ICD-10 Code M89.9: Disorder of bone, unspecified
M89.9 is billable for disorder of bone, unspecified, and the only M89 code that ...
Last Updated: August 6, 2026
ICD-10 Code Y76.8: Miscellaneous obstetric and gynecological devices is a billable ICD-10-CM code valid for all HIPAA-covered transactions.
Y76.8 captures OB/GYN devices not classified under Y76.0 through Y76.3, including uncommon or miscellaneous device types associated with adverse incidents.
Always document the specific device involved, the nature of the adverse event, and any resulting complications when reporting this code.
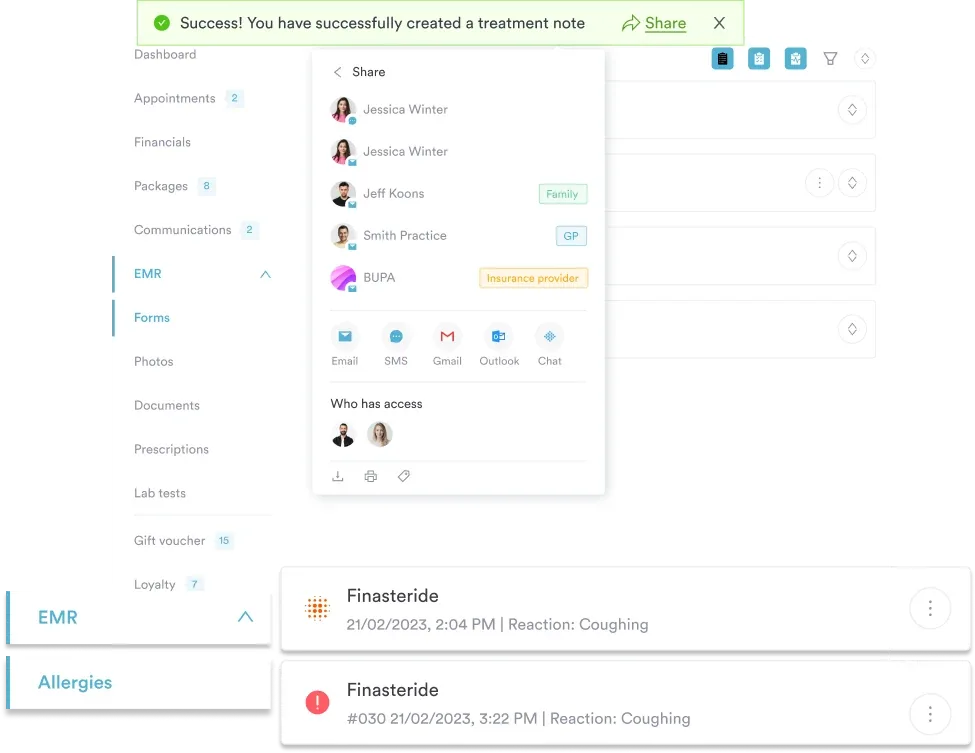
Pabau, practice management software for OB/GYN practices, supports structured clinical documentation and claims management workflows to help coders accurately capture device-related adverse incidents at the point of care.
ICD-10 Code Y76.8: Miscellaneous obstetric and gynecological devices associated with adverse incidents, not elsewhere classified is the billable external cause code for OB/GYN device malfunctions, breakage, leaks, or failures that don’t fit the more specific Y76.0 through Y76.3 subcodes. Getting this right matters for reimbursement, patient safety reporting, and audit readiness.
This reference covers the full clinical and billing context for OB/GYN practices using ICD-10-CM Y76.8: code definition, billable status, hierarchy, applicable to notes, excludes notes, clinical usage scenarios, documentation requirements, and sequencing guidance.
Y76.8 is a billable, specific ICD-10-CM diagnosis code. Per the Centers for Medicare and Medicaid Services (CMS), the 2026 edition of this code became effective on October 1, 2025.
This code belongs to the external cause code category, meaning it does not describe a patient’s disease or injury directly. Instead, it identifies the circumstance that caused or contributed to harm.
That circumstance is a malfunction, failure, breakage, or other adverse event involving an obstetric or gynecological device that falls outside the more specific Y76.0-Y76.3 subcodes. It is used alongside a primary diagnosis code describing the resulting condition.
The code is valid for all HIPAA-covered electronic transactions, making Y76.8 a reportable code for Medicare, Medicaid, and commercial payers. Coders should note that external cause codes like Y76.8 are generally reported as additional (secondary) diagnosis codes, not as the principal diagnosis.
For quick reference, the table below summarizes the core billing and classification data for Y76.8, drawn from the CDC/NCHS ICD-10-CM official lookup tool.
Understanding where Y76.8 sits in the ICD-10-CM hierarchy helps coders select the most specific code available. Specifically, external cause codes in the Y70-Y82 block all describe medical devices associated with adverse incidents.
To illustrate, the code tree for Y76.8 runs from the broadest classification down to the specific subcategory, as shown below.
The Y76 category contains five billable subcodes. Y76.8 is the residual “other” subcode for obstetric and gynecological device adverse incidents that do not fit into Y76.0 through Y76.3. The WHO ICD-10 classification underpins this structure, which the National Center for Health Statistics (NCHS), part of the CDC, adapted for the US ICD-10-CM implementation.
Before assigning Y76.8, verify the device type does not fit Y76.0 (diagnostic/monitoring), Y76.1 (therapeutic/rehabilitative), Y76.2 (prosthetic/implant), or Y76.3 (surgical instruments/sutures). Y76.8 is the claims-ready fallback when no more specific subcode applies.

Run a specificity check before using Y76.8. Review the device involved against Y76.0-Y76.3 descriptions. If the device is a fetal monitor, ultrasound probe, or intrauterine pressure catheter, Y76.0 likely applies. If it is a uterine balloon or cervical ripening device, check Y76.1. Y76.8 is reserved for devices that genuinely do not fit those categories.
The Applicable To notation in the ICD-10-CM tabular list clarifies which devices and scenarios fall within the scope of Y76.8. Per standard ICD-10-CM convention, the “.8” subcode captures obstetric and gynecological devices not elsewhere classified (NEC) within category Y76.
Devices that commonly fall under this code include miscellaneous or combination-use OB/GYN devices that do not fit the diagnostic, therapeutic, prosthetic, or surgical instrument categories.
The key inclusion criterion is that the device must be specifically designed for or used in obstetric or gynecological practice. A general-purpose hospital device used incidentally during an OB/GYN procedure would not qualify.
When in doubt, cross-reference with the AAPC ICD-10-CM code lookup and the official CMS tabular list for the most current Applicable To annotations before assigning this code.
Pabau helps OB/GYN clinics capture structured clinical notes, link device-related events to the right ICD-10 codes, and submit clean claims. See how it works for your practice.

The Y76 category carries excludes notes that restrict when codes in this category can be used alongside other diagnosis codes. Understanding these restrictions prevents claim denials related to incorrect gynecological device complication coding.
The Y70-Y82 block carries a general Type 2 Excludes note. It excludes later complications following the use of a medical device without breakdown or malfunctioning of the device. It also excludes surgical and medical procedures as the cause of an abnormal reaction or later complication in the patient, without mention of misadventure at the time of the procedure.
Both scenarios are coded to Y83-Y84 instead, not to Y76.8. In practice, this distinction trips up coders more than any other aspect of Y76.8 billing.
For coders handling fertility clinic billing, note that device complications occurring during fertility procedures may require careful review to determine whether the adverse event stems from the device or the underlying procedure. Use clinical documentation to distinguish the two before assigning Y76.8.
Check whether the adverse event is device-caused or procedure-caused before coding Y76.8. If the provider’s note says ‘uterine perforation during hysteroscopy due to instrument malfunction,’ that supports Y76.3 (surgical instrument) or Y76.8. If the note says ‘perforation occurred during insertion technique,’ the complication code set T80-T88 applies instead. The phrasing in the clinical note determines the code.
Y76.8 applies when a patient experiences harm or an unintended outcome directly attributable to an OB/GYN device that does not have a more specific Y76 subcode. The adverse incident can include device malfunction, breakage, leakage, disconnection, contamination, or failure to perform as intended.
Common clinical scenarios where this code may apply include newly marketed OB/GYN devices without established Y76.0-Y76.3 classification, combination-use accessories, or single-use devices whose function straddles multiple categories. In all such cases, use the structured clinical record to capture the device name, lot number, incident description, and resulting complication at the point of care.
Strong clinical documentation is the single most important factor in supporting a Y76.8 claim during audit. Without it, the code is unsupportable regardless of what happened clinically. Digital intake forms help standardize the documentation capture that coders need to assign Y76.8 accurately.
The clinical record must contain four elements to support this code:
OB/GYN practices using structured medical forms for adverse event reporting reduce coding ambiguity and improve first-pass claim acceptance rates. Standardized templates that prompt clinicians to identify the device type, failure mode, and resulting injury produce the documentation that coders need without requiring multiple chart queries.
Y76.8 is an external cause code and must always be coded in addition to a principal diagnosis that describes the resulting condition. It cannot stand alone as the only reported diagnosis on a claim. The principal diagnosis drives medical necessity and reimbursement, while Y76.8 provides context about the cause.
Common companion codes for Y76.8 include conditions that result directly from device failure. The sequencing rule is: principal diagnosis first (the injury or complication), then Y76.8 as an additional external cause code.
For practices managing complex OB/GYN billing, HIPAA-compliant documentation workflows ensure that the full code set for each adverse incident encounter is captured consistently. OB/GYN-specific EMR software can link device incident documentation directly to billing codes, streamlining the path from documentation to claims submission.
ICD-10-CM codes are updated annually by the National Center for Health Statistics (NCHS) and CMS, with new editions becoming effective October 1 of each year. The table below shows known validity for Y76.8 across recent fiscal years. The 2026 edition (effective October 1, 2025) is the current active version.
Y76.8 has not undergone description changes in recent update cycles. Coders should verify the current edition’s tabular list each October for any modifications to Applicable To or Excludes notes.
The CDC/NCHS ICD-10-CM tool reflects the most current published edition and is the authoritative source for code validation. OB/GYN practices benefit from reviewing the full tabular update each fiscal year, alongside related supply codes such as HCPCS Code A4322 for irrigation syringes.
Device-related adverse incidents in OB/GYN practice require precise external cause coding to support claims, audits, and patient safety reporting.
ICD-10 Code Y76.8: Miscellaneous obstetric and gynecological devices associated with adverse incidents, not elsewhere classified, is the correct residual code when the device involved does not fit the more specific Y76.0 through Y76.3 subcategories. Accurate selection depends on specificity review, strong clinical documentation, and correct sequencing alongside the principal diagnosis.
Pabau’s OB/GYN EMR helps practices build the structured documentation workflows that support accurate adverse event coding. To see how Pabau supports claims management and clinical record-keeping for OB/GYN teams, contact the team to discuss your practice’s needs.
Handling other external-cause coding scenarios? ICD-10 Code T87.42 covers infection of an amputation stump, another precise external-cause distinction coders need to get right.
Want to reduce documentation errors across your practice? Digital forms standardize adverse event capture so coders have the information they need before coding begins.
Coding other scenarios in your specialty? CPT Code 11423 and HCPCS Code J1459 are two related reference guides covering commonly coded conditions in multi-specialty practices.
ICD-10 Code Y76.8 is an external cause code for OB/GYN device adverse incidents not covered by Y76.0–Y76.3. It is always reported as an additional code alongside a principal diagnosis describing the resulting condition.
Yes. Y76.8 is valid for all HIPAA-covered electronic transactions. The 2026 edition became effective October 1, 2025.
Y76.0 = diagnostic/monitoring devices; Y76.1 = therapeutic/rehabilitative devices; Y76.2 = prosthetics and implants; Y76.3 = surgical instruments and sutures; Y76.8 = residual “other” category. Always use the most specific subcode before defaulting to Y76.8.
Always pair Y76.8 with a principal diagnosis code such as N93.8 (abnormal uterine bleeding), R33.9 (urinary retention), or T83.69XA (device-related infection). Sequence the injury or complication code first; Y76.8 follows as an additional external cause code.
The record must name the device, describe the failure mode, document the resulting condition, and confirm no more specific Y76 subcode applies. Structured adverse event forms reduce missing documentation and support first-pass claim acceptance.
No. ICD-10-CM coding and FDA MedWatch reporting are separate obligations. Assigning Y76.8 does not fulfill any requirement to report the device event to the FDA.