ICD-10 code S53.442D: UCL sprain of left elbow, subsequent encounter
ICD-10 code S53.442D is a valid, billable ICD-10-CM diagnosis code effective Oct...
Last Updated: August 10, 2026
CPT code 01464 describes anesthesia for arthroscopic procedures of the ankle and/or foot — distinct from CPT 01400, the separate knee-joint arthroscopy code it is sometimes confused with
The code carries 3 base units. Reimbursement is calculated as (Base Units + Time Units + Modifying Units) x Conversion Factor
Modifier selection (AA, QK, QX, QZ) depends on whether an anesthesiologist performs or medically directs the case, and whether a CRNA is involved
Practice management software like Pabau streamlines CPT 01464 billing by combining code entry, modifier selection, and claim submission in one workflow
CPT code 01464 is the anesthesia code for arthroscopic procedures of the ankle and/or foot. It carries 3 base units and sits in the lower leg, ankle, and foot anesthesia section — distinct from CPT 01400, which covers knee-joint arthroscopy, and from neighboring lower-leg codes like 01462 and 01470.
Getting this code wrong triggers claim rejections, delayed reimbursement, and audit flags. This reference covers the official description, base unit value, applicable modifiers, 2025/2026 Medicare reimbursement rates, common ICD-10 pairings, and billing guidelines for CPT code 01464 so anesthesia billers and coders can submit clean claims the first time.
CPT code 01464 covers anesthesia for arthroscopic procedures performed on the ankle joint and/or the foot, including diagnosis and treatment of osteochondral lesions, anterior ankle impingement, loose bodies, synovitis, and chronic ankle instability.
It sits in the “Anesthesia for Procedures on the Lower Leg (Below Knee)” section of the CPT anesthesia code set, alongside 01462, 01470, and 01480, which also cover the lower leg, ankle, and foot region. It does not cover knee-joint arthroscopy, which is billed under CPT 01400 in the separate “Knee and Popliteal Area” section.
Ankle and foot arthroscopy under this code is common among sports medicine practices treating ligament and cartilage injuries, with post-operative rehabilitation often coordinated through physical therapy providers billing separately for the recovery phase.
CPT code 01464 carries 3 base units, set by the American Medical Association and confirmed on CMS and VA nationwide anesthesia base-unit tables. Base units represent the inherent complexity of administering anesthesia for a given procedure type. Every anesthesia reimbursement calculation for this code starts here.
The same CMS and AMA base-unit table also covers other recently published anesthesia procedure codes, including CPT 01272 and CPT 01444.
The standard Medicare anesthesia reimbursement formula is:
Time units are calculated by dividing total anesthesia time (start of induction to patient transfer out of anesthesia care) by 15 minutes, rounding to the nearest unit per payer policy.
Accurate time documentation is therefore critical: A 60-minute case generates 4 time units, giving a total of 7 units before modifying units. You can verify current conversion factor values using the CMS Physician Fee Schedule lookup tool.
Modifier selection for CPT code 01464 determines how much Medicare reimburses and who is authorized to bill. The wrong modifier on an anesthesia claim is one of the fastest routes to a denial or a post-payment audit.
For medical direction (QK/QX) to be valid under CMS rules, the anesthesiologist must satisfy all seven conditions:
Missing a single condition voids the medical direction claim and exposes the practice to repayment liability.
CRNA eligibility for QZ billing varies by state. As of mid-2026, 26 states have opted out of the federal physician supervision requirement, allowing CRNAs to bill at the full rate independently.
Confirm your state’s current opt-out status using the ASA opt-out tracker before applying QZ to any CPT code 01464 claim. More on billing compliance protocols is available for practices building internal review processes.
Document which modifier applies before the case starts, not after. When an anesthesiologist begins a case intending to personally perform it (AA) but is pulled to direct another case mid-procedure, the modifier must be updated and the record must reflect the handoff time. Retroactive modifier changes without contemporaneous documentation are a common audit trigger.
Medicare calculates anesthesia reimbursement using the formula described above, applying a locality-specific conversion factor. The Centers for Medicare and Medicaid Services (CMS) publishes an annual anesthesia conversion factor. The rate varies by geographic practice cost index (GPCI) locality, meaning a practice in San Francisco reimburses differently from one in rural Mississippi for the identical CPT code 01464 claim.
A 45-minute ankle arthroscopy under general anesthesia billed with CPT code 01464 generates 3 time units (45 minutes divided by 15). With 3 base units, a P1 patient (0 modifying units), and an illustrative conversion factor of $21.00, the calculation is: (3 + 3 + 0) x $21.00 = $126.00 for an AA modifier claim.
QK and QX claims at 50% would each receive $63.00. Verify current conversion factor values directly via the FastRVU 2026 RVU lookup tool or on the CMS fee schedule for the applicable payment year.
Private payer rates are negotiated separately and often exceed Medicare rates. Medicaid rates vary by state and typically fall below Medicare. When billing CPT code 01464 to commercial insurers, confirm the payer’s specific conversion factor and any policy-level modifiers in the provider contract before submitting.
Every CPT code 01464 claim must carry at least one ICD-10-CM diagnosis code establishing medical necessity. The diagnosis must support the arthroscopic procedure being performed on the ankle or foot. Mismatched or overly vague diagnosis codes are a top reason for claim rejections on anesthesia services.
Always verify ICD-10-CM codes against the current tabular list before submission. Using the AAPC Codify CPT lookup alongside the ICD-10 crosswalk can confirm medical necessity linkage. Laterality matters: codes for left-side and right-side ankle and foot procedures are distinct, and submitting without the correct laterality qualifier commonly triggers edits.
Clean CPT code 01464 claims require meeting several pre-submission checkpoints. Skipping any one of them increases the likelihood of a rejection or a post-payment audit. Review these medical office compliance requirements alongside the code-specific rules below.
Anesthesia records for CPT code 01464 must contain all of the following to support audit-proof billing. Using standardized clinical documentation forms reduces the risk of missing a required element.
Maintaining HIPAA-compliant documentation practices across all anesthesia records protects the practice both during payer audits and in the event of a patient complaint. Digital anesthesia records also support faster retrieval during post-payment review windows. Consider moving to paperless anesthesia record workflows to streamline this process.
Pabau brings CPT code entry, modifier selection, and claim submission into one platform so your billing team spends less time on manual steps and more time ensuring clean claims.

Coders frequently look up CPT code 01464 alongside adjacent lower-leg anesthesia codes — and alongside CPT 01400, the separate knee-joint arthroscopy code it’s sometimes confused with. The distinctions are specific: Wrong code selection between 01462, 01464, and 01400 is a common billing error because all three involve arthroscopic or lower-limb anesthesia.
The critical distinction for CPT code 01464 is twofold. First, versus 01400: 01464 applies to the ankle and/or foot, while 01400 applies to the knee joint — different anatomical sites, different CPT sections, and different base unit values (3 versus 4), so the two are never interchangeable.
Second, versus 01462, 01470, and 01480: All four ankle/foot-region codes share the same 3 base units, so payers rely entirely on procedure type (arthroscopic, closed, soft tissue, or open bone) to differentiate the claim.
Billing an ankle arthroscopy under 01462, or a knee arthroscopy under 01464, will likely trigger a denial for a procedure-code mismatch. The identical base-unit-plus-modifier formula also applies to CPT 01830.
Reference tools and fee schedule lookups tell you what CPT code 01464 pays. Getting it paid accurately requires clean execution across every step of the claim lifecycle: code selection, modifier assignment, documentation capture, and submission.
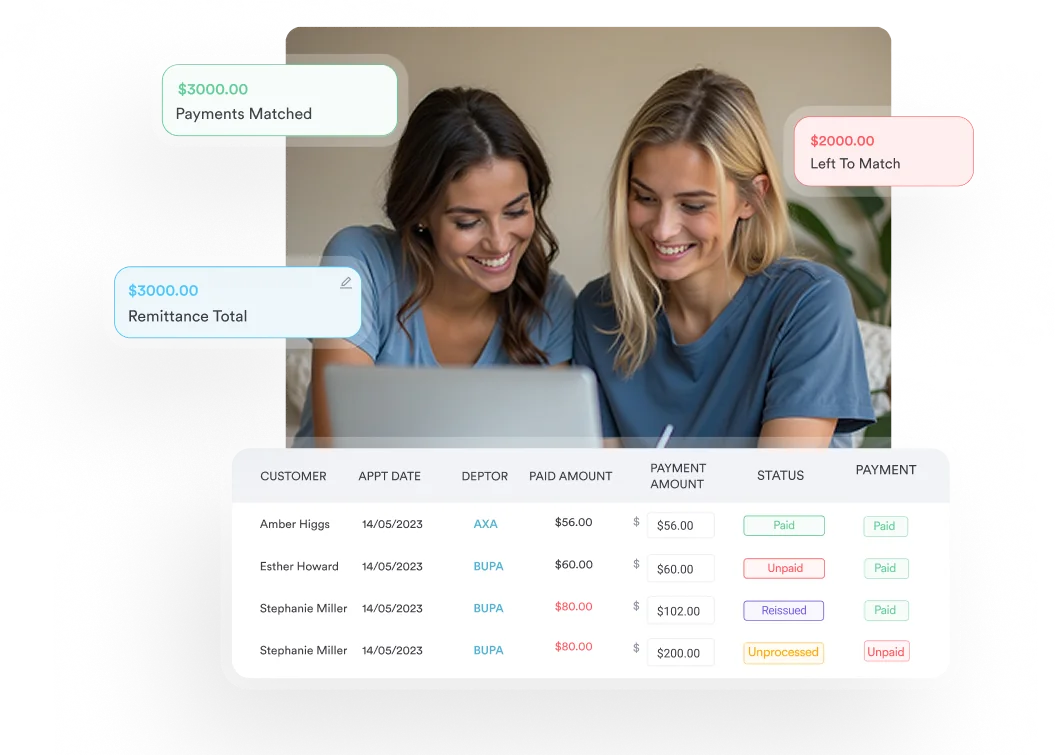
Most anesthesia billing errors come from workflow breakdowns between the anesthesia record, the billing team, and the clearinghouse. Practice management software like Pabau that integrates clinical documentation with billing workflows closes that disconnect.
Its claims management workflows allow billing teams to enter CPT codes, apply modifiers, attach supporting diagnosis codes, and submit claims within a single platform rather than switching between a coding reference tool, an EHR, and a separate billing system.
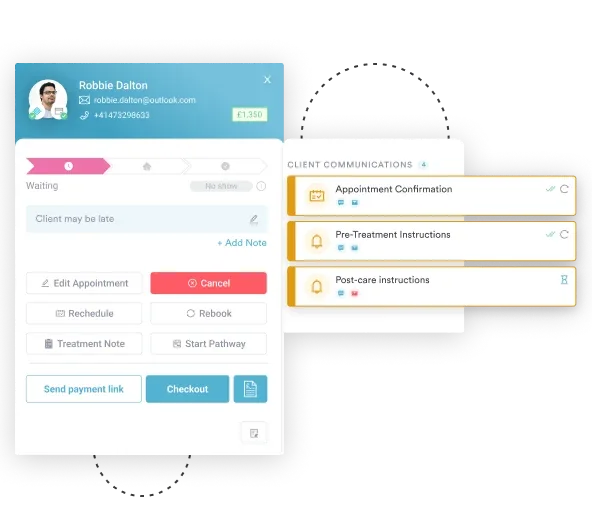
The digital intake and documentation forms feature supports structured pre-anesthesia evaluations and intraoperative records that can be retrieved quickly during payer audit requests.
For practices running multiple anesthesia providers across different case types, automated billing workflows can trigger documentation reminders at case completion, flag missing time entries before claims are batched, and route claims by modifier type for team review. Practice management software that connects the clinical record to the billing cycle is where most anesthesia practices find meaningful reductions in denial rates.
Run a monthly denial audit filtered to anesthesia codes 01462-01480, and check separately for any claims that mistakenly used the knee-joint code 01400 for an ankle or foot procedure (or vice versa). If CPT 01464 denials cluster around modifier type (AA vs QK/QX), that signals inconsistent documentation of how providers record their role at case end. If denials cluster around diagnosis codes, review ICD-10 pairing for the most common surgical procedures your anesthesia team covers.
CPT code 01464 is a precise code: It applies specifically to arthroscopic procedures of the ankle and/or foot, carries 3 base units, and reimburses differently depending on which modifier reflects the documented provider role.
It is a distinct code from CPT 01400 (knee joint arthroscopy, 4 base units) and from its lower-leg neighbors 01462, 01470, and 01480 (each also 3 base units, but for different procedure types).
The most common billing failures on this code come from three sources:
Pabau’s claims management software helps anesthesia and surgical practices fix those breakdowns by connecting clinical documentation to claim submission in one workflow. To see how it handles anesthesia code billing in practice, book a demo with the team.
List Item #1
List Item #2
CPT code 01464 is the anesthesia code for arthroscopic procedures of the ankle and/or foot. It covers anesthesia services for ankle and foot arthroscopies, including treatment of osteochondral lesions, anterior ankle impingement, loose body removal, and chronic ankle instability repair. It does not apply to knee-joint arthroscopy, which uses CPT 01400, or to closed lower-leg procedures or open bone procedures, which use different codes.
CPT code 01464 carries 3 base units as set by the American Medical Association and confirmed on CMS and VA nationwide anesthesia base-unit tables. These base units are added to time units (1 per 15 minutes of anesthesia time) and modifying units (based on physical status), then multiplied by the applicable CMS conversion factor to calculate the total reimbursement amount for the claim.
The primary modifiers for CPT code 01464 are AA (anesthesiologist personally performs), QK (anesthesiologist medically directs 2-4 CRNA cases), QX (CRNA under medical direction), QZ (CRNA without physician supervision in opt-out states), QY (medical direction of one CRNA), and AD (supervision of more than 4 concurrent cases). Physical status modifiers P1 through P6 are also appended to reflect patient complexity.
Medicare reimbursement for CPT code 01464 is not a fixed dollar amount. It is calculated using the formula (Base Units + Time Units + Modifying Units) x Conversion Factor, where the conversion factor is locality-specific and updated annually by CMS. Check the current conversion factor for your locality using the CMS Physician Fee Schedule lookup before estimating payment for any specific claim.
Both CPT 01462 and CPT 01464 carry 3 base units, so the difference is procedure type, not payment value. CPT 01462 covers closed (non-arthroscopic) procedures on the lower leg, ankle, and foot, while CPT code 01464 covers arthroscopic procedures of the ankle and/or foot specifically. Billing an arthroscopic ankle procedure under 01462 is incorrect and will likely trigger a denial.
No. CPT 01400 covers anesthesia for open or surgical arthroscopic procedures on the knee joint and carries 4 base units. CPT code 01464 covers arthroscopic procedures of the ankle and/or foot and carries 3 base units. The two codes cover different anatomical sites and CPT sections and are not interchangeable — using 01464 for a knee arthroscopy, or 01400 for an ankle or foot arthroscopy, will result in a claim denial.
Yes, a CRNA can bill CPT code 01464. When working under anesthesiologist medical direction, the CRNA uses modifier QX (reimbursed at 50% of the allowed amount). When working without physician supervision in a state that has opted out of the federal supervision requirement, the CRNA uses modifier QZ and bills at 100% of the allowed amount. As of mid-2026, 26 states have opted out of the federal requirement. Confirm current state law via the ASA opt-out tracker before applying QZ.
Anesthesia reimbursement for CPT code 01464 follows the formula: (Base Units + Time Units + Modifying Units) x Conversion Factor. With 3 base units, a 45-minute case generates 3 time units. Adding 0 modifying units for a P1 patient gives 6 total units. Multiplied by the applicable locality conversion factor (published annually by CMS), that produces the gross allowed amount before any modifier-based reduction (such as the 50% reduction for QK/QX).