ICD-10 Code Y76.8: Miscellaneous obstetric and gynecological devices
ICD-10 Code Y76.8: Miscellaneous obstetric and gynecological devices associated ...
July 15, 2026
ICD-10 Code H47.9 describes an unspecified disorder of visual pathways and is a billable ICD-10-CM diagnosis code valid for the 2026 fiscal year (effective October 1, 2025).
Use H47.9 only when a more specific H47.x code cannot be assigned; ICD-10-CM guidelines require coders to document why specificity was not achievable.
Payers may flag H47.9 for medical necessity review because unspecified codes carry higher audit risk; robust clinical documentation of symptoms, exam findings, and diagnostic workup is essential.
Practice management software like Pabau — with clinical records and claims management tools — helps ophthalmology and neurology practices document and submit H47.9 accurately, reducing denial risk on HIPAA-covered transactions.
ICD-10 Code H47.9 is a billable ICD-10-CM code for an unspecified disorder of visual pathways. Coders assign it when documentation doesn’t identify a more specific type, such as optic atrophy, papilledema, a chiasm disorder, or another named condition under H47.
It’s also the code payers’ audit systems flag most often, since unspecified codes carry a higher review risk than a specific, documented diagnosis.
This reference covers the definition, billable status, code hierarchy, sibling codes, documentation requirements, and billing considerations for ICD-10 Code H47.9, including a comparison table to help coders choose between H47.9 and more specific visual pathway diagnosis codes.
ICD-10 Code H47.9 is a billable/specific ICD-10-CM diagnosis code for Unspecified disorder of visual pathways. It is valid for use in HIPAA-covered transactions for the 2026 fiscal year, effective October 1, 2025.
The code falls under category H47, which covers other disorders of the optic (2nd) nerve and visual pathways, within Chapter H00-H59 (Diseases of the eye and adnexa) of the ICD-10-CM Tabular List.
Unlike a “not otherwise specified” code in older classifications, H47.9 in ICD-10-CM carries a specific clinical expectation: the coder must demonstrate from the documentation that the type of visual pathway disorder could not be determined at the time of the encounter.
According to CMS ICD-10 coding guidance, the unspecified code is appropriate only when no further specificity is documented or clinically knowable.
The table below summarizes H47.9’s key attributes as published in the 2026 ICD-10-CM edition, alongside other neuro-ophthalmic codes such as H57.01.
Optic nerve and visual pathway disorders sit within a clear four-level hierarchy in the ICD-10-CM Tabular List, home to sibling codes like H47.49. Understanding where H47.9 sits helps coders identify the correct level of specificity before assigning the unspecified code.
The sibling category H46 covers optic neuritis specifically. H47 is a broader category that holds disorders of the optic nerve beyond neuritis, plus disorders of the chiasm, visual cortex, and other visual pathway structures. H47.9 is the residual, catch-all code within H47 when no more granular sub-code applies.
According to the CDC/NCHS ICD-10-CM web tool, the full H47 category contains sub-codes ranging from H47.01 through H47.9, covering optic atrophy, papilledema, disorders of the chiasm, and visual cortex disorders before reaching the unspecified code.
Before assigning H47.9, coders should systematically review the sibling codes within H47. Each sub-code describes a specific type of optic nerve or visual pathway disorder, and many of them have their own further-specified sub-codes by laterality or etiology. The same last-resort logic applies to other catch-all codes across ICD-10-CM, such as M79.9: unspecified is always the last resort.
ICD-10-CM Official Guidelines for Coding and Reporting, maintained by CMS and NCHS, are clear: unspecified codes are acceptable when the clinical record does not allow for a more specific code assignment. For ICD-10 Code H47.9, that means the following scenarios are appropriate uses:
H47.9 should not be used as a convenience code when a more specific code is achievable. If the documentation clearly identifies optic atrophy, that is H47.2x. If the record specifies papilledema, that is H47.1x. And if the note documents only a subjective visual complaint without evidence of a pathway lesion, a symptom code such as other visual disturbances (H53.8) may describe the encounter more accurately than H47.9. The medical documentation workflows supporting the encounter note must justify why H47.9 was selected over those alternatives.
Payers scrutinize unspecified codes more than specific ones. The clinical note supporting ICD-10 Code H47.9 needs to do more than identify a symptom. It must create a complete clinical picture that explains why specificity was not achievable. Good clinical records management begins with structured note templates that prompt clinicians to capture this context at the point of care.
The note must include all of the following:
Using digital clinical forms with pre-structured fields for visual pathway disorders helps ensure clinicians capture the right details at each encounter, reducing the missing documentation that triggers payer queries.
Flag H47.9 claims for internal review before submission. Because unspecified codes carry a higher denial risk, a quick coder review confirming documentation supports the unspecified selection is a worthwhile safeguard, especially for Medicare and Medicaid encounters where LCD policies may apply.
ICD-10 Code H47.9 is a valid HIPAA-covered transaction code, but its unspecified nature means payers may apply heightened scrutiny. Ensuring HIPAA-covered transaction compliance goes beyond code validity: the submitted claim must pair H47.9 with CPT codes that are medically necessary for evaluating an unspecified visual pathway disorder, and the clinical record must support that pairing.
Common CPT codes billed alongside H47.9 in ophthalmology and neurology practices include evaluation and management codes, visual field testing, and imaging studies. Payer LCD (Local Coverage Determination) policies for visual pathway disorders vary, so verifying that the selected CPT-ICD pairing meets the specific payer’s medical necessity criteria is important before submission.
Use claims management software to track denial patterns by payer for H47.9 submissions.
Important: CPT-ICD pairing acceptability depends on the specific payer’s LCD/NCD policy. These pairings reflect general coding practice and should be verified against current payer policies before claim submission. The AAPC CPT-to-ICD-10 crosswalk tool can assist with medical necessity verification.
Ophthalmology practices using specialty practice software with integrated coding support can set up internal flags to review H47.9 claims before submission, helping reduce preventable denials.
Pabau helps ophthalmology and neurology practices document visual pathway disorders accurately, submit HIPAA-compliant claims, and track denial patterns by diagnosis code. See how it works for your practice.

The most common H47.9 coding error is selecting the unspecified code when the documentation supports a more precise assignment. This comparison table helps coders systematically evaluate whether H47.9 or a specific sibling code is appropriate. The CDC/NCHS ICD-10-CM tool is a reliable reference for confirming current code validity.
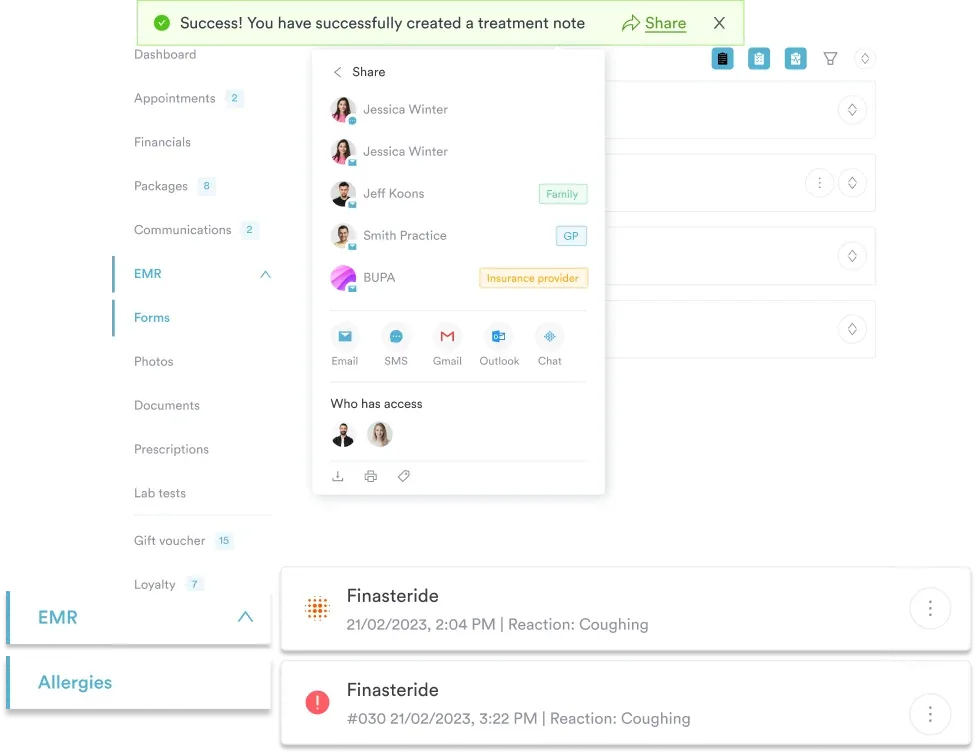
None of the leading ICD-10 reference pages for H47.9 address what happens inside the practice management system before a claim is submitted. That is where most coding errors are preventable. Pabau helps ophthalmology, neurology, and other specialty practices, including regenerative medicine practices, capture the clinical detail that supports accurate code selection at every stage of the patient encounter.
Pabau’s AI-assisted clinical documentation transcribes and structures consultation notes in real time, prompting clinicians to document examination findings, diagnostic orders, and clinical reasoning in a format that translates cleanly into ICD-10 coding decisions.
For a visual pathway disorder encounter, that means the structured note automatically captures the presenting symptoms, exam findings, imaging referrals, and the reason specificity was not achievable — creating the documentation trail that H47.9 claims require.
Pabau’s compliance management tools also help practices stay aligned with HIPAA transaction requirements as ICD-10-CM editions update each October, so coders are always working with current code validity status.
ICD-10 Code H47.9 fills a necessary but narrow role in visual pathway coding. It is the right code when specificity genuinely cannot be achieved, and the wrong code when the clinical record supports a more precise sibling assignment. The difference is almost always in the documentation.
Pabau’s structured clinical notes, integrated claims management, and denial-tracking workflows give ophthalmology and neurology practices the documentation infrastructure to use H47.9 correctly and defend those claims when payers ask. To see how Pabau handles ICD-10 coding workflows in practice, book a demo with our team.
Coding another catch-all diagnosis? M99.9 covers biomechanical lesions when the specific segment can’t be documented, the same specificity problem this page addresses for visual pathways.
Working with unspecified ENT codes? H66.93 walks through documentation requirements for bilateral otitis media when laterality and cause aren’t confirmed.
Need another example of an unspecified sensory-organ code? H83.19 covers labyrinthine fistula documentation when the affected ear isn’t specified.
ICD-10 Code H47.9 is used to document an unspecified disorder of visual pathways when the specific type of disorder cannot be determined from the available clinical information. It is a billable ICD-10-CM code valid for 2026 fiscal year claims, appropriate when a more specific H47.x code cannot be assigned.
Yes, H47.9 is a billable and specific ICD-10-CM diagnosis code. It is valid for submission on HIPAA-covered transactions for the 2026 fiscal year, effective October 1, 2025. However, being billable does not prevent payers from reviewing medical necessity for unspecified codes.
Use H47.9 only when the clinical documentation cannot support a more specific code assignment, such as when diagnostic workup is pending, imaging results are inconclusive, or the referring documentation does not identify the type of visual pathway disorder. If optic atrophy, papilledema, or another specific condition is documented, use the corresponding sub-code instead.
Ischemic optic neuropathy is coded to H47.01x, with a required 6th character for laterality (1 = right eye, 2 = left eye, 3 = bilateral, 9 = unspecified). Other optic neuropathies may be classified under H47.09x (other disorders of optic nerve, not elsewhere classified). H47.9 should not be used when the record specifies the type of neuropathy.
The clinical note must document presenting visual symptoms, ophthalmologic or neurological examination findings, diagnostic workup performed or ordered (such as OCT, MRI, or visual field testing), and an explicit or implied reason why the disorder type could not be specified. Notes that simply list H47.9 without supporting context are at risk of payer denial.