ICD-10 code S12.150K: Subsequent encounter for nondisplaced C5 fracture
Most cervical fracture denials trace back to a single documentation gap: the wro...
Last Updated: July 28, 2026
ICD-10 code B49 (Unspecified mycosis) is a billable ICD-10-CM diagnosis code for fungal infections not classifiable to a more specific mycosis code in the B35-B49 range.
Use B49 only when clinical evidence confirms a fungal infection but the causative organism or anatomical site cannot be determined from available diagnostic data.
Payers may query B49 if a more specific code exists in the patient record. Thorough documentation of the diagnostic workup is essential to justify the unspecified code and withstand audit.
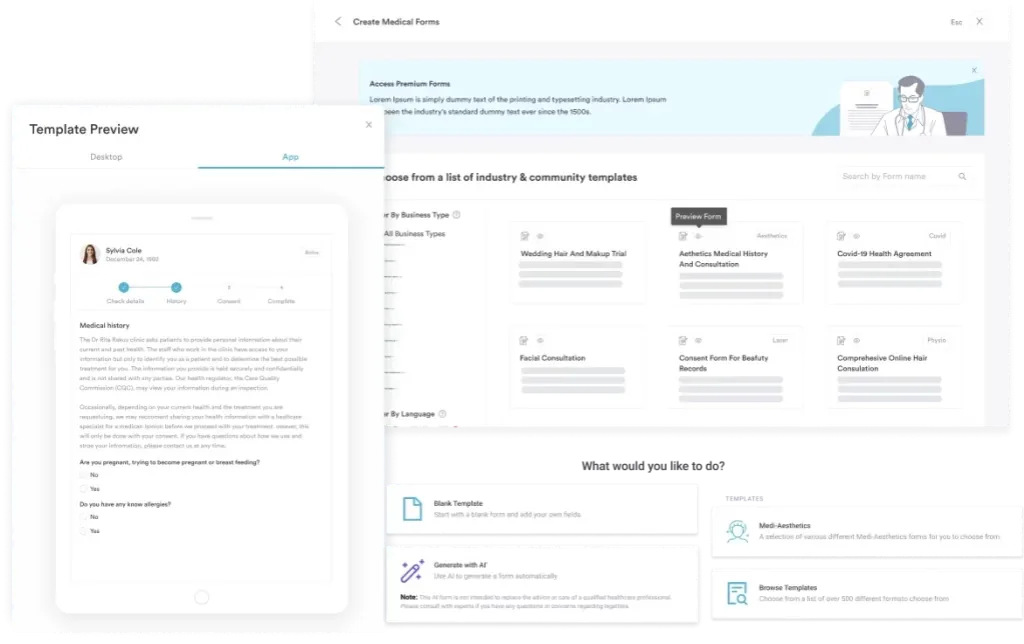
Pabau’s claims management software and digital clinical documentation forms help reduce coding errors and support audit-ready fungal infection records.
ICD-10 code B49 is the diagnosis code for an unspecified fungal infection, listed officially as unspecified mycosis. It is the ICD-10 code for a fungal infection that is confirmed but cannot be tied to a specific organism or site. B49 is billable and confirmed by the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS), valid on claims from fiscal year 2016 through the current FY 2026 code set.
| Code | Description | Chapter | Category Range | Billable |
|---|---|---|---|---|
| B49 | Unspecified mycosis | Certain Infectious and Parasitic Diseases (A00-B99) | Mycoses (B35-B49) | Yes |
Under the WHO ICD-10 classification hierarchy, B49 sits at the terminal position of the B35-B49 Mycoses block, which itself falls within Chapter 1 (A00-B99: Certain Infectious and Parasitic Diseases). It carries a single Applicable To note: Fungemia NOS (not otherwise specified), meaning bloodstream fungal infection of unspecified organism.
B49 has no subcodes. As a result, it is a leaf-level code, which means coders can use it directly on a claim without further specification. This distinguishes it from parent-level codes such as B37 (Candidiasis) or B44 (Aspergillosis), which carry subcodes that coders must select when the site or organism is known.
B49 applies in a narrower set of circumstances than many coders assume. The ICD-10-CM Official Guidelines for Coding and Reporting, maintained jointly by CMS and NCHS, instruct coders to assign the most specific code supported by the clinical documentation. B49 is the correct selection only when all three conditions below are met.
In practice, the most common legitimate B49 scenario is a systemic fungemia where blood cultures grow fungal elements but species identification is pending or inconclusive at the time of billing. A second scenario is a patient with immune suppression and clinical signs that point to a deep fungal infection, yet biopsy results stay non-specific. Both situations can justify B49, as long as the documentation reflects the diagnostic reasoning clearly.
Practice management software like Pabau, with digital clinical documentation forms that prompt for organism identification and anatomical site at the point of care, helps capture the data that allows coding to a specific code. That reduces reliance on B49 and lowers audit risk. Where data is genuinely absent, those same structured forms create the documented trail that justifies the unspecified code.
B49 carries a single Applicable To note: Fungemia NOS. When the record documents a fungus in the bloodstream but no organism is named, B49 is the correct fungemia ICD-10 code. This is the most common legitimate use of B49 in hospital coding.
The distinction that trips coders up is what happens once the blood culture returns. As soon as the organism is named, B49 no longer applies. Candidemia, the most frequent fungemia, is coded B37.7 (Candidal sepsis), not B49. A systemic fungal infection with an identified organism always moves to its specific code in the B35-B48 range. Reserve B49 for the window when fungemia is confirmed but speciation is still pending or inconclusive.
The ICD-10-CM tabular list and major reference databases list a range of synonyms and inclusion terms associated with B49. These are conditions for which the classification defaults to the unspecified mycosis code when a more specific code cannot be assigned.
Coders working in ID (infectious disease), oncology, and critical care settings encounter B49 most frequently. For example, immunocompromised patients, including those on chemotherapy or biological agents, post-transplant patients, and patients with advanced HIV, carry elevated fungal infection risk without always having a confirmed organism at the time of the clinical encounter. Each of these presentations may legitimately use B49 when documentation supports it.
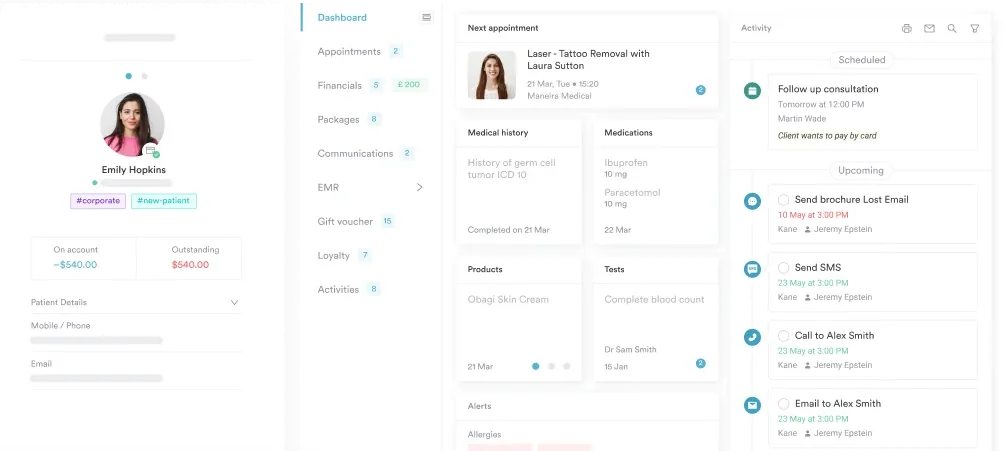
For coders in dermatology or primary care, B49 is rarely the right pick. Most cutaneous fungal infections have identifiable organisms and map to specific codes within B35-B48. A coder who regularly assigns B49 in outpatient dermatology should audit their workflow, as this may signal incomplete intake documentation rather than genuinely unidentifiable infections. Structured intake using structured client records reduces this risk.
Audit your B49 use rate quarterly. A high frequency of B49 assignments across dermatology or primary care encounters typically signals a documentation gap rather than a genuine diagnostic gap. Review whether intake forms capture organism type and anatomical site at triage.
The B35-B49 block contains 15 categories, each representing a distinct mycosis type. Selecting the correct code requires knowing which organism or site the patient’s condition maps to. The table below summarizes the most commonly referenced codes in this range, using ICD-10 guidance from the CDC/NCHS ICD-10-CM web tool.
Two Type 2 Excludes notes govern the B35-B49 block as a whole. Specifically, the block excludes hypersensitivity pneumonitis due to organic dust (codes in J67), along with mycosis fungoides (C84.0). Neither of these conditions should receive a B35-B49 code. For this reason, coders should not confuse mycosis fungoides (a T-cell lymphoma with a misleading name) with a true fungal infection.
Payers are more likely to query an unspecified code than a specific one, because unspecified codes signal incomplete diagnostic workup. In addition, using B49 without supporting documentation is the fastest way to a denial or a medical review letter. The following documentation elements should appear in the patient record when B49 is assigned.
Practices that rely on compliance management tools within their practice management platform are better positioned to enforce documentation standards at the point of care, reducing post-submission queries.
For outpatient claims, code only what the provider has confirmed during the encounter. Uncertain diagnoses (“probable,” “suspected,” “rule out”) cannot be coded as confirmed in the outpatient setting under UHDDS guidelines. B49 should only appear on an outpatient claim when the clinician has confirmed a fungal infection, even if the organism is not known.
By contrast, for inpatient coding, the Uniform Hospital Discharge Data Set (UHDDS) guidelines permit coding uncertain diagnoses as confirmed. A patient discharged with a working diagnosis of “probable fungemia” may be coded B49 on the inpatient claim. Coders should apply this guideline carefully and ensure the discharge summary clearly reflects the qualifying language.
When assigning B49 for inpatient stays, include the attending physician’s discharge summary language in your audit file. Words like ‘probable,’ ‘likely,’ or ‘presumed’ in the inpatient discharge summary are sufficient to support B49 under UHDDS guidelines. The same language would not support B49 on an outpatient claim.
Practices transitioning legacy records or running parallel billing systems still encounter ICD-9-CM mycosis codes. The ICD-9-CM classified mycoses in the range 110-118, using a substantially different structure than the current B35-B49 block. The crosswalk below reflects the general mapping used during the October 2015 ICD-9 to ICD-10 transition.
| ICD-9-CM Code | ICD-9 Description | ICD-10-CM Equivalent | Notes |
|---|---|---|---|
| 117.9 | Other and unspecified mycoses | B49 | Primary ICD-9 crosswalk to B49 |
| 117.3 | Aspergillosis | B44.9 | Maps to Aspergillosis, unspecified |
| 117.5 | Cryptococcosis | B45.9 | Maps to Cryptococcosis, unspecified |
| 112.9 | Candidiasis of unspecified site | B37.9 | Maps to Candidiasis, unspecified |
| 110.9 | Dermatophytosis of unspecified site | B35.9 | Maps to Dermatophytosis, unspecified |
For coders cross-referencing legacy records, the AAPC Codify ICD-10-CM code reference provides a searchable crosswalk tool alongside the official code descriptions. The ICD-9 range 110-118 mapped to 15 distinct ICD-10 categories. Therefore, coders should not assume a one-to-one relationship: many ICD-9 codes split into several more specific ICD-10 codes, and the reverse mapping can also produce multiple candidates.
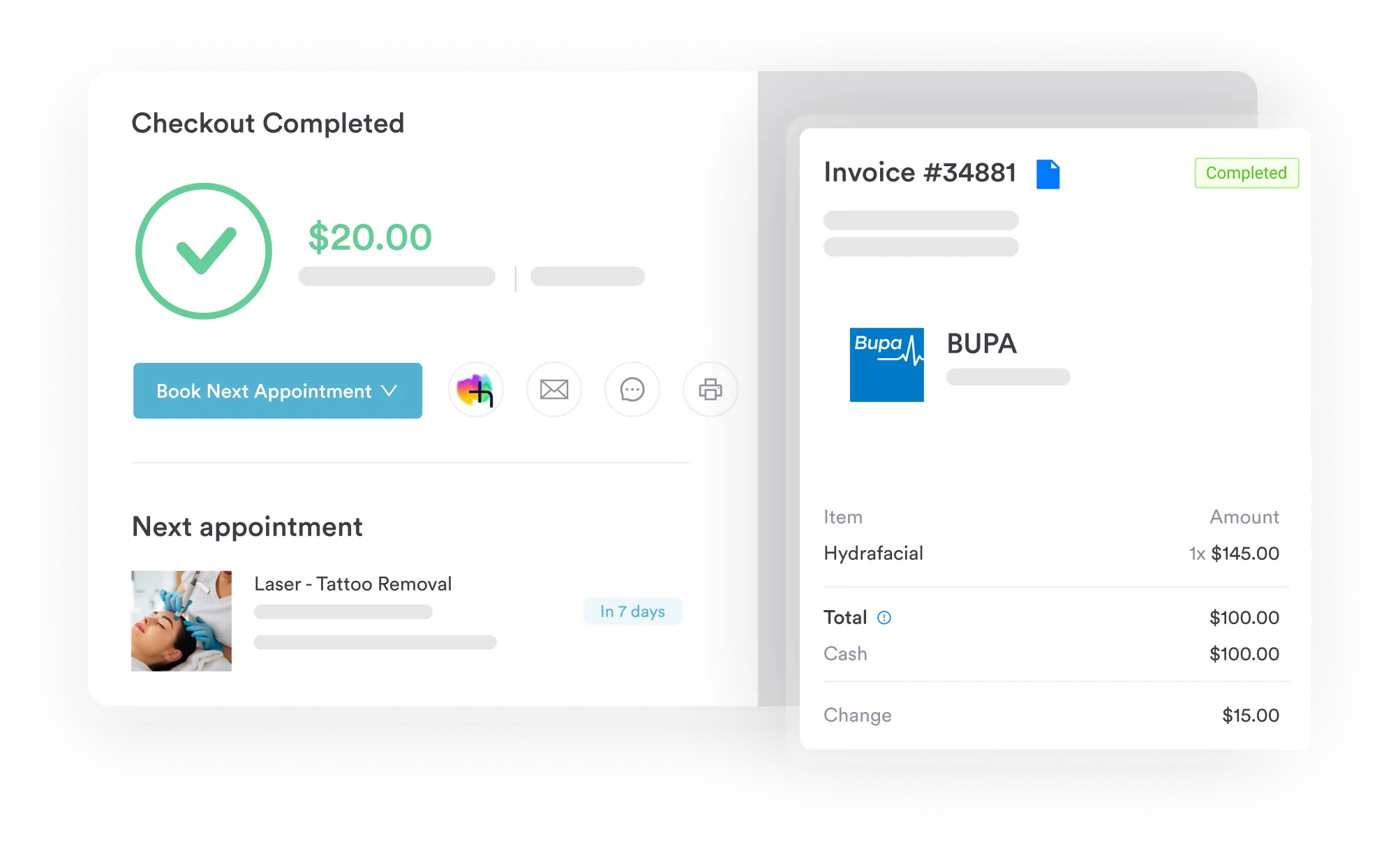
Pabau's claims management and documentation tools help practices code accurately, capture complete diagnostic data, and submit cleaner claims. See how it works for your clinic.

Unspecified codes do not automatically result in denial, but they do increase scrutiny. For this reason, several payer dynamics are worth understanding before submitting claims with B49.
Antifungal agents, particularly intravenous formulations such as echinocandins and amphotericin B, often require prior authorization. Payers typically want a diagnosis code that reflects the severity and specificity of the infection. A claim for IV antifungal therapy paired with only B49 may trigger a clinical review requesting additional documentation. Preparing the authorization request with the diagnostic workup notes and treatment rationale reduces back-and-forth.
CMS instructs providers that code selection must reflect the highest degree of specificity supported by the medical record. A Medicare contractor auditing a claim coded B49 will look for evidence that a more specific code was not available. Practices with consistent B49 assignment patterns without documented diagnostic attempts are at higher risk of Targeted Probe and Educate (TPE) review. Accurate claims management software that surfaces coding inconsistencies before submission is the most practical safeguard. For context on broader diagnostic code documentation patterns, see our reference on ICD-10 documentation requirements for complex diagnoses.
AHIMA and AAPC both support clinical documentation improvement (CDI) querying when a record is ambiguous. If a patient encounter clearly involved a fungal infection but the provider note does not specify the organism or cannot because results are pending, a concurrent query to the attending physician can result in an addendum that either confirms B49 as correct or allows assignment of a specific code once results return. Retroactive queries are also acceptable when the record is incomplete at the time of billing.
Practices with AI-powered clinical documentation tools can capture diagnostic reasoning and pending result references at the time of the encounter, reducing the need for post-encounter queries.
ICD-10 code B49 is a narrow, specific-use code that applies when a fungal infection is confirmed but neither the organism nor the site can be coded more precisely. Getting it right means understanding the full B35-B49 range, capturing adequate documentation at the point of care, and knowing how payers evaluate unspecified codes during audit.
Practices that build structured documentation workflows into their systems make accurate mycosis coding a natural output rather than an afterthought. Pabau’s practice management platform supports clinicians and coders with structured records, claims workflows, and documentation tools designed to reduce specificity gaps. To see how it works in your practice, book a demo.
Need to understand how ICD-10 diagnostic codes affect dermatology billing? Dermatology EMR software covers how Pabau supports accurate coding and documentation for skin and fungal conditions.
Want to go paperless with clinical documentation? Going paperless in healthcare explains how digital documentation reduces audit risk and improves coding accuracy.
ICD-10 code B49 is a billable ICD-10-CM diagnosis code representing an unspecified fungal infection (mycosis) where the causative organism or anatomical site cannot be determined from the clinical record. It falls within the B35-B49 Mycoses category in Chapter 1 of the ICD-10 classification (Certain Infectious and Parasitic Diseases, A00-B99). It carries one Applicable To note: Fungemia NOS.
Use B49 only when three conditions are met: the provider has confirmed a fungal infection, the specific organism has not been identified, and the anatomical site cannot be mapped to a more specific code in the B35-B48 range. B49 is not appropriate for suspected or probable fungal infections in outpatient settings, and it should never be assigned when a specific organism such as Candida (B37) or Aspergillus (B44) is known.
Yes. B49 is a valid, billable, specific ICD-10-CM diagnosis code confirmed through FY 2026. It has no subcodes and can be used directly on a claim. It has been billable in every ICD-10-CM edition since the October 2015 transition from ICD-9-CM.
The primary ICD-9-CM equivalent of B49 is code 117.9 (Other and unspecified mycoses). The broader ICD-9 mycosis range, 110-118, mapped to the current ICD-10 B35-B49 block during the October 2015 transition. Coders should use an official crosswalk tool rather than relying on the general range mapping, as several ICD-9 codes expanded into multiple ICD-10 codes.
Synonyms and inclusion terms associated with B49 include: Fungemia NOS (the primary Applicable To entry), abscess of intracranial subdural space caused by fungus, abscess of spinal cord caused by fungus, unspecified fungal infection, and mycosis of unspecified organism. These represent conditions for which B49 is the correct default when a more specific code in B35-B48 is not supported by the clinical record.
B49 is the ICD-10 code for an unspecified fungal infection, listed officially as unspecified mycosis. Assign it only when a fungal infection is confirmed but the organism and anatomical site cannot be determined. If the record names the organism such as Candida or Aspergillus, or a clear skin site, use the specific code in the B35-B48 range instead.
Most skin fungal infections are not coded B49. Dermatophytosis such as ringworm and tinea maps to B35, and candidiasis of the skin maps to B37.2. The unspecified mycosis code applies to a cutaneous infection only when the organism genuinely cannot be determined, which is rare in dermatology.