HCPCS Code A7033: Nasal pillow replacement billing guide 2026
A7033 bills replacement nasal pillows per pair, not per pillow. Medicare allows ...
Last Updated: August 6, 2026
CPT Code 00632 describes anesthesia for procedures in the lumbar region, specifically lumbar sympathectomy
The ASA assigns 7 base units to this code; total payment uses the formula (base units + time units) x conversion factor x GPCI
Modifier AA is required when an anesthesiologist personally performs the service; omitting it is one of the most common denial triggers
Pabau’s claims management software automates base and time unit calculations, modifier prompts, and claim scrubbing for anesthesia billing teams
CPT Code 00632 is the anesthesia code for procedures in the lumbar region, specifically lumbar sympathectomy. The anesthesiologist or CRNA providing anesthesia care reports it, not the surgeon performing the procedure. This reference covers the code definition, base units, modifiers, 2026 fee schedule data, the ICD-10 crosswalk, documentation requirements, and the billing errors most likely to trigger a denial.
This guide is written for anesthesia billers, coders, and practice managers who need a current, reliable reference for CPT Code 00632 alongside the broader lumbar anesthesia code family.
CPT Code 00632 is the procedure code used to report anesthesia services provided during surgical procedures in the lumbar region, with the specific descriptor covering lumbar sympathectomy. The American Medical Association (AMA), which owns and maintains the CPT code set, places 00632 within the Anesthesia section under codes for procedures on the lower back and lumbar region (the 00600-00640 range).
The full official descriptor reads: Anesthesia for procedures in lumbar region; lumbar sympathectomy.
For coders looking to cross-reference related lumbar anesthesia codes, the AAPC Codify CPT lookup tool provides full descriptor text and crosswalk data for the entire 006xx anesthesia range. Pabau’s coaching CPT codes reference also demonstrates how anesthesia billing logic applies across specialty-specific code families.
Lumbar sympathectomy is a surgical procedure that interrupts sympathetic nerve fibers in the lumbar region of the sympathetic chain. It is used to treat conditions where excessive sympathetic nerve activity causes vascular insufficiency, chronic pain, or hyperhidrosis in the lower extremities.
The procedure can be performed open (via retroperitoneal or transperitoneal approach) or laparoscopically. The anesthesiologist reports CPT Code 00632 regardless of surgical approach, as long as the procedure is a lumbar sympathectomy.
If the anesthesia is provided for a different lumbar procedure, such as diskectomy, laminectomy, or fusion, it is reported under 00630 as anesthesia for lumbar procedures not otherwise specified, since none of those procedures has its own dedicated code.
The distinction between 00632 and adjacent lumbar codes is clinically driven. If the operative report describes sympathetic chain interruption in the lumbar region, 00632 is correct.
For lumbar procedures not separately coded, or for diagnostic or therapeutic lumbar puncture, see the 00630 or 00635 range. Practices billing anesthesia for spine surgery across multiple procedure types will find Pabau’s CPT code reference library a useful companion for understanding how code selection logic differs by clinical context.
Anesthesia reimbursement does not work like standard procedure codes. Payment is calculated using base units assigned by the Centers for Medicare and Medicaid Services (CMS) and the American Society of Anesthesiologists (ASA) Relative Value Guide (RVG), combined with time units accrued during the procedure.
CPT Code 00632 carries 7 base units according to the ASA Relative Value Guide. Base unit values reflect the relative complexity and risk associated with the procedure for which anesthesia is administered. Lumbar sympathectomy sits at a mid-level complexity within the lumbar anesthesia code family.
The FastRVU 2026 RVU lookup tool applies the finalized CY2026 conversion factor with locality-specific geographic adjustment, useful for calculating exact payment in a specific GPCI region.
The standard CMS anesthesia payment formula applies to CPT Code 00632 as it does to all anesthesia procedure codes. Reimbursement is not a flat fee: It scales with procedure complexity (base units) and the actual duration of anesthesia services (time units).
Payment formula: (Base Units + Time Units) x Anesthesia Conversion Factor x GPCI
A 90-minute lumbar sympathectomy would generate 6 time units (90 min / 15 min per unit). Adding 7 base units gives 13 total units. At the finalized CY2026 Medicare conversion factor of $20.4976 per unit (before GPCI adjustment), the raw Medicare payment before geographic adjustment is approximately $266. Payment varies by locality, payer, and whether qualifying circumstances apply.
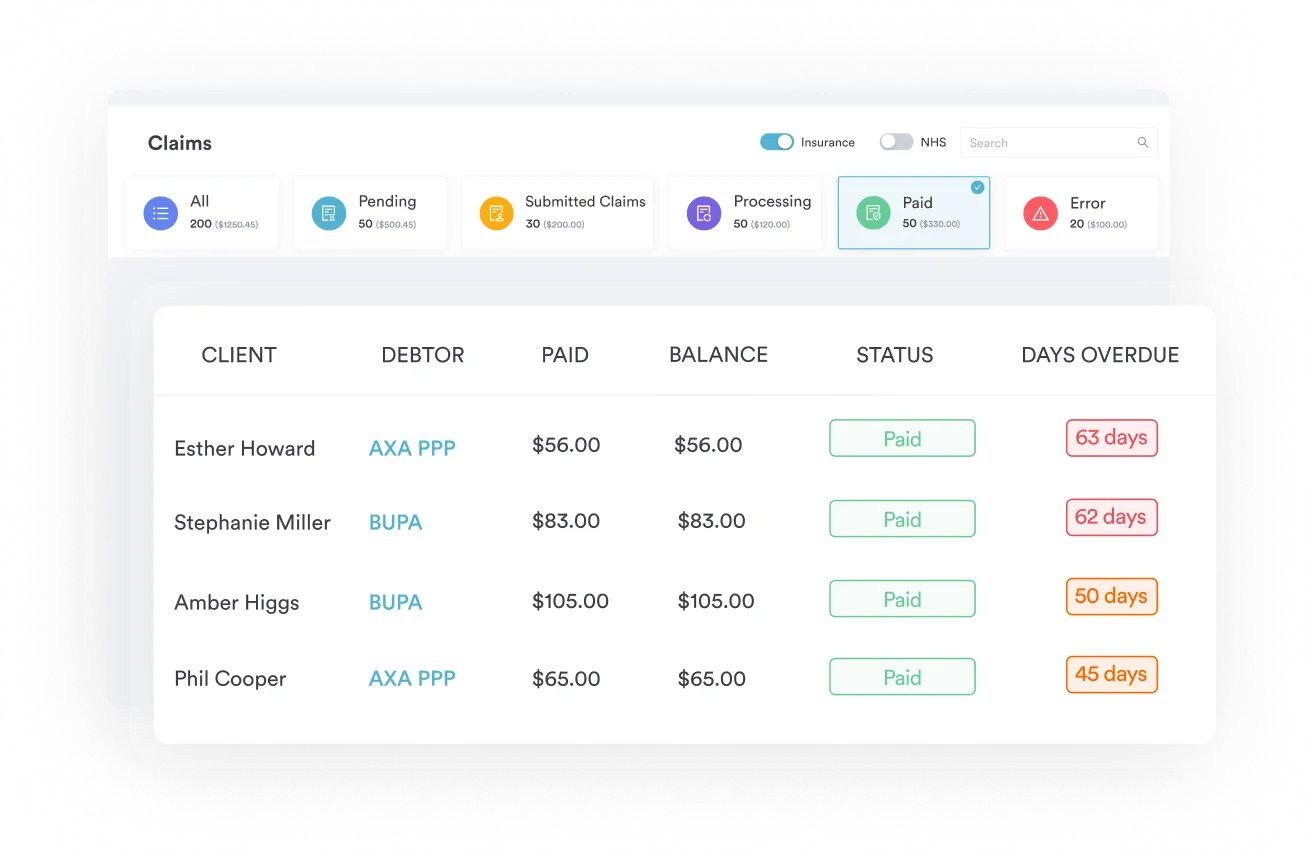
Commercial payers typically negotiate rates above Medicare. The difference between Medicare and commercial rates for anesthesia services varies significantly by region and payer contract. Practices using Pabau’s claims management software can track payer-specific payment patterns against expected rates to catch underpayment systematically rather than case by case.
Medicare payment for anesthesia services is governed by the CMS Physician Fee Schedule and the anesthesia-specific conversion factor published in the annual PFS Final Rule. Geographic Payment Cost Indices (GPCI) adjust payment up or down based on locality.
These figures use the finalized CY2026 conversion factor and do not include GPCI adjustment. High-cost localities (Manhattan, San Francisco) typically yield higher payments; rural or low-cost localities yield less. Apply the locality-specific GPCI from the CMS Physician Fee Schedule lookup before using these figures for contract negotiation or revenue projections.
Track anesthesia time documentation against billed time units at claim submission. Discrepancies between the anesthesia start/stop times in the record and the time units billed are one of the most audited items in anesthesia claims. Build a workflow that calculates units directly from the timed record, not from memory or manual entry.
Anesthesia modifiers are required on every anesthesia claim. Unlike surgical codes, anesthesia codes do not stand alone: The modifier communicates the care delivery model (who provided the anesthesia and under what supervision structure), and CMS and commercial payers use it to determine the applicable payment percentage.
Modifier selection is not optional. CMS will deny or reduce payment when the modifier is missing, incorrect, or inconsistent with the supervision documentation in the record.
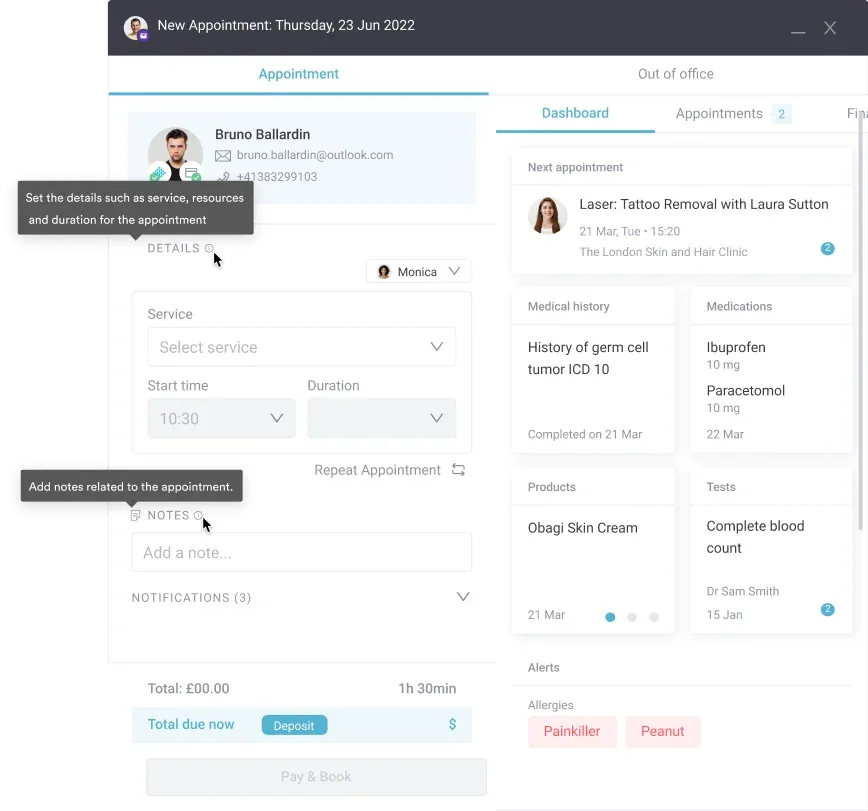
Practices billing CPT Code 00632 should verify that the modifier on the claim matches the care delivery model documented in the anesthesia record. Pabau’s automated workflows can prompt for modifier selection at the point of claim creation, reducing the risk of a missing or misapplied modifier.
Qualifying circumstances are add-on codes that may be reported alongside CPT Code 00632 when specific clinical conditions increase the complexity of anesthesia services. They are not routinely reported: Clinical documentation must support their use, and applicability depends on the patient’s condition and the clinical judgment of the anesthesiologist.
Verify current NCCI edits and any applicable MAC local coverage determinations (LCDs) before reporting these add-on codes. Payer policies on qualifying circumstances vary, and some commercial payers require prior authorization or additional documentation.
Practices handling high-complexity surgical anesthesia cases will benefit from having a structured digital documentation workflow that captures qualifying circumstance criteria in the anesthesia record before the claim is created.
Pabau's claims management and workflow automation tools help anesthesia billing teams apply the right modifiers, calculate time units accurately, and catch documentation issues before claims go out the door.

Medical necessity for lumbar sympathectomy anesthesia must be supported by an appropriate ICD-10-CM diagnosis code. The diagnosis code communicates why the procedure was performed. Payers may deny CPT Code 00632 if the submitted diagnosis does not align with recognized clinical indications for lumbar sympathectomy.
This crosswalk is for reference only. Coverage is payer-specific and LCD-dependent. Confirm diagnosis code validity against the current FY ICD-10-CM tabular list and your MAC’s applicable LCD before submitting claims.
G90.521 is the specific code for complex regional pain syndrome I of the right lower limb, with laterality carried in the final digit: .521 for the right limb, .522 for the left, and .523 for bilateral involvement. Vascular indications for this procedure also sit within the same circulatory-system block as I76.
Practices managing complex pain and vascular cases can use Pabau’s structured client records to capture and carry diagnosis codes consistently from the clinical note through to the billing claim.
Anesthesia claims for CPT Code 00632 require documentation that demonstrates the service was personally performed or appropriately supervised, that time was accurately recorded, and that medical necessity is supported. Missing or inconsistent documentation is the most common reason for post-payment audit recovery demands in anesthesia billing.
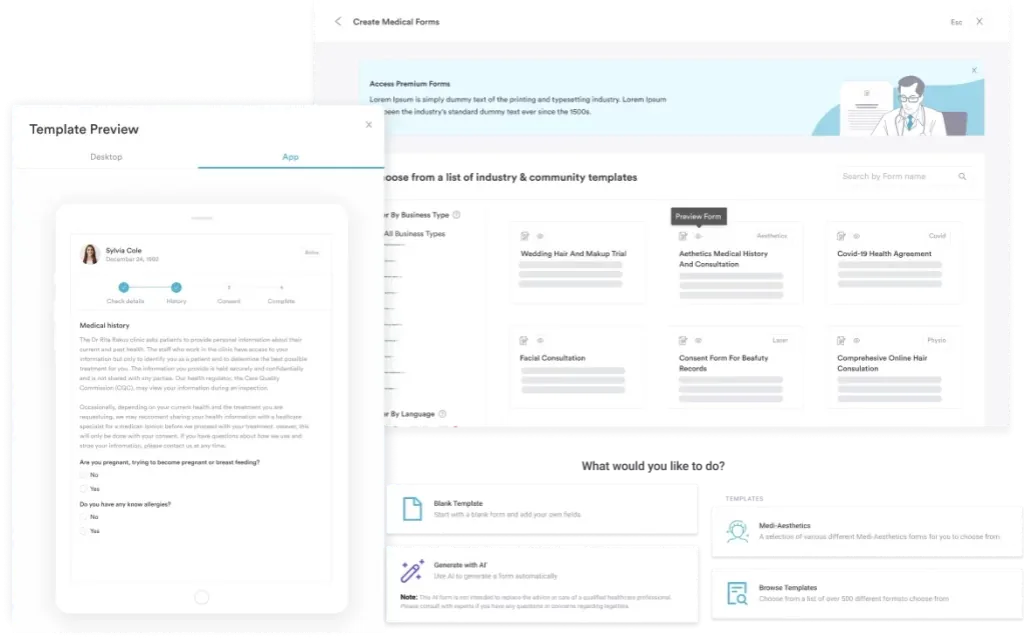
Practices with structured clinical documentation templates for anesthesia services can reduce documentation issues before they become audit findings. The ADHD screening CPT code reference on Pabau’s procedure code library illustrates how structured pre-visit documentation workflows translate into cleaner billing across specialty code families.
Anesthesia billing for lumbar procedures has a consistent set of denial patterns. Most are preventable with a structured pre-submission review process.
Practices can review fee schedule data by payer for CPT Code 00632 via the Pabau fee schedule reference, which covers multi-payer billing context. Denial pattern tracking across a claim volume gives billing teams the data to identify which of these errors is most prevalent in their specific payer mix.
For broader practice billing management context, Pabau’s practice management software guide covers how integrated billing and documentation workflows reduce denial rates across specialties.
Choosing the correct code within the lumbar anesthesia range requires reading the operative report carefully. The procedures below are frequently performed in the same surgical setting, and incorrect code selection is an audit risk. The same base-plus-time-unit formula governs anesthesia codes throughout the CPT set, including 01500 and 01991.
There is no dedicated CPT code for anesthesia during lumbar diskectomy, laminectomy, or spinal fusion. Those procedures are reported under 00630, the not-otherwise-specified code for the lumbar region. Misassigning between 00630 and 00632 is a documented audit pattern: Reporting 00630 for a case that was actually a lumbar sympathectomy, or the reverse, is a compliance risk.
Always base code selection on the operative report, not the anticipated complexity. Anesthesia practices managing spine surgery volume will find the Pabau surgical EMR feature set relevant for maintaining procedure-level documentation integrity across complex cases, and practices whose referral network extends into spinal manipulation can apply the same documentation discipline with Pabau’s chiropractic practice tools.
A static code lookup tells you what CPT Code 00632 is. It doesn’t help you bill it accurately. Anesthesia billing involves three error-prone calculations on every claim: Base unit assignment, time unit calculation, and modifier selection. Each one is manual without dedicated billing software, and each one is auditable.
Pabau’s claims management software automates the anesthesia billing workflow at each of these points. Base units are assigned to the procedure code at the point of claim creation.
Time units calculate automatically from the documented start and stop times in the anesthesia record. Modifier prompts appear based on the recorded provider role, reducing the risk of a missing or misapplied modifier on CPT Code 00632 claims.
For anesthesia practices and surgical facilities managing lumbar procedure volume, the combination of structured documentation and integrated claim creation keeps what was documented and what was billed aligned. Practices interested in how integrated automated billing workflows reduce denial rates can explore Pabau’s documentation and claims workflow in a live demo.
Run a quarterly audit of CPT Code 00632 claims against anesthesia records. Compare billed time units to documented start and stop times, verify modifier selection matches the supervision model in the record, and flag any qualifying circumstance add-on codes where the clinical basis is unclear. A 30-minute quarterly review prevents the kind of billing pattern that triggers a payer audit.
Lumbar sympathectomy anesthesia billing is low-volume for most practices, which is exactly why errors accumulate. When a code isn’t billed frequently, modifiers get missed, time units get estimated rather than calculated, and qualifying circumstance documentation gets skipped. Those issues translate directly into denials and audit exposure.
Pabau’s claims management software addresses the three core failure points in anesthesia billing: Base and time unit calculation, modifier selection, and pre-submission claim scrubbing.
For practices managing lumbar anesthesia cases alongside a broader surgical mix, integrated documentation and billing workflows reduce the manual steps that cause CPT Code 00632 claims to fail. To see how Pabau handles anesthesia billing end to end, book a demo with the team.
Need to see anesthesia coding logic applied to a different region? 00164 walks through the same base-and-time-unit structure for anesthesia during nasal and sinus procedures.
Billing a drug administered alongside anesthesia care? J0640 covers the HCPCS side of drug billing that often accompanies a surgical anesthesia claim.
Coding a musculoskeletal diagnosis instead? M60.9 shows how the same diagnosis-to-claim documentation trail applies outside the lumbar anesthesia family.
CPT Code 00632 is anesthesia for procedures in the lumbar region specifically lumbar sympathectomy. It covers the full scope of anesthesia services including pre-anesthetic evaluation, intraoperative monitoring, and post-anesthetic care, reported by the anesthesiologist or supervising provider, not the operating surgeon.
CPT 00632 carries 7 base units per the ASA Relative Value Guide. Total anesthesia payment adds time units (1 per 15 minutes of anesthesia) to the base units, then multiplies by the anesthesia conversion factor and geographic price cost index (GPCI).
The anesthesia modifier depends on the care delivery model: AA for personal performance by an anesthesiologist (100% payment), QK for medical direction of 2-4 concurrent procedures (50%), QZ for an independent CRNA (100%), QX for a medically directed CRNA (50%), and AD for supervision of more than 4 concurrent procedures (3 base units only). The modifier must match the documented supervision structure.
Yes, Medicare covers CPT Code 00632 when medical necessity is documented and the claim is submitted with a valid anesthesia modifier and a supporting ICD-10-CM diagnosis code. Payment uses the Medicare anesthesia conversion factor and GPCI for the locality. Coverage depends on the applicable MAC LCD and diagnosis code alignment.
Standard CPT codes pay a flat RVU-based fee regardless of procedure duration. Anesthesia base unit calculation adds time units to the base units: Every 15 minutes of anesthesia time generates one additional unit. The total (base plus time units) is then multiplied by the conversion factor and GPCI, making anesthesia payment dynamic rather than flat.
Required documentation includes a pre-anesthetic evaluation with ASA physical status classification, a contemporaneous intraoperative anesthesia record with precise start and stop times, a post-anesthetic note, and medical necessity documentation aligning the ICD-10-CM diagnosis with the indication for lumbar sympathectomy. Supervision documentation is required when using modifiers QK, QX, QY, or AD.