








ICD-10 Code K25.0: Gastric ulcer, acute with hemorrhage
ICD-10 Code K25.0 is a billable, specific ICD-10-CM code describing a gastric ul...
July 23, 2026
T86.10 is a billable ICD-10-CM diagnosis code for unspecified complication of kidney transplant, valid for FY2026 claims.
Use T86.10 only when the transplant complication cannot be specified as rejection (T86.11), failure (T86.12), infection (T86.13), or another defined type (T86.19).
Documentation must clearly establish a link between the patient’s kidney transplant history and the presenting complication to support T86.10 over an unrelated diagnosis code.
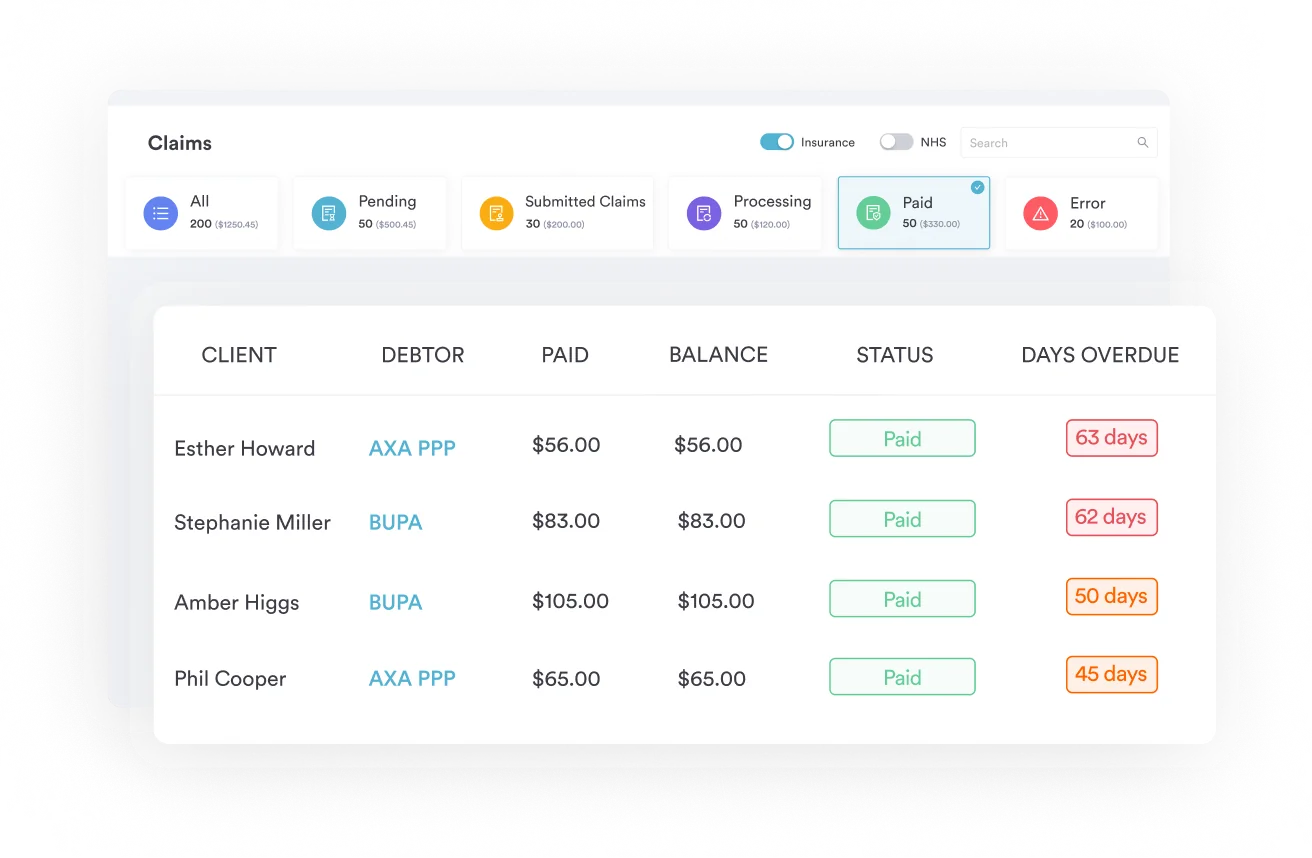
Pabau’s claims management software supports accurate diagnostic code submission and post-transplant documentation workflows for multi-specialty practices.
ICD-10 Code T86.10 is the billable ICD-10-CM diagnosis code for an unspecified complication of a kidney transplant. Coders assign it when the record confirms a transplant-related complication but does not specify whether it is rejection, failure, infection, or another defined type. It is valid for FY2026 claims and sits within the T86 category for complications of transplanted organs and tissue.
ICD-10 Code T86.10 covers unspecified kidney transplant complications, meaning encounters where the clinical record confirms a problem with the transplanted kidney but does not support a narrower diagnosis. According to the CDC/NCHS ICD-10-CM classification system, T86.10 falls under Chapter 19 (Injury, poisoning, and certain other consequences of external causes), within the T86 category block for complications of transplanted organs and tissue.
The full clinical descriptor for ICD-10 Code T86.10 is “Unspecified complication of kidney transplant.” Major coding references confirm its inclusion terms – “disorder of transplanted kidney” and related synonyms. The parent code T86 (Complications of transplanted organs and tissue) is non-billable; T86.10 is the billable child code coders use when the complication type is genuinely undetermined at the time of coding.
T86.10 is a valid, billable ICD-10-CM diagnosis code for FY2026. The CMS ICD-10 codes page and multiple authoritative coding reference databases confirm it as current. Coders should note the hierarchy carefully before submitting.
| Code | Description | Billable? |
|---|---|---|
| T86 | Complications of transplanted organs and tissue | No (non-billable parent) |
| T86.1 | Complications of kidney transplant | No (non-billable parent) |
| T86.10 | Unspecified complication of kidney transplant | Yes |
| T86.11 | Kidney transplant rejection | Yes |
| T86.12 | Kidney transplant failure | Yes |
| T86.13 | Kidney transplant infection | Yes |
| T86.19 | Other complication of kidney transplant | Yes |
Billing T86 or T86.1 directly will result in a claim rejection because neither code has billable/specific status. Payers accept only the five-character codes (T86.10 through T86.19). This mirrors how other ICD-10-CM diagnostic coding hierarchies work – parent codes signal a category; child codes carry the specificity needed for reimbursement.
The most common coding error in transplant care is defaulting to T86.10 when sufficient clinical information exists to support a more specific code. Payers and auditors look for this pattern – it signals incomplete documentation review rather than genuine clinical ambiguity.
Use T86.10 only when none of the following can be established from the clinical record:
T86.10 is appropriate when the encounter is for a post-transplant complication that the clinical record describes only in general terms – for instance, “kidney transplant complication, nature under investigation” – and no further specificity is obtainable from the available documentation at the time of coding. Coders relying on strong claims management software can flag these encounters for documentation queries before claim submission rather than defaulting to unspecified codes.
Before coding T86.10, query the treating provider for specifics. Ask whether rejection, failure, infection, or a defined complication type was established. A one-sentence clarification in the record can move a claim from T86.10 to a more specific code, reducing audit risk and strengthening medical necessity documentation.
Accurate coding of T86.10 depends on two things being present in the clinical record: a confirmed history of kidney transplant and a documented complication linked to that transplant. Missing either element creates a claim vulnerability. The same causal-link principle applies across ICD-10-CM diagnostic codes – the code must reflect what the record actually supports.
Post-transplant monitoring encounters present a specific challenge. Routine surveillance visits are not always separately coded with a complication code unless a complication is actually identified. When a complication is found during monitoring, the record must reflect the finding and its clinical significance. Using ICD-10-CM coding guidelines correctly means coding what is documented, not what is suspected.
Some ICD-10-CM coding references list a 7th character episode-of-care extension as applicable to codes within the T86 block. This claim requires caution. Based on the official ICD-10-CM tabular structure, many T86 subcategory codes – including T86.10 – do not require a 7th character extension in the way that injury codes in other Chapter 19 blocks do – such as ICD-10 code T75.29XS (Other effects of vibration, sequela), where the trailing S extension is mandatory.
Coders should verify the 7th character requirement directly against the official ICD-10-CM tabular list for the current fiscal year, as published by the CMS or CDC/NCHS. Some third-party lookup tools may display 7th character options inherited from parent-block instructions that do not apply to every child code within that block. Relying on a commercial tool without cross-checking the official tabular list is a known source of coding errors.
If a 7th character is required for a specific encounter, the standard options for applicable T86 codes include: A (initial encounter), D (subsequent encounter), and S (sequela). Document the episode of care clearly in the encounter record to support whichever character applies. Practices managing high volumes of post-transplant patients benefit from patient record management tools that surface transplant history and prior encounter data at the point of documentation.
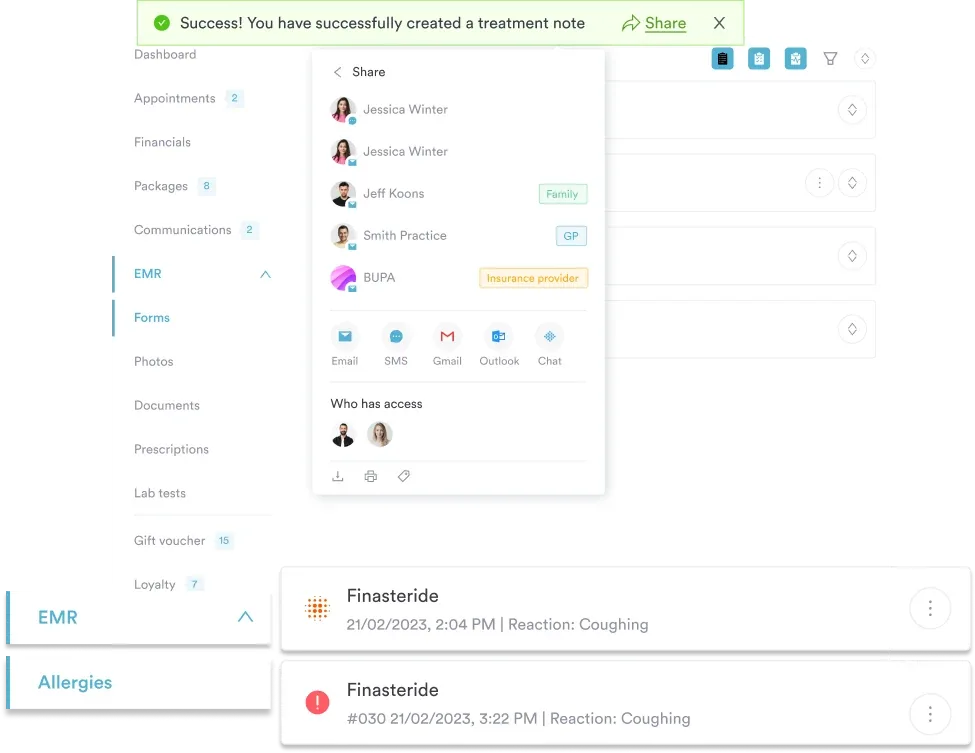
Pabau helps transplant care teams and multi-specialty practices maintain complete, auditable patient records – so coders have the documentation they need to assign the right ICD-10 code every time.

Kidney transplant complications sit within a larger T86 family that covers all transplanted organ types. Understanding the adjacent codes helps coders cross-check their selection and identify secondary code requirements that may apply. The AAPC Codify ICD-10-CM lookup provides the full T86 hierarchy for reference.
These parallel codes follow the same specificity logic as the T86.1x kidney codes. When a patient has received multiple transplants, code each organ’s complication separately with the applicable T86 subcategory.
Post-transplant lymphoproliferative disorder (PTLD) and other malignancies associated with transplanted organs require a specific coding sequence. The ICD-10-CM tabular instruction for the T86 block includes a “Use additional code” note directing coders to assign C80.2 (Malignancy associated with transplanted organ) when applicable. Sequence T86.10 or a more specific T86.1x code first, followed by C80.2, and then a code identifying the specific malignancy.
This multi-code sequence is one area where EHR integration for clinical coding delivers real value. Systems that link problem lists to coding workflows can prompt for secondary codes during documentation rather than relying on coders to recall complex instructional notes from memory.
When coding a post-transplant malignancy encounter, sequence the T86.1x kidney code first, then C80.2, then the specific malignancy code. Reversing this order is a common audit finding. Review the current ICD-10-CM Official Guidelines for Coding and Reporting for the exact sequencing rule applicable to your facility type.
Kidney transplant patients often present across multiple specialties – nephrology, infectious disease, transplant surgery, and primary care. Each encounter generates documentation that may or may not be accessible to the coder at the time of claim submission. This fragmented care model is where unspecified codes like T86.10 get overused.
A practical coding workflow for these encounters should include:
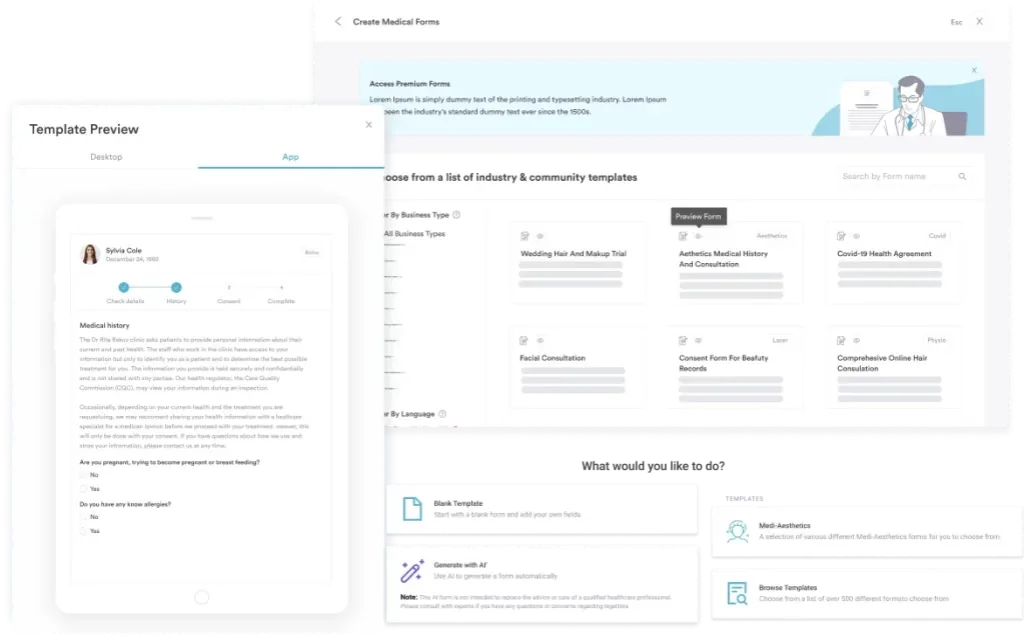
Practices supporting post-transplant patient care management at scale benefit from digital clinical documentation forms that capture transplant history, current immunosuppression, and complication status as structured fields – reducing the free-text ambiguity that leads to unspecified code assignments.
Unspecified codes are a legitimate part of ICD-10-CM – T86.10 exists because clinical reality sometimes produces complications that cannot be fully characterized at the time of coding. The risk is overuse. When providers document kidney transplant encounters with enough specificity to support T86.11, T86.12, T86.13, or T86.19, defaulting to T86.10 creates audit exposure and may not accurately reflect the clinical picture for future care decisions.
Pabau’s compliance management in transplant care workflows help practices build the documentation habits that support accurate coding from the first encounter. To see how Pabau supports multi-specialty and transplant care documentation teams, book a demo.
Need a reference for other ICD-10 diagnostic codes in your specialty? Intraparenchymal hemorrhage ICD-10 codes covers a parallel diagnostic coding reference for another high-complexity condition.
Managing complex patient records across multiple care episodes? Practice management software for clinics outlines how integrated platforms keep specialty-care documentation complete.
Want to streamline clinical documentation for HIPAA-compliant workflows? HIPAA compliance for clinic software walks through the documentation and security requirements for multi-specialty practices.
T86.10 is a billable diagnosis code for “Unspecified complication of kidney transplant,” used when a complication cannot be further specified as rejection, failure, infection, or another defined type at the time of coding. Valid for FY2026 claims under Chapter 19 of ICD-10-CM.
Use T86.10 only when the clinical record does not support a more specific code. If documentation establishes rejection, use T86.11; failure, use T86.12. T86.10 applies when the complication type is genuinely undetermined, under investigation, or documented only in general terms.
Some tools list 7th character options for T86 block codes, but verify this directly against the official ICD-10-CM tabular list for FY2026 from CMS or CDC/NCHS. Not all T86 subcategory codes require a 7th character, and third-party tools can mislead without cross-checking.
T86.10 is valid for Medicare claims, but payers may flag unspecified codes for additional documentation. Practices should review applicable Medicare Coverage Determinations and Local Coverage Determinations (LCDs) for transplant complication coding requirements.
Secondary codes depend on clinical context. Post-transplant malignancy requires C80.2 sequenced after the T86.1x code. Immunosuppressive therapy and infection organism codes may also apply. Check the T86 block’s “Use additional code” instructional notes for a full list.
For a post-transplant malignancy such as PTLD, code the kidney transplant code (T86.10 or a more specific T86.1x code) first, then C80.2 for the malignancy associated with the transplanted organ, followed by a code identifying the specific cancer. The T86 block’s “use additional code” note directs this order, and reversing it is a common audit finding.



