Obesity nursing care plan: Current NANDA-I diagnoses
Download your free obesity nursing care plan template A ready-to-use plan coveri...
Last Updated: August 6, 2026
An insulin resistance levels chart gives clinicians quick reference thresholds for HOMA-IR, fasting insulin, and fasting glucose to stratify metabolic risk.
HOMA-IR below 1.0 indicates normal insulin sensitivity, 1.0-1.9 is borderline, 2.0-2.9 suggests insulin resistance, and 3.0 or higher indicates severe resistance.
Female-specific HOMA-IR cut-offs differ from male cohort data. PCOS amplifies insulin resistance and requires contextual interpretation alongside clinical presentation.
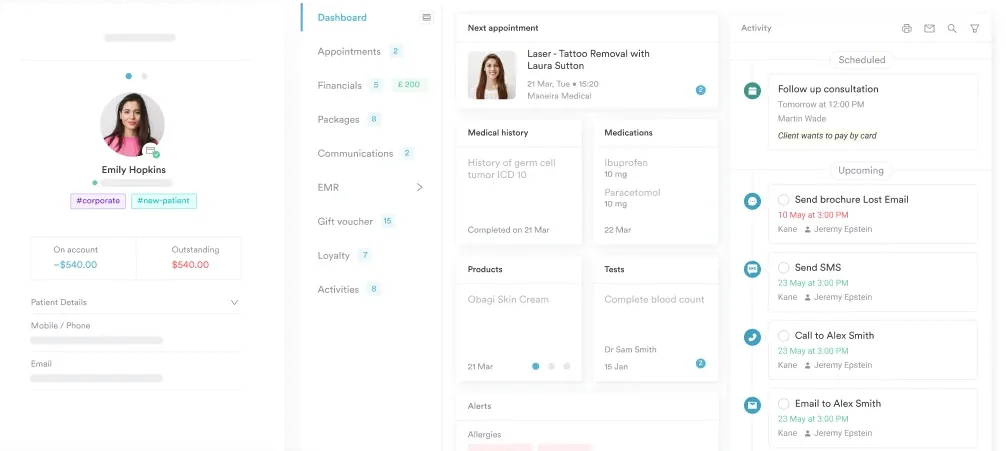
Pabau’s digital forms and client records help clinicians document metabolic panel results, track trends, and link lab findings directly to patient consultations.
A downloadable clinical documentation template for recording insulin resistance assessments in the patient chart. It includes patient and test-date fields, a fasting insulin reference range, with space to record results by age group, and structured sections for interpretation, clinical insights, dietary recommendations, and multi-visit progress tracking. Use it alongside the HOMA-IR, fasting glucose, and HbA1c reference ranges covered in this guide.
Download templateClinicians assessing metabolic health often juggle multiple reference ranges across different lab reports. An insulin resistance levels chart centralizes the key diagnostic thresholds in one visual resource, enabling faster patient risk stratification and clearer documentation of metabolic findings during consultations.
This guide explains how to use the chart, what each marker means, and why female-specific guidance matters when interpreting insulin resistance in PCOS and other populations.
An insulin resistance levels chart is a clinical reference tool that displays diagnostic thresholds for biomarkers used to assess and stage insulin resistance.
It helps practitioners quickly categorize fasting insulin, HOMA-IR scores, fasting glucose, HbA1c, and metabolic panel markers into normal, borderline, and pathological ranges.
Insulin resistance develops when cells become progressively less responsive to circulating insulin, forcing the pancreas to secrete more insulin to maintain glucose homeostasis.
Untreated, this compensatory hyperinsulinemia can progress to prediabetes, type 2 diabetes, and metabolic syndrome. Early detection via the chart enables timely lifestyle and pharmacological intervention.
The HOMA-IR ranges in this chart come from peer-reviewed endocrinology literature and standard clinical practice. Neither the Endocrine Society nor the American Diabetes Association (ADA) publishes an official HOMA-IR cut-off.
The ADA’s own diagnostic criteria for prediabetes and diabetes are based on fasting glucose, HbA1c, and oral glucose tolerance testing, while the Endocrine Society’s guidelines address related metabolic conditions.
This chart serves as both a patient education tool and a clinician-facing documentation framework for metabolic health EMR workflows.
This structured workflow transforms scattered lab values into a clinician-friendly snapshot that informs diagnosis, risk stratification, and follow-up planning.
The chart organizes four primary markers into graduated ranges. Each has clinical significance for assessing metabolic health and guiding intervention.
Note on laboratory variation: Reference ranges vary by assay and laboratory. Always use your lab’s reference intervals for fasting insulin and glucose. These ranges represent typical clinical cut-offs but should be contextualized with the patient’s clinical presentation and symptoms.
The fasting insulin range printed on the downloadable template is illustrative, not a universal standard. Replace it with your ordering lab’s own reference interval before using the template with patients.
Several approaches exist to assess insulin resistance. The chart supports multiple testing strategies depending on clinical context and available resources.
Most practitioners use a combination: fasting insulin + fasting glucose to calculate HOMA-IR, plus HbA1c for long-term glucose control and client record documentation of metabolic trends.
Insulin resistance rarely appears in isolation. The chart includes supporting metabolic panel markers that refine risk stratification and guide clinical decision-making.
Triglycerides. Fasting triglycerides >150 mg/dL are a hallmark of insulin resistance and metabolic syndrome. Elevated triglycerides reflect impaired lipid metabolism secondary to compensatory hyperinsulinemia. Plot alongside HOMA-IR to confirm the metabolic picture.
HDL cholesterol. Insulin-resistant patients often have low HDL (<40 mg/dL in men, <50 mg/dL in women). The triglyceride-to-HDL ratio (normal <2) is a simple surrogate for insulin resistance severity. High triglycerides + low HDL = heightened cardiometabolic risk.
Blood pressure and waist circumference. Abdominal obesity and hypertension co-cluster with insulin resistance as features of metabolic syndrome. Document these anthropometric measures on the chart alongside lab values for a complete metabolic assessment.
Standard HOMA-IR cut-offs (developed in large European cohorts, predominantly male or mixed-gender) may not translate directly to female populations or PCOS. Clinicians must contextualize thresholds with patient phenotype and reproductive history.
PCOS and insulin resistance. Up to 70% of women with PCOS have insulin resistance, independent of BMI. The disorder amplifies compensatory hyperinsulinemia, driving androgen excess and anovulation. In PCOS cohorts, HOMA-IR thresholds as low as 1.5-2.0 (compared to population averages of 1.0-2.0) may trigger intervention.
A woman with PCOS, HOMA-IR 1.8, and regular ovulatory cycles may have different cardiometabolic risk than a non-PCOS woman with identical HOMA-IR and absent menstrual regularity.
Reproductive health context. Elevated androgen levels in PCOS exacerbate insulin resistance. Insulin resistance, in turn, worsens androgen synthesis. Use the chart as a screening tool, then refine interpretation with functional medicine assessment of cycle regularity, hirsutism, acne, and baseline androgen levels (free testosterone, androstenedione).
The chart’s value multiplies when embedded into your practice’s documented workflow. Print a copy for each metabolic health consultation, or complete it digitally as part of the patient’s measurements-tracking workflow to flag abnormal values automatically.
Use the chart during consultations to educate patients about their results, clarify the relationship between fasting insulin elevation and glucose dysregulation, and frame lifestyle interventions (dietary modification, resistance training, sleep optimization) as first-line treatment before or alongside medication.
Document the completed chart in your patient record for historical reference and longitudinal trend assessment.
Pabau's patient records, digital forms, and measurement tracking make it easy to document insulin resistance assessments, track lab trends, and link findings directly to clinical notes, so you can focus on patient outcomes, not paperwork.

This chart serves multiple healthcare settings where metabolic assessment is core to diagnosis and management.
Standardized reference ranges. A unified chart eliminates confusion from conflicting lab reports and non-standardized verbal reporting. Every consultation uses the same thresholds, improving consistency and patient trust.
Faster risk stratification. Within seconds, practitioners can place a patient into a risk category (normal, borderline, resistant, severely resistant) and frame the clinical message accordingly. No need to mental-math or consult external guidelines mid-consultation.
Enhanced patient education. Showing a patient their results on a clear visual chart makes the concept of insulin resistance concrete. Patients understand why an elevated HOMA-IR matters and why early intervention is worthwhile.
Documented clinical reasoning. Completed charts become part of the medical record, providing audit-trail evidence of systematic metabolic assessment. Useful for HIPAA compliance, insurance documentation, and continuity of care during referrals.
Filter your patient population by HOMA-IR score in your practice’s records. Identify all patients scoring 2.0 or higher (2.0-2.9 insulin resistant, 3.0 or higher severely resistant) and flag them for proactive lifestyle counseling. Early intervention before progression to prediabetes has the highest evidence-based success rate for insulin resistance reversal.
An insulin resistance levels chart centralizes the diagnostic thresholds clinicians need to assess metabolic health quickly and accurately during patient consultations. The chart transforms scattered lab values into a unified metabolic snapshot, enabling faster risk stratification and clearer patient education about the importance of early intervention.
Whether you manage metabolic health, oversee weight loss programs, or specialize in women’s reproductive health, this chart is a practical tool for every consultation. Download it, print it, and pair it with AI clinical documentation to standardize care and improve outcomes.
Book a demo to see how Pabau turns tools like this into a connected workflow across your whole practice.
Managing PCOS in your practice? Our PCOS hormone levels template gives you a ready-made framework to document androgen and reproductive hormone panels alongside insulin resistance markers.
Want a printable option for glucose tracking? Our blood sugar chart gives patients a simple take-home tool to log fasting and post-meal readings between visits.
Weighing lifestyle changes against medication? This clinical guide compares lifestyle and pharmacologic interventions for managing metabolic health.
Normal fasting insulin for adult women is typically 2-12 μIU/mL (lab ranges vary by assay). Levels above 12 μIU/mL suggest compensatory hyperinsulinemia. However, women with PCOS may have elevated insulin even within the conventional “normal” range. Clinical context (cycle regularity, androgen markers, BMI) matters more than the number alone.
A HOMA-IR of 2.5 indicates insulin resistance. The patient’s fasting insulin is elevated relative to their fasting glucose, signaling that cells are not responding normally to insulin. This warrants lifestyle intervention (dietary change, resistance training) and potential pharmacological screening. It is not a diabetes diagnosis but a warning sign of metabolic dysfunction.
PCOS does not directly cause insulin resistance, but the two disorders co-occur and amplify each other. Up to 70% of women with PCOS have insulin resistance. Insulin resistance, in turn, worsens androgen excess and anovulation. The bidirectional relationship makes metabolic assessment essential in PCOS evaluation and treatment planning.
Fasting glucose 100-125 mg/dL indicates prediabetes (ADA criteria), often accompanied by insulin resistance. However, insulin resistance can exist with normal fasting glucose if hyperinsulinemia is sufficient to compensate. Calculate HOMA-IR using both fasting insulin and glucose to confirm insulin resistance, since glucose alone is insufficient.
Evidence-based interventions include resistance training (builds insulin-sensitive muscle), a meal plan that cuts refined carbohydrates and increases fiber, sleep optimization (7-9 hours nightly), and weight loss if overweight (5-10% body weight reduction improves insulin sensitivity). Metformin may be considered if lifestyle alone is insufficient. Outcomes improve when multifactorial intervention is sustained over 3-6 months.