








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT code 12001 covers simple repair of superficial wounds 2.5 cm or less on the scalp, neck, axillae, external genitalia, trunk, and extremities (including hands and feet).
Simple repair means one-layer closure involving only the epidermis, dermis, or subcutaneous tissue with no deeper structure involvement.
The global period is 000 (zero post-op days), so any E/M service on the same date requires Modifier -25 to be separately billable.
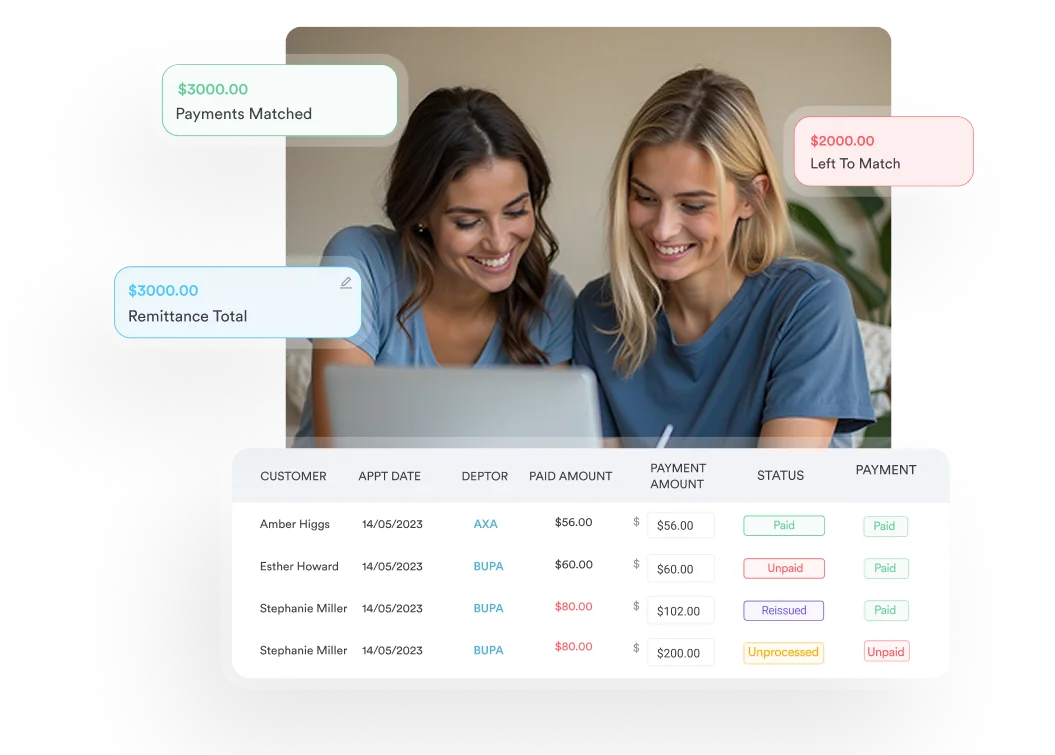
Pabau’s claims management software automates claim submission and flags modifier requirements, reducing denial rates for wound repair billing.
CPT code 12001 is the standard billing code for simple repair of superficial wounds measuring 2.5 cm or less on the scalp, neck, axillae, external genitalia, trunk, and extremities. It is one of the most frequently billed integumentary codes across primary care, urgent care, and emergency medicine settings.
This guide covers every element providers and billing staff need to submit clean 12001 claims — from documentation requirements and modifier rules to global period implications, Medicare reimbursement, and NCCI bundling edits.
CPT code 12001 is defined by the American Medical Association (AMA) as: “Simple repair of superficial wounds of scalp, neck, axillae, external genitalia, trunk and/or extremities (including hands and feet); 2.5 cm or less.”
It is the entry-level code in the simple repair series (12001–12021) and one of the most frequently billed integumentary codes across primary care, urgent care, and emergency medicine.
Skin practices and emergency departments billing 12001 see more documentation-driven denials than almost any other integumentary code, not because the repair was wrong, but because the record didn’t capture the measurement, anatomical site, or closure method in sufficient detail.
The classification “simple repair” has a specific clinical meaning in CPT guidelines. Three criteria must all be met before 12001 applies.
A wound that meets all three criteria but sits on the face, ears, eyelids, nose, lips, or mucous membranes does not qualify for 12001. Those anatomical sites fall under a separate code series (12011-12018), even when the repair is otherwise simple in nature. Coders billing those facial repairs should reference the ICD-10-CM facial laceration codes guide for the correct diagnosis pairing.
The AMA’s CPT guidelines are explicit that codes 12001-13160 “designate closure utilizing sutures, staples or tissue adhesive (e.g., 2-cyanoacrylate), either singly or in combination with each other, or in combination with adhesive strips.” This matters for practices that use Steri-Strips or tissue adhesive as the primary closure method.
Applying tissue adhesive alone to a qualifying wound still supports billing 12001 provided the wound meets the size and site criteria. Using only adhesive strips without any sutures, staples, or tissue adhesive does not support reporting a repair code; adhesive-strip-only closure is considered simple wound care.
Incomplete documentation is the leading cause of 12001 denials and audits. Every element below must appear in the procedural note before the claim is submitted. Using digital forms and structured note templates reduces the risk of missing fields at the point of care. Urgent care sites in particular benefit from a standardized urgent care doctor’s note template that prompts for wound measurement and closure method at the time of the visit.
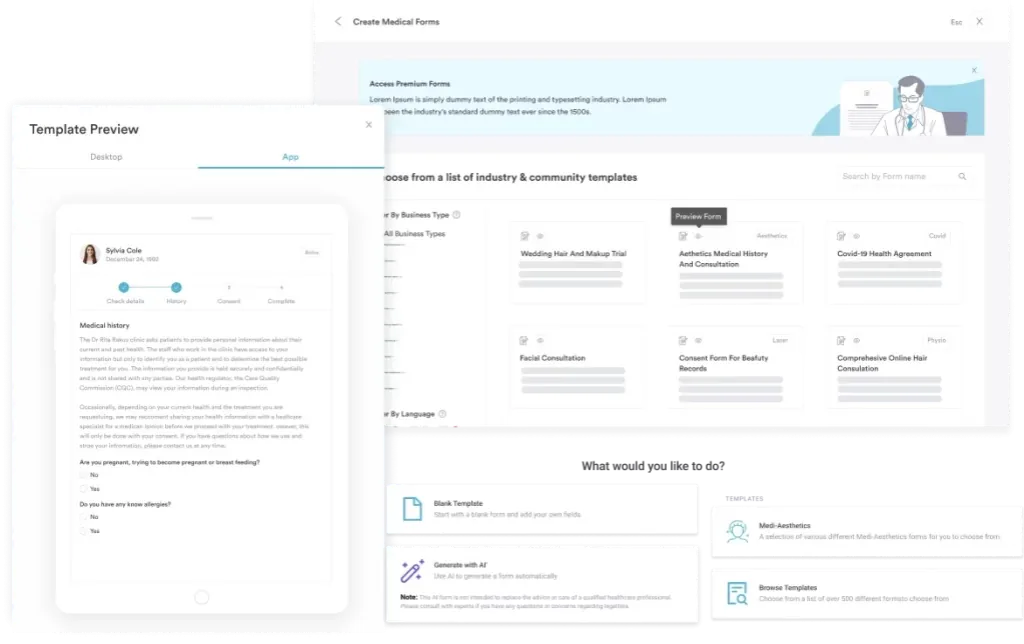
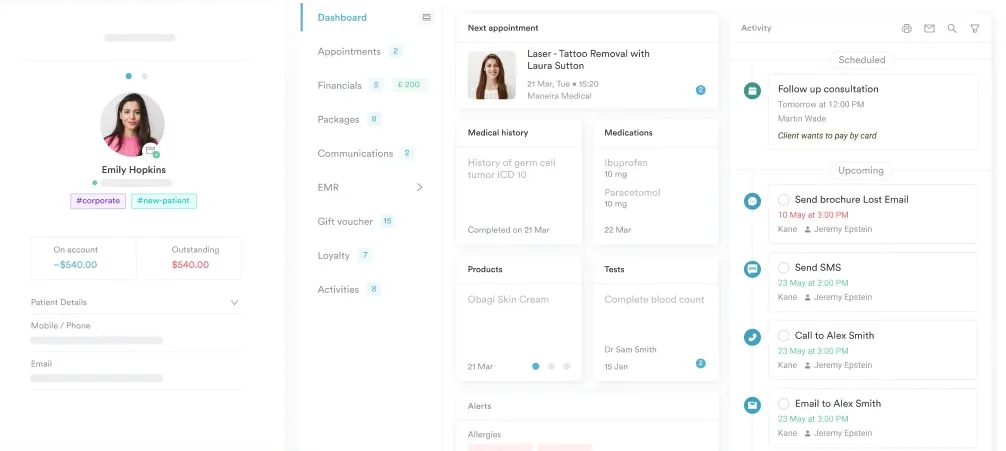
Maintaining structured client records with procedure-specific fields makes it far easier to produce complete documentation consistently across providers. Practices relying on free-text notes frequently miss the wound measurement or depth description, which are the two fields payers most commonly flag on audit.
Good clinical forms and documentation workflows built into the EHR make this a system problem rather than a provider behavior problem.
Using the wrong modifier (or omitting a required one) is one of the most common billing errors on wound repair claims. Three modifiers apply regularly to CPT code 12001.
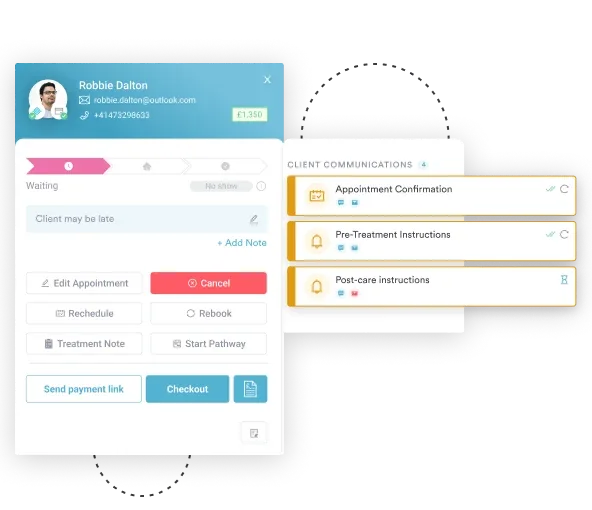
When a clinician performs an evaluation and management (E/M) service on the same date as a wound repair, Modifier -25 must be appended to the E/M code to demonstrate that the visit was a significant, separately identifiable service beyond the repair itself.
Without Modifier -25, payers will typically bundle the E/M into the procedure and deny it as part of the repair’s pre-service work. The clinical documentation must support that the E/M addressed a separate problem or a condition not related solely to the wound repair decision.
When CPT code 12001 is billed alongside another wound repair code on the same date (for example, 12001 for a simple scalp repair and 12032 for an intermediate extremity repair), the American College of Emergency Physicians (ACEP) confirms that Modifier -59 should be appended to the secondary procedure code to indicate the procedures are distinct and not a single service.
The higher-valued repair code is listed first without a modifier; the lower-valued code takes Modifier -59.
Modifier -51 signals that multiple procedures were performed during the same operative session. It applies when CPT code 12001 is reported alongside non-wound-repair procedures on the same date.
Some payers require it; others (including many Medicare Administrative Contractors) have specific multiple-procedure reduction policies that apply automatically. Verify payer-specific rules before applying Modifier -51, as incorrect use can trigger a payment reduction that wasn’t warranted.
Check NCCI (National Correct Coding Initiative) edits before billing CPT code 12001 with any foreign body removal code. The Medicaid NCCI edits bundle wound repair codes 12001-13153 with removal of foreign body services, meaning they should not be reported together. Verify against the current CMS NCCI Policy Manual for the applicable version.
CPT code 12001 carries a global period of “000” per the Medicare Physician Fee Schedule. Zero post-operative days means the global package includes only the day of the procedure itself. No follow-up wound checks, suture removals, or dressing changes are bundled into the payment beyond the date of service.
The practical implication: a return visit the following day for suture removal or wound inspection can be billed separately using an E/M code. This is a significant difference from procedures with 10-day or 90-day global periods, where post-op visits are included in the original payment and cannot be separately billed.
Confirming the global period through the CMS Physician Fee Schedule lookup is good practice before advising patients or scheduling follow-up appointments.
Medicare reimbursement for CPT code 12001 is calculated using the Resource-Based Relative Value Scale (RBRVS). Payment varies by geographic location based on the Geographic Practice Cost Index (GPCI).
National average reimbursement figures change each year with the Medicare Physician Fee Schedule update; always verify current amounts using the CMS Physician Fee Schedule lookup (linked above) to get location-adjusted figures before quoting patients or running financial projections.
As a reference point, CPT code 12001 is a relatively low-RVU procedure. Practices billing it as a standalone code should ensure documentation supports the full procedure, including wound preparation (cleansing, irrigation), since these are included in the work RVU and should not be separately billed.
Providers managing critical-care patients with wound injuries may also reference the CPT code 99291 critical care services billing guide. Pabau’s claims management software integration automatically checks fee schedule alignment and flags claims where submitted charges fall outside expected MPFS ranges.
Medicaid reimbursement for 12001 varies by state and managed care organization. Some state Medicaid programs reimburse at a percentage of the Medicare fee schedule; others use independently negotiated rates. Practices billing Medicaid should verify rates through their state’s Medicaid fee schedule rather than relying on the MPFS as a proxy.
Commercial payers typically negotiate rates above Medicare; confirm contracted rates in payer agreements before submitting claims.
Pabau's built-in claims management tools help practices track modifier requirements, document wound measurements at the point of care, and submit cleaner CPT code 12001 claims from day one.

When a patient presents with more than one wound requiring repair, the additive length rule applies for wounds in the same anatomical grouping. Wounds of the same complexity type (simple, intermediate, or complex) repaired on the same anatomical site grouping have their lengths added together and reported under a single code representing the combined total length. Practices that also handle deeper wounds requiring debridement before closure should review the CCSD code S4213 debridement and primary suture billing guide for the coding distinction.
CPT code 12001 covers wounds up to 2.5 cm. If two simple wounds on the trunk measure 1.5 cm and 1.5 cm, the combined length is 3.0 cm, which moves into the 12002 range (2.6-7.5 cm). Reporting both separately as 12001 would be incorrect and could trigger an NCCI edit or payer audit.
The additive rule applies per anatomical grouping, so a simple scalp wound and a simple trunk wound repaired the same day are reported separately, each under its own code, because they occupy different site groupings.
When repairs of different complexity types are performed on the same date, each complexity level is coded separately, and Modifier -59 identifies the distinct services. Reviewing current HIPAA compliance standards for medical offices also matters here, as billing two codes for what is effectively one service can constitute an improper claim if not documented correctly.
Understanding where 12001 sits within the broader repair series helps coders select the correct code when wound characteristics fall outside the 12001 criteria. The AAPC Codify CPT lookup provides the full descriptor and instructional notes for each code in the series.
Intermediate repair (12031-12037) applies when one or more of the following are present: layered closure of one or more deeper layers, wound contamination requiring significant cleansing, or infected wounds. Complex repair (13100-13160) covers wounds requiring more than layered closure, such as scar revision, debridement, or extensive undermining.
For further reference on CPT billing across procedure categories, see new patient office visit and other CPT code billing guides in the Pabau procedure codes library.
The single most common coding error in simple wound repair is billing 12001 for a wound that measures between 2.6 cm and 7.5 cm, which belongs to 12002. Both codes cover the same anatomical sites and the same simple repair criteria; the only difference is wound length.
Measuring before closure (not after, when wound edges may approximate differently) gives the most defensible measurement for the claim.
Every 12001 claim requires at least one ICD-10-CM diagnosis code that supports medical necessity for the wound repair. The correct ICD-10 code depends on the wound type, body site, and clinical circumstances. Payers use ICD-10 pairing to validate that the procedure matches the diagnosis.
Maintaining accurate HIPAA-compliant documentation for injury-related claims is particularly important when billing under S-code categories, as these often require laterality and encounter type (initial, subsequent, or sequela). Hand injuries involving a retained foreign body, such as those described in the ICD-10 code S61.122D thumb laceration with foreign body guide, need additional specificity beyond the codes listed here.
Always use the most specific ICD-10 code available. Unspecified codes (those ending in 9 or containing “unspecified”) are acceptable only when the clinical record genuinely does not support greater specificity. Payers increasingly apply LCD and NCD policies that restrict payment for unspecified codes when more specific options exist.
Good patient compliance documentation during wound assessment, including clear notes on laterality and wound etiology, supports accurate ICD-10 code selection and reduces payer requests for additional information. For partial traumatic injuries that may accompany lacerations, see also the ICD-10 code S88.929D partial traumatic amputation billing guide.
When billing CPT code 12001 for a wound with a retained foreign body removed during repair, do not also bill a foreign body removal code on the same claim. The CMS NCCI edits bundle wound repair codes 12001–13160 with foreign body removal. Document the foreign body removal in the procedure note, but do not attempt to separately bill it alongside the repair code.
Claims examiners and coding auditors see the same errors on 12001 claims repeatedly. Knowing the denial patterns helps billing staff prevent them before submission rather than chasing appeals. Using automated billing workflows with pre-submission claim scrubbing catches most of these systematically.
Practices that review denial patterns monthly and route those insights back into documentation templates significantly reduce denial rates over time. Pabau’s practice management software features include claim status tracking and denial categorization to make that feedback loop practical for small and mid-sized practices. The same discipline applies across other high-volume codes, as outlined in the CPT code 97014 denial prevention guide.
Practices performing cardiovascular procedures alongside wound repair may also find the CPT code 93015 cardiovascular stress test billing guide useful for multi-specialty billing workflows, and teams that also handle anesthesia claims can compare how the anesthesia base-unit approach works in the CPT Code 00950 (Vaginal Endoscopy Anesthesia) billing guide.
CPT code 12001 is a straightforward code on paper. In practice, the wound measurement, anatomical site classification, closure documentation, and modifier logic generate more billing friction than the procedure’s simplicity would suggest.
Pabau’s claims management software brings measurement fields, modifier prompts, and NCCI edit flags directly into the documentation and billing workflow, so 12001 claims go out complete and come back paid.
For vaccine billing workflows that often accompany urgent-care wound visits, the CPT code 90715 Tdap vaccine billing guide is a helpful companion reference. To see how Pabau supports integumentary billing in your practice, book a demo with the team.
Need a structured workflow for wound documentation? Pabau’s digital forms let practices build procedure-specific note templates that capture wound measurements, site, depth, and closure method at the point of care.
Billing across multiple CPT specialties? Pabau’s CPT code billing guides cover procedure billing across specialties, from integumentary to reproductive medicine.
Want to streamline your claims submission process? Simplifying practice management explains how integrated EHR and billing workflows reduce rework and denial rates for procedure-heavy practices.
CPT code 12001 covers simple repair of superficial wounds measuring 2.5 cm or less on the scalp, neck, axillae, external genitalia, trunk, and extremities including hands and feet. The repair must involve only the epidermis, dermis, or subcutaneous tissue and require no more than one-layer closure using sutures, staples, tissue adhesive, adhesive strips, or a combination of these methods. Wounds on the face, ears, eyelids, nose, lips, and mucous membranes fall under a separate code series (12011-12018) even when the repair is clinically simple.
The global period for CPT code 12001 is “000,” meaning zero post-operative days. Only the day of the procedure itself is included in the global package. Follow-up visits for suture removal, wound checks, or dressing changes on any subsequent date can be billed separately using an appropriate E/M code.
Three modifiers apply most commonly. Modifier -25 is appended to a same-date E/M code to identify it as a significant, separately identifiable service. Modifier -59 is appended to 12001 when it is the secondary repair code billed alongside a higher-complexity repair on the same date, indicating the procedures are distinct. Modifier -51 may apply when 12001 is billed alongside non-repair procedures in the same session, though Medicare applies multiple-procedure reductions automatically.
Both 12001 and 12002 cover simple repair of superficial wounds on the same anatomical sites (scalp, neck, axillae, external genitalia, trunk, and extremities). The only difference is wound length: 12001 applies to wounds 2.5 cm or less, while 12002 applies to wounds from 2.6 cm to 7.5 cm. When multiple wounds in the same anatomical grouping are repaired on the same date, their lengths are added together before selecting the correct code, which can shift a claim from 12001 to 12002.
Yes, but only when the E/M service is a significant, separately identifiable service beyond the decision to perform and perform the wound repair. Modifier -25 must be appended to the E/M code, and the clinical documentation must support that the visit addressed a distinct problem or condition. Without Modifier -25 and adequate supporting documentation, payers will bundle the E/M into the repair and deny it.
The appropriate ICD-10-CM code depends on the wound type, anatomical site, and etiology. S-category injury codes are most common, such as S01.01XA (unspecified open wound of scalp, initial encounter) or S71.011A (laceration without foreign body of right thigh, initial encounter). Always use the most specific code available, including laterality and encounter type (initial “A,” subsequent “D,” or sequela “S”) to reduce payer requests for additional documentation.



