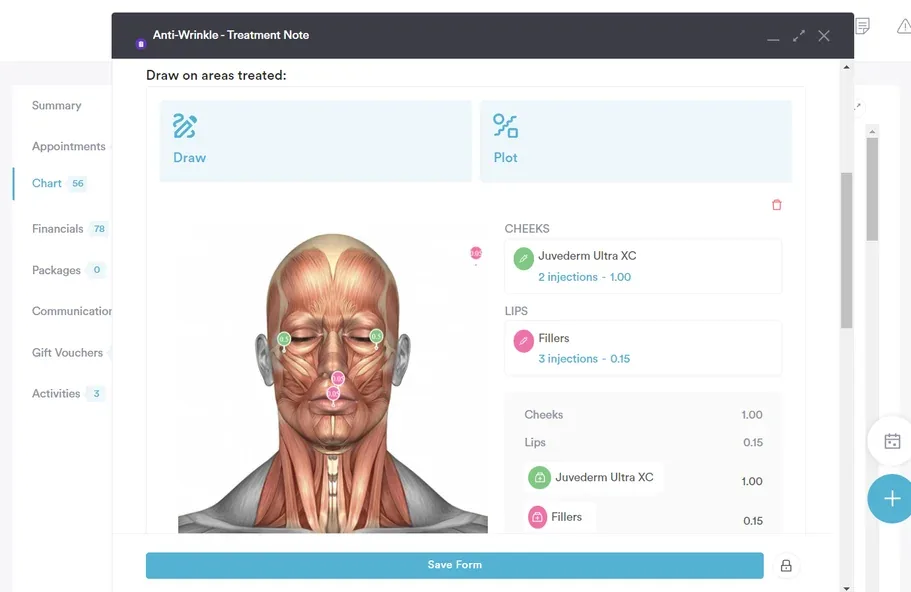
Pabau's structured clinical documentation captures wound measurements, repair techniques, and modifier logic in audit-ready fields linked to the patient record, so the details behind a CPT code 12034 claim are easy to find later.

A CPT claim without a supporting ICD-10 diagnosis code fails medical necessity review. The diagnosis code tells the payer why the repair was performed. For CPT code 12034, the most commonly paired ICD-10 codes are wound and laceration diagnoses matching the anatomic site reported. Diagnosis codes describing a sprain or strain, such as S93.619A, don’t support medical necessity for a repair code, since no open wound is present. Verify that your specific payer’s Local Coverage Determination (LCD) does not restrict coverage to a narrower diagnosis list.
Select the ICD-10 code that matches the specific anatomic site and wound type documented in your operative note. For practices that manage dermatology and wound care encounters, dermatology EMR software with integrated ICD-10 search can accelerate correct diagnosis pairing at the point of documentation. The AAPC’s CPT-to-ICD-10 crosswalk is a useful verification resource.
CPT code 12034 is part of the 12031-12037 intermediate repair series for the scalp, axillae, trunk, and extremities. Understanding where 12034 sits within the full intermediate repair ladder prevents both under- and over-coding. The same size-tiered logic shows up elsewhere in the integumentary system chapter – excision codes like CPT 11423 scale by lesion diameter the same way repair codes scale by wound length.
Wound repair codes generate a disproportionate share of payer audits relative to their reimbursement value. In most cases, errors fall into four recurring patterns.
Build a wound repair audit checklist into your post-visit charge entry workflow. Before submitting a 12034 claim, verify: (1) cumulative wound length recorded and meets 7.6-12.5 cm threshold, (2) anatomic location is scalp/axillae/trunk/extremity and not hands or feet, (3) documentation explicitly states subcutaneous closure or heavy contamination with cleaning, (4) modifier 25 is on the E&M code if billed same day.
The most common CPT code 12034 errors – wrong wound measurement, missing contamination documentation, incorrect modifier placement – are all documentation errors. They happen before the claim is built, not during submission. Practice management software that connects the clinical note directly to the billing workflow closes this gap.
Pabau’s structured clinical documentation links wound length, body location, closure layers, and contamination level to the patient record through dedicated note fields, so that detail stays attached to the encounter instead of living in a separate free-text note. Practices using Pabau also benefit from EHR integration that keeps clinical records and billing data in the same system, so the documentation that supports a CPT code 12034 claim is always retrievable during a payer audit.
For practices that handle HIPAA compliance requirements, Pabau’s documentation architecture maintains encrypted records with role-based access, supporting both audit readiness and HIPAA Security Rule obligations. Reviewing practice management software features that include wound documentation templates is a practical starting point for practices looking to tighten their wound repair billing accuracy.
CPT code 12034 has a narrow scope: intermediate repair, four qualifying body regions, and a precise 7.6-12.5 cm wound length window. The most expensive errors are not complex – they are a missed wound measurement aggregation, a vague contamination note, or modifier 25 on the wrong code line. Accurate documentation at the point of care is the fix for all of them.
Pabau’s structured clinical documentation keeps the wound repair note and the billing record built from the same data, so the detail that justifies the code is never more than a click away. To see how Pabau handles wound repair documentation and billing in practice, book a demo with the team.
Need the excision-side equivalent of a repair-tier code? CPT 11644 covers excision of a malignant lesion using the same size-tiered logic as the repair series.
Managing a wound that needs debridement before closure? CPT 11004 explains how necrotizing soft tissue debridement is coded separately from the repair itself.
Curious how ICD-10 specificity extends beyond open wounds? S93.619A shows the same site-and-laterality logic applied to a foot ligament sprain.
CPT code 12034 is an intermediate repair code for wounds on the scalp, axillae, trunk, and extremities (excluding hands and feet) measuring 7.6 cm to 12.5 cm. It applies when closure involves subcutaneous tissue layers or management of heavy contamination.
The qualifying range is 7.6 cm to 12.5 cm. When multiple wounds in the same repair category and body region are treated in one session, their lengths are added together to determine the correct code.
The most common modifiers are 25 (appended to the E&M code, not 12034), 51 (multiple procedures), and 59 (distinct procedural service). RT/LT may apply for bilateral specificity. Confirm all modifier use with individual payer policies.
All three are intermediate repair codes for the same body regions, differing only by wound length: 12032 covers 2.6–7.5 cm, 12034 covers 7.6–12.5 cm, and 12035 covers 12.6–20.0 cm.
The operative note must include the anatomic site, wound length in centimeters, contamination level and cleaning performed, and repair technique with layers closed and suture material. Vague notes without contamination or layer detail are the most common audit triggers.
Yes, when the E&M service was separately identifiable from the decision to perform the repair. Append modifier 25 to the E&M code — not to 12034 — and verify requirements with your payer.