ICD-10 code S62.163P: Displaced pisiform fracture, malunion
ICD-10 code S62.163P is a billable diagnosis code for a displaced fracture of th...
Last Updated: August 7, 2026
ICD-10 Code F09 is a billable ICD-10-CM code for unspecified mental disorder due to a known physiological condition, effective October 1, 2025 for fiscal year 2026.
F09 applies only when a documented physiological condition causes the mental symptoms and no more specific F01-F06 code fits the presentation; code the physiological condition first, with F09 following as the manifestation code.
F09’s only Excludes1 notes are F06.7- and F29, and neither can be coded with F09; F01-F06 are more specific codes to rule out first, not formal excludes notes, and F09 carries no Excludes2 note.
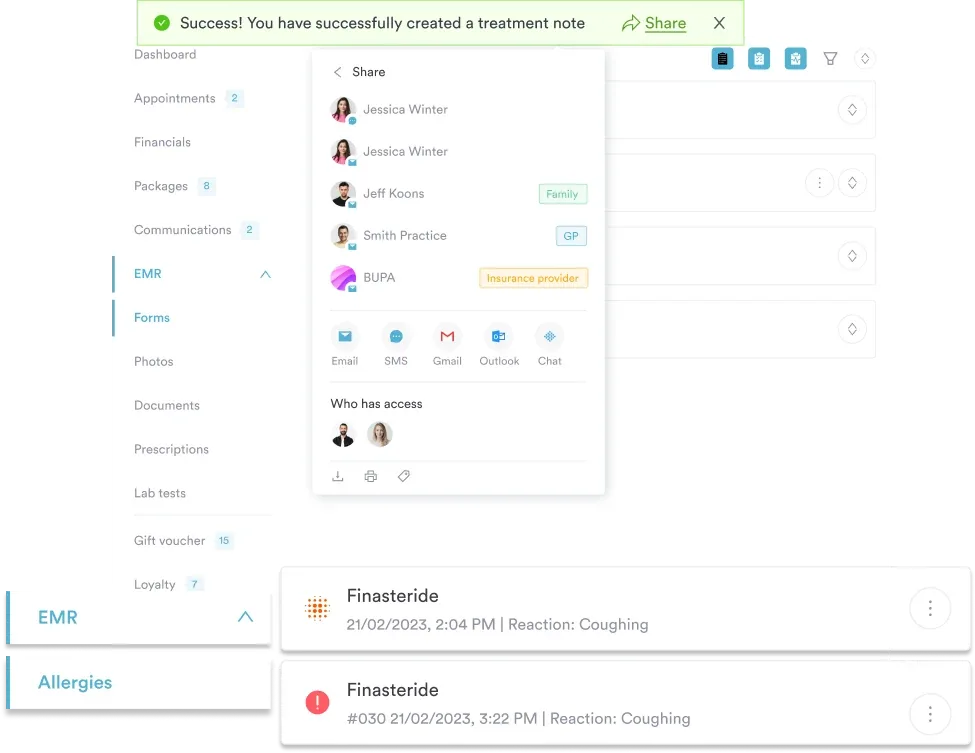
Practice management software like Pabau keeps the diagnosis, the physiological-condition link, and the medical-necessity narrative documented and audit-ready through structured intake forms and treatment-note workflows.
ICD-10 Code F09 is a billable ICD-10-CM code for unspecified mental disorder due to a known physiological condition. It sits at the end of the organic mental disorder block, reserved for cases where a physiological cause is confirmed but the presentation doesn’t fit any more specific code from F01 through F06.
This guide covers F09’s official description, excludes notes, DRG grouping, documentation requirements, how it compares with neighboring codes, its ICD-9 crosswalk, and a practical billing workflow for behavioral health practices.
ICD-10 Code F09 carries the official description Unspecified mental disorder due to known physiological condition. It sits at the tail of the F01-F09 block, which the CDC/NCHS ICD-10-CM tool classifies as “Mental disorders due to known physiological conditions.”
The word “unspecified” here does not mean the cause is unknown. It means the physiological cause is confirmed, but the mental disorder presentation does not meet the criteria for any more precise code in the F01-F06 range.
According to the Centers for Medicare and Medicaid Services (CMS), ICD-10-CM codes are updated annually, with FY 2026 changes effective October 1, 2025. F09 carries no revisions in the 2026 edition beyond the standard effective-date rollover.
The Applicable To note under F09 lists five synonym presentations. Each maps to the same code when documented alongside a confirmed physiological cause. Good patient care management means ensuring the underlying condition appears in the record before applying any of these aliases.
Note that “NOS” designations in ICD-10-CM are not interchangeable with “unspecified” in the payer sense. Coders should confirm that the physiological cause is explicitly linked to the mental symptoms in the clinical note before applying F09.
The excludes notes are where F09 claims most often go wrong. Excludes1 means the listed code is mutually exclusive with F09 and the two can never appear on the same claim. F01-F06 aren’t Excludes1 codes at all — they’re simply the more specific diagnoses to check before defaulting to F09.
F01-F06 aren’t Excludes1 codes for F09. They’re the more specific diagnoses in the same block, and the ICD-10-CM hierarchy expects coders to rule each of them out before F09 becomes appropriate.
F09 does not carry an official Excludes2 note in the ICD-10-CM Tabular List. F29 is sometimes miscast as an Excludes2 companion to F09, allowing both codes on one claim — that’s incorrect. F29 is an Excludes1 exclusion (see the table above), so it can never be coded alongside F09.
Understanding the F01-F09 block structure prevents the most common miscoding error: reaching for F09 before reviewing the more specific options. F09 is specifically the “catch-all” for cases where a physiological cause is confirmed but none of F01-F06 fits. Browse the full international classification in the WHO ICD-10 browser.
The same hierarchy logic applies to F07, the organic personality-disorder code in this block: confirm the physiological cause before ruling out F69 as the primary diagnosis.
For inpatient claims, F09 groups within specific Medicare Severity Diagnosis Related Groups (MS-DRGs). Relative weights change annually with the CMS IPPS final rule; confirm current weights before billing. The clinical documentation tools your practice uses should capture the diagnosis precisely so the grouper assigns the correct DRG.
F09 as the principal diagnosis groups to MS-DRG 884 only. Unlike many medical/surgical DRG families, MDC 19 (Mental Diseases and Disorders) doesn’t split by complication or comorbidity — there’s no MCC/CC/without-CC-MCC tier in this DRG family. DRGs 885 through 887 cover entirely different mental health diagnoses, not a more severe version of the same F09 case.
Don’t expect an F09 claim’s DRG to move based on comorbidities. If a grouper output shows a code outside 884-887 for an F09 principal diagnosis, check the diagnosis sequencing rather than assume a documentation gap — F09 as principal diagnosis groups to 884 regardless of what else is documented.
Coders cannot assign ICD-10 Code F09 without a clear clinical narrative supporting it. F09 carries a “Code first” instructional note in the Tabular List: the underlying physiological condition is sequenced first, with F09 following as the secondary, manifestation code.
Payer audits for unspecified mental disorder codes routinely target documentation gaps and sequencing errors. A solid psychiatric evaluation template helps clinicians capture exactly what auditors look for. Your practice management software should flag incomplete documentation before claims leave the system.
Three elements must be present in the clinical record before F09 is coded:
HIPAA-compliant recordkeeping practices, covered in detail in our guide to HIPAA compliance for medical offices, require that clinical rationale is preserved and retrievable for audit. For mental health EMR users, built-in structured note templates reduce the risk of documentation gaps that auditors flag.
The most common miscoding errors around F09 involve F05, F29, F99, and the F06 subcategories. F99 is the mirror image of F09: it applies when no physiological or organic cause is identified, while F09 requires that cause to be confirmed and documented.
The F09 vs F29 distinction is clinically significant. F29 indicates psychosis of unknown or primary etiology.
If a physiological condition is documented and the clinician attributes the psychosis to it, F09 (or the more specific F06.0 or F06.2) applies, not F29. Misapplying F29 when a physiological cause is documented wastes the specificity that the ICD-10-CM Official Guidelines for Coding and Reporting require.
Practices managing legacy records or conducting historical data analysis need the ICD-9-CM crosswalk. As with all crosswalk data, the General Equivalence Mappings (GEM) files published by CMS and NCHS provide the authoritative reference — and GEMs are approximate, many-to-many mappings, not a clean one-to-one match to F09. Verify crosswalk accuracy using the AAPC ICD-10-CM lookup before updating historical records.
Crosswalks for F09 are approximate and many-to-many, not one-to-one. The ICD-9-CM codes 293.9, 294.8, and 294.9 mapped broadly to organic mental disorders; GEMs route most of that group primarily to F06.8, with F09 as a secondary approximate match. When converting historical records, review each case clinically rather than defaulting to F09.
Claims carrying unspecified codes draw more review than specific codes. The steps below reflect a practical workflow for behavioral health and psychiatry practices attaching F09 to outpatient or inpatient claims.
Pabau helps behavioral health and psychiatry practices capture the physiological-condition link, structure the clinical narrative, and keep documentation audit-ready with digital intake and treatment-note workflows. See how it works in a live demo.

Practices using psychiatry EMR software with built-in diagnosis workflows can pre-populate the F09 code from the documented physiological condition and flag the encounter for secondary diagnosis entry before the claim goes out. This catches the most common denial trigger: F09 submitted without the underlying condition code.
Run a monthly audit of all claims submitted with F09 as the principal diagnosis. Pull the denial rate and compare it to the overall practice denial rate. A significantly higher denial rate for F09 claims signals a documentation gap, not a coding error. The fix is almost always in the clinical note, not the code selection.
F09 has been part of the ICD-10-CM tabular list since the US transition from ICD-9-CM. The code has carried no description changes through the 2026 edition. The FY 2026 update became effective October 1, 2025, consistent with the annual CMS update cycle co-managed with the National Center for Health Statistics (NCHS).
ICD-10 Code F09 is a legitimate, billable diagnosis for organic mental disorder presentations that defy more specific classification. The code works when documentation is tight: the physiological cause named, the causal link stated, and every F01-F06 option ruled out. Without that clinical foundation, F09 claims stall or deny.
Practice management software like Pabau helps psychiatry and behavioral health practices build the documentation workflow that supports F09 accuracy — structured intake forms, treatment notes that capture the physiological-condition link, and secondary diagnosis fields that stay attached to the claim. Book a demo to see how Pabau keeps diagnostic code documentation organized from the clinical note onward.
Need a framework for documenting the causal chain behind a behavioral episode? Behavior chain analysis worksheet gives clinicians a structured format for the same kind of causal documentation F09 coding requires.
Supporting patients between behavioral health sessions? Asking for help worksheet gives patients a simple prompt for identifying when and how to reach out for support.
Billing for home-based behavioral health visits? 99350 covers the billing requirements for extended home visit encounters, common for homebound patients with organic mental disorders.
ICD-10 Code F09 is a billable ICD-10-CM diagnosis code for unspecified mental disorder due to known physiological condition. It applies when a confirmed physiological condition causes mental symptoms that do not meet criteria for any more specific code in the F01-F06 range, effective October 1, 2025 for fiscal year 2026.
Yes. F09 is a billable and specific ICD-10-CM code that can be submitted on claims for reimbursement. Documentation must confirm the physiological cause and explain why no more specific organic mental disorder code applies.
F09 applies when a known physiological condition causes the mental disorder; F29 (unspecified psychosis) applies when there is no identified physiological or substance-related cause. If a physiological condition is documented and causally linked to psychotic symptoms, F09 or a more specific F06 code applies, not F29.
Organic brain syndrome refers to mental dysfunction caused by a physiological or structural condition affecting the brain. In ICD-10-CM, “organic brain syndrome NOS” is listed as an Applicable To alias under F09, meaning it codes to F09 when no more specific organic mental disorder code fits the presentation.
The approximate ICD-9-CM predecessors for F09 are codes 293.9 (unspecified transient mental disorder in conditions classified elsewhere), 294.8 (other persistent mental disorders due to conditions classified elsewhere), and 294.9 (unspecified persistent mental disorders due to conditions classified elsewhere). GEMs route most of this group to F06.8, with F09 as a secondary match; verify clinical context before updating historical records.
The physician must document the specific physiological condition, explicitly link it to the mental symptoms, and indicate that the presentation does not meet criteria for a more specific code (F01-F06). The NOS qualifier should reflect a clinical determination, not incomplete evaluation.