ICD-10 Code L88: Pyoderma gangrenosum coding reference
L88 is the billable ICD-10-CM code for pyoderma gangrenosum. One Excludes1 note ...
Last Updated: August 4, 2026
ICD-10 Code M27.1 identifies giant cell granuloma, central. It is a billable, specific ICD-10-CM code for this benign jaw lesion of the mandible or maxilla.
M27 (parent code) is non-billable: always use M27.1 for the central variant. The peripheral giant cell granuloma codes differently, typically under K06.8.
Documentation must confirm the central location and the histopathological findings. Vague jaw notes without anatomical specificity risk a claim denial under this code.
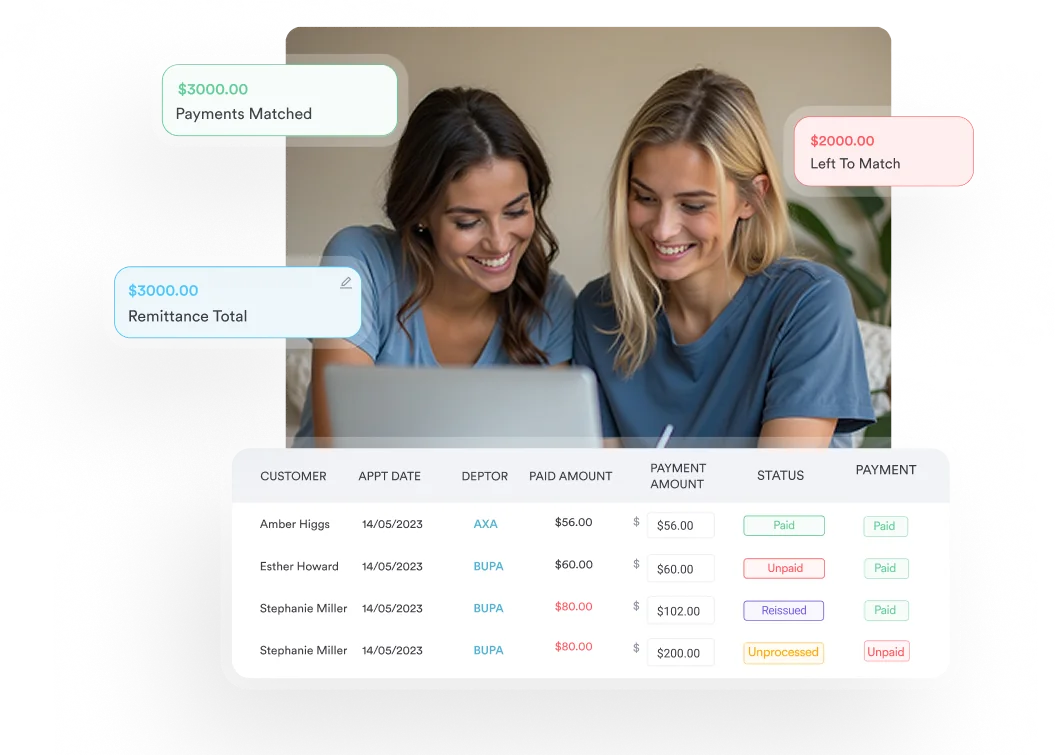
Practice management software like Pabau helps oral surgery and dental practices capture the structured documentation M27.1 billing requires. Its claims management tools and digital intake forms do the heavy lifting.
ICD-10 code M27.1 is the billable diagnosis code for giant cell granuloma, central. It marks a benign but locally aggressive lesion within the bone of the jaw. The code applies only when the lesion is central, meaning intraosseous. It does not cover the gingival soft-tissue form, which is the peripheral variant coded elsewhere.
For coders, the M27.1 giant cell granuloma code turns on one detail in the record. Is the lesion documented as central or peripheral?
Central giant cell granuloma (CGCG) is a non-neoplastic proliferative lesion. It occurs mainly in patients under 30, and it typically favors the anterior mandible.
Coders working in oral and maxillofacial surgery, dental oncology, and hospital-based dental services encounter M27.1 most often when processing excision or curettage claims. Getting the code right matters, because the two variants call for different procedural pairings. They also carry different clinical risk profiles.
In the ICD-10-CM tabular list, M27.1 also covers giant cell granuloma NOS (not otherwise specified). Reference tabular tools list reparative giant cell granuloma as a synonym too. So a documented central giant cell granuloma of the mandible or maxilla maps to this code.
The code sits within ICD-10-CM Chapter 13 (Diseases of the Musculoskeletal System and Connective Tissue, M00-M99). Its subcategory is M26-M27 (Dentofacial Anomalies and Other Disorders of Jaw). It is a billable, fifth-character-specific code. The parent code M27 (Other diseases of jaws) is non-billable and cannot be submitted for reimbursement.
The Centers for Medicare and Medicaid Services (CMS) sets the standard here. Valid ICD-10-CM code selection requires the highest level of specificity available in the tabular list. Submitting the parent M27 code when M27.1 exists counts as an unspecified submission. As a result, it often triggers payer queries.
For inpatient coding, M27.1 is not classified as a complication or comorbidity (CC) or a major complication or comorbidity (MCC). On its own it does not raise the DRG severity level, so the supporting documentation and correct principal diagnosis sequencing carry the weight on the claim.
M27.1 carries one Type 1 Excludes (Excludes1) note in the ICD-10-CM tabular list: peripheral giant cell granuloma (K06.8). An Excludes1 note means “not coded here.” The two conditions are mutually exclusive. So you cannot report M27.1 and K06.8 together for the same lesion.
If the granuloma is peripheral rather than central, K06.8 replaces M27.1 instead of joining it on the claim.
Confirm the current Excludes1 entries for M27.1 against the CDC/NCHS ICD-10-CM web tool, which reflects the current fiscal year’s official tabular list. Cached commercial lookup tools can show outdated Excludes notes after the annual October code updates.
Giant cell granuloma presents in two anatomically and histologically related but clinically distinct forms. The central variant (M27.1) arises within the medullary bone of the mandible or maxilla.
The peripheral variant arises from the gingival soft tissue or periodontal ligament, and it is coded separately. Typically that means K06.8 (Other specified disorders of gingiva and edentulous alveolar ridge). Even so, coders should verify the current tabular assignment.
The clinical note, imaging report, and pathology report together form the documentation triad that supports M27.1. Missing any one element creates vulnerability at audit.
Insufficient documentation is the main reason M27.1 claims face payer scrutiny. The record must establish three things. First, the central (intraosseous) nature of the lesion. Next, its location within the jaw, including the side where it applies. Finally, histopathological confirmation of giant cell granuloma.
Practices using digital intake forms can structure pre-procedure documentation to capture the specific anatomical site, relevant imaging findings, and clinical impression before the encounter is coded. This reduces the back-and-forth between coders and clinicians that typically delays claim submission.
The American Academy of Professional Coders (AAPC) and the American Health Information Management Association (AHIMA) agree on one rule. ICD-10-CM code selection must reflect the provider’s documented clinical judgment, not the coder’s inference. If the record says “probable giant cell granuloma” rather than a confirmed diagnosis, coding guidelines may require an alternative unconfirmed-diagnosis approach depending on the care setting.
Run a documentation check before submitting M27.1 claims: confirm the pathology report is filed in the patient record, the imaging report specifies intraosseous location, and the clinical note uses language consistent with central (not peripheral) origin. A 30-second pre-submission review catches most missing M27.1 documentation elements before they become denial letters.
M27.1 sits in a cluster of jaw disorder codes, and coders frequently need to distinguish it from adjacent codes during differential diagnosis situations. Selecting the wrong code from the M27 family is a common audit finding in oral surgery billing.
When the final diagnosis is not yet confirmed, knowing how related codes differ helps you avoid a premature or inaccurate assignment. The same clustered-code challenge shows up with M81.6, where distinguishing localized osteoporosis from other bone disorders depends on matching documentation to the right level of specificity.
Sometimes a biopsy is still pending, and the differential includes giant cell tumor or fibrous dysplasia. In that case, coding guidelines generally require coders to wait for pathological confirmation before assigning M27.1. Inpatient coding rules assign the condition to the highest degree of certainty at discharge. Outpatient rules, however, usually don’t allow coding an unconfirmed diagnosis as if it were established.
One distinction trips up coders most often: giant cell granuloma is not the same as a giant cell tumor. M27.1 is a benign, non-neoplastic jaw lesion, whereas a giant cell tumor of bone is a neoplasm classified under a different code family.
They share multinucleated giant cells on histopathology but code separately, so assign M27.1 only when the pathology report names giant cell granuloma, central.
A separate condition, M31.6, also involves giant cells on biopsy. However, it describes vascular inflammation with no relation to jaw pathology. In short, shared histology terms don’t imply shared coding.
Pabau helps dental and oral surgery practices capture structured clinical documentation, manage claims, and reduce denials, all in one place.

ICD-10 Code M27.1 functions as the diagnosis code. The procedural code (CPT) depends on the treatment approach documented in the operative report.
The two most common procedures for central giant cell granuloma differ by how aggressive the lesion is. Non-aggressive lesions call for enucleation with curettage (CPT 21030 or 21040). Aggressive lesions call for resection requiring osteotomy (CPT 21046 or 21047).
Practices with strong claims management software can build standard code pairings for M27.1 into their billing workflow. This cuts the manual lookup burden on coders, and it lowers code-mismatch denials. Oral and maxillofacial surgery coding is especially prone to CPT-ICD mismatch errors when the operative approach differs from the original plan.
The AMA’s CPT code set does not include a lesion-specific code for giant cell granuloma of the jaw. Coders select the closest anatomically and procedurally accurate CPT code based on the site (mandible vs. maxilla) and the surgical approach: enucleation and curettage for non-aggressive lesions, or resection requiring osteotomy for aggressive ones.
Always verify current CPT descriptors against the CMS Physician Fee Schedule before submitting.
Prior authorization requirements vary by payer. Oral and maxillofacial surgery procedures billed with M27.1 frequently require pre-authorization from commercial insurers, particularly when the CPT code selected involves significant bone excision. Practices should confirm payer-specific requirements before scheduling surgical intervention.
When pairing CPT codes with M27.1, keep the pathology report and operative report in sync. If the pathology report describes ‘central giant cell granuloma’ but the operative note describes a gingival soft-tissue excision, the code pairing will fail medical necessity review. Confirm the surgical access route matches the central (intraosseous) designation before submitting.
Dental and oral surgery practices that see jaw lesion patients benefit from a structured coding workflow that spans from the initial consultation through pathology receipt. Ad hoc coding, where the coder assigns M27.1 based on the clinical impression alone before pathology returns, creates audit exposure.
Skin clinic software, plastic surgery EMR platforms, and oral surgery practice management systems handle the documentation chain differently. But the core requirement is the same. Every code needs a matching document in the record to justify it.
Practices that store patient records digitally reduce the retrieval lag when payer audits or pre-payment reviews request supporting documentation.
The coding workflow for M27.1 typically follows four stages:
Practices using Pabau can attach pathology reports and imaging directly to the patient record, so the full documentation chain is available at the point of claim review. For broader documentation guidance, Pabau’s resource library covers structured intake and record-keeping best practices across specialties.
M27.1 is part of the ICD-10-CM code set. The Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) maintain it jointly. This work sits under the authority of the World Health Organization’s ICD-10 framework.
Annual updates to the ICD-10-CM tabular list take effect each October 1. So coders should verify the code’s active status, and any notation changes, at the start of each fiscal year.
The 2026 ICD-10-CM edition took effect on October 1, 2025, and M27.1 remains an active, billable code with no changes to its descriptor. So practices should monitor the CMS ICD-10-CM update files each year. Pay special attention to the Excludes notes, which can change without any change to the code descriptor.
Other codes within the same musculoskeletal chapter face similar specificity demands: M05.9 carries its own documentation requirements to confirm rheumatoid factor status before submission.
The WHO’s broader ICD framework, accessible via the WHO ICD-10 browser, classifies giant cell granuloma within the musculoskeletal chapter. The US clinical modification (ICD-10-CM) follows the same hierarchical placement, making M27.1 consistent across international and domestic coding frameworks.
Accurate ICD-10 code selection is part of the broader job of managing patient data. This matters most where records feed billing, clinical care, and population health reporting. Keeping client records current with confirmed diagnoses, updated code assignments after pathology, and documented care episodes protects practices during retrospective audits.
Claim denials for M27.1 rarely involve the code itself. They trace back to documentation that cannot confirm what the code asserts: an intraosseous lesion of the jaw, histopathologically confirmed as giant cell granuloma, central. Practices that treat documentation as a pre-coding step rather than a post-encounter formality submit cleaner claims and face fewer audit requests.
Pabau’s compliance management tools help oral surgery and dental practices build structured documentation workflows that support accurate ICD-10 code assignment across the full episode of care. To see how Pabau handles jaw disorder documentation in practice, book a demo.
Need guidance on related ICD-10 diagnostic coding? Intraparenchymal hemorrhage ICD-10 codes walks through documentation and code selection for another complex diagnosis category.
Looking for structured clinical intake workflows? Digital forms shows how Pabau captures structured pre-procedure data that supports accurate ICD-10 code assignment.
ICD-10 Code M27.1 is the billable ICD-10-CM diagnosis code for giant cell granuloma, central: a benign but locally aggressive fibrous lesion arising within the bone of the jaw (mandible or maxilla), characterized by multinucleated giant cells on histopathology. It falls under ICD-10-CM Chapter 13 (Musculoskeletal System and Connective Tissue), subcategory M26-M27.
Yes. M27.1 is a specific, billable ICD-10-CM code. The parent code M27 (Other diseases of jaws) is non-billable and cannot be submitted for reimbursement. Always use M27.1, not M27, when the confirmed diagnosis is central giant cell granuloma.
Central giant cell granuloma (M27.1) originates within the jaw bone itself (intraosseous), while the peripheral variant arises from gingival soft tissue and is coded separately, typically under K06.8. The distinction is critical because the procedural CPT code paired with the diagnosis must match the anatomical depth confirmed in the operative report. Mismatching the central code with a soft-tissue CPT triggers medical necessity review.
In outpatient settings, M27.1 should be assigned only after histopathological confirmation from the biopsy or pathology report. Before the biopsy result is available, code the presenting symptom (jaw mass, jaw pain) rather than the suspected diagnosis. Inpatient coding rules may differ; consult the official ICD-10-CM guidelines for setting-specific instructions.
The most common CPT codes paired with M27.1 are 21040 (excision of benign tumor or cyst of mandible; enucleation and/or curettage) and 21030 (excision of benign tumor or cyst of maxilla or zygoma; enucleation and curettage). For aggressive lesions requiring resection, CPT 21046 or 21047 (excision of benign tumor or cyst of mandible requiring intra-oral or extra-oral osteotomy) may apply. Verify current descriptors and fee schedule data via the CMS Physician Fee Schedule before submitting.
Peripheral giant cell granuloma is not coded under M27.1. As a soft-tissue lesion of the gingiva, it is typically reported under K06.8 (other specified disorders of gingiva and edentulous alveolar ridge), where it may also appear as giant cell epulis. M27.1 applies only to the central, intraosseous variant, so confirm the current tabular assignment before submitting.
No. Giant cell granuloma of the jaw (M27.1) is a benign, non-neoplastic lesion, while a giant cell tumor of bone is a neoplasm classified under a different code family. They share multinucleated giant cells on histopathology but code differently, so match the pathology report wording before assigning M27.1.
No. M27.1 is not classified as a complication or comorbidity (CC) or a major complication or comorbidity (MCC). On its own it does not raise the DRG severity level, so accurate documentation and correct principal diagnosis sequencing carry the weight on an inpatient claim.