VO2 max testing: methods, norms, and clinical protocols
What is a VO2 max assessment and why does it matter? Most fitness metrics tell y...
Last Updated: July 30, 2026
ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) has no confirmatory diagnostic test, so diagnosis relies on matching symptom criteria and ruling out other conditions.
The IOM 2015 criteria center on post-exertional malaise (PEM) alongside disabling fatigue and unrefreshing sleep, so PEM assessment is essential to any evaluation.
A structured chronic fatigue syndrome test helps practitioners evaluate symptom duration, functional impact, and PEM severity in a consistent way.
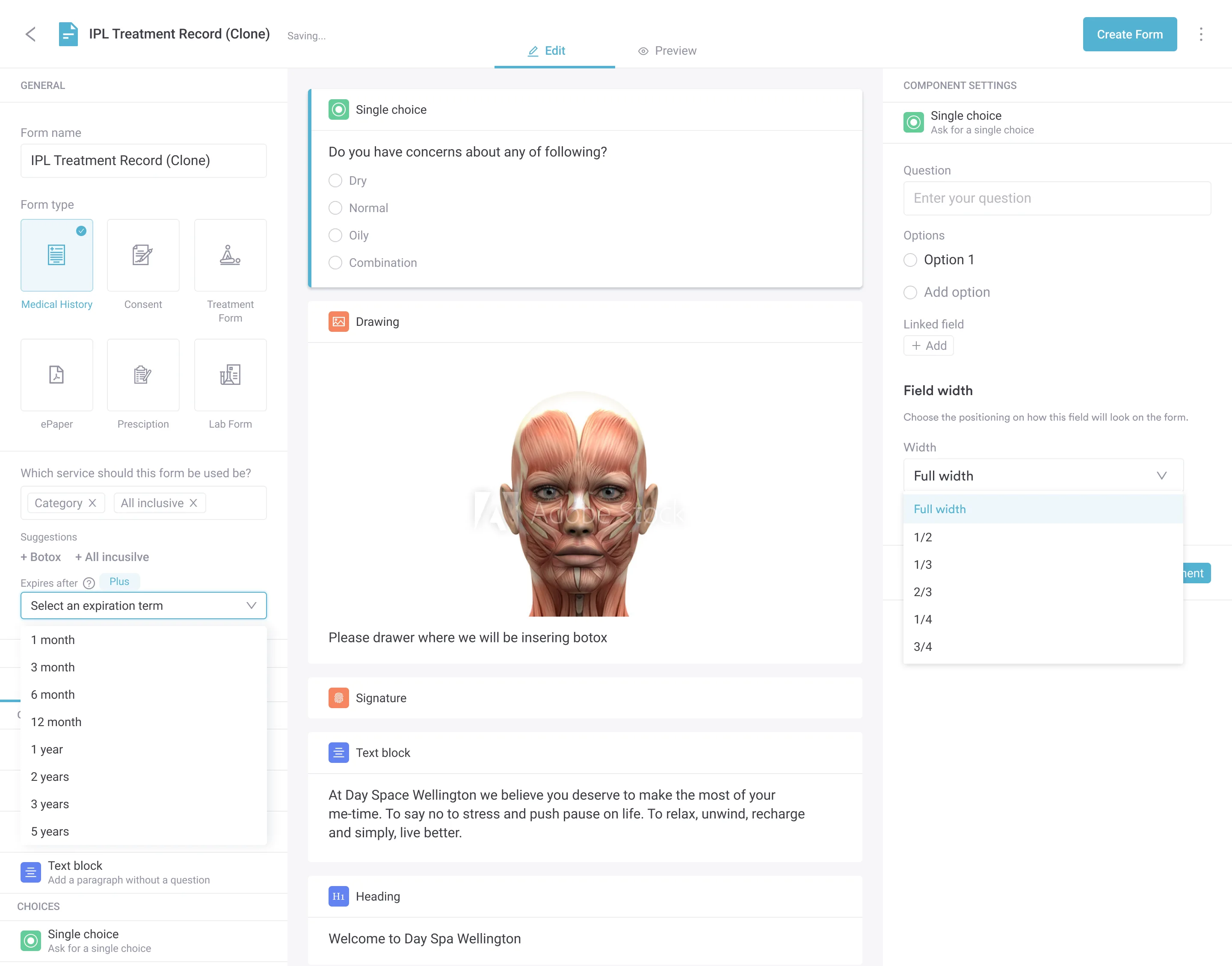
Practice management software like Pabau keeps the assessment, intake forms, and lab results in one patient record, with follow-up reminders that support continuity across visits.
A comprehensive diagnostic assessment tool designed for healthcare providers to evaluate patients presenting with suspected ME/CFS. Covers symptom criteria, post-exertional malaise screening, functional impact rating, and recommended laboratory panels for differential diagnosis.
Download templateThere is no single blood test that confirms chronic fatigue syndrome. Diagnosing ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) means matching a patient’s symptoms to established criteria and ruling out conditions that mimic it. A structured chronic fatigue syndrome test lets practitioners document those symptoms, score post-exertional malaise, and record the lab work that rules out other causes.
A chronic fatigue syndrome test is a structured assessment template that helps clinicians judge whether a patient meets the diagnostic criteria for myalgic encephalomyelitis (ME) or chronic fatigue syndrome (CFS).
It documents the four cardinal symptoms in the Institute of Medicine (IOM) 2015 criteria: persistent fatigue unrelieved by rest, post-exertional malaise (PEM), unrefreshing sleep, and cognitive impairment or orthostatic intolerance.
This assessment tool is not a confirmatory diagnostic test like a blood culture or imaging scan. Instead, it functions as a clinical checklist aligned with CDC and NICE diagnostic guidance, allowing practitioners to systematically record symptom patterns, duration, severity, and functional impact. Many practices integrate this assessment into their initial consultation workflow to ensure no diagnostic criteria are overlooked.
Here’s how to test for chronic fatigue syndrome, step by step. The workflow below mirrors a real patient evaluation:
A standardized chronic fatigue syndrome test keeps diagnosis consistent and lowers the risk of missing a criterion or a mimic condition. Many practitioners pair it with practice management software like Pabau, so findings, forms, and lab results sit in one patient record with automated follow-up reminders and a longitudinal diagnostic history.
A structured chronic fatigue syndrome test earns its place across specialties and practice settings:
GPs in the UK increasingly adopt structured tests to meet NICE NG206 diagnostic standards.
A structured assessment offers measurable operational and clinical advantages. It reduces diagnostic delays by ensuring clinicians evaluate all four IOM diagnostic criteria rather than anchoring on fatigue alone. This is particularly important because unrefreshing sleep and cognitive impairment are easy to overlook without systematic prompting.
The test creates a baseline clinical record that supports continuity of care across multiple practitioners. When patients move between a GP, a rheumatologist, and an integrative medicine specialist, a shared template reduces redundant questioning. Specialists can then track changes in functional status over time — a critical measure of disease trajectory and treatment response in ME/CFS.
Documentation clarity protects practices during audits and medicolegal review. A detailed, structured assessment demonstrates due diligence in differential diagnosis — ruling out thyroid disease, B12 deficiency, autoimmune conditions, and sleep disorders. It also shows alignment with established clinical guidelines. This is especially valuable in jurisdictions where ME/CFS is sometimes dismissed or misdiagnosed.
A chronic fatigue syndrome test also enables outcome tracking. By rating PEM severity and functional impact at baseline and at each follow-up, practitioners can see whether pacing and symptom-management strategies are helping or making the patient worse. That feedback matters in a condition where the same approach rarely suits every patient.
Pabau's digital forms and client records help you systematize ME/CFS evaluations, capture lab results, and track patient progress over time.

A critical component of any chronic fatigue syndrome test is systematic exclusion of conditions that mimic ME/CFS. Thyroid dysfunction (hypothyroidism), vitamin B12 or folate deficiency, iron deficiency anemia, and metabolic disorders like diabetes or adrenal insufficiency all present with severe fatigue and can coexist with ME/CFS.
Many practices build the differential into the assessment itself, prompting the practitioner to rule out:
The recommended lab panel for chronic fatigue evaluation includes CBC, comprehensive metabolic panel, ferritin, TSH, hemoglobin A1c, and inflammatory markers. Additional testing — ANA, EBV serology, cortisol, B12/folate, ferritin saturation — depends on clinical presentation. A normal basic lab panel does not rule out ME/CFS. It clarifies that symptoms are not secondary to a correctable metabolic or nutritional deficiency.
The Institute of Medicine (IOM) 2015 criteria, adopted by the CDC, require all of the following:
Two earlier frameworks, the Canadian Consensus Criteria and the International Consensus Criteria, put PEM at the center and give more granular guidance on symptom assessment. Many experienced ME/CFS clinicians reference all three to keep the evaluation comprehensive. A structured chronic fatigue syndrome test aligned with these standards helps practitioners navigate the overlap.
Key distinction: a chronic fatigue syndrome test is a screening and assessment tool, not a diagnostic instrument that “confirms” or “rules out” ME/CFS on its own. It supports clinical judgment by organizing information in a standardized format aligned with evidence-based criteria.
Persistent fatigue demands a methodical diagnostic approach. A structured chronic fatigue syndrome test integrated into your client records system ensures that every patient undergoes the same comprehensive evaluation, PEM is properly assessed, and differential diagnoses are systematically addressed. This standardization improves diagnostic accuracy, strengthens clinical documentation, and delivers better outcomes for patients living with ME/CFS.
Looking for ways to streamline patient intake? Digital forms and automated intake workflows eliminate paper shuffling and ensure no diagnostic questions are missed.
Need to track treatment response over time? Functional medicine practice management tools help you document baseline assessments and measure progress across follow-up visits.
Managing multiple locations or practitioners? Multi-location practice software ensures consistent ME/CFS evaluation standards across all your locations.
A chronic fatigue syndrome test is a structured diagnostic assessment template that helps clinicians evaluate whether a patient meets ME/CFS diagnostic criteria. It documents the four core IOM 2015 symptoms: persistent fatigue unrelieved by rest, post-exertional malaise, unrefreshing sleep, and cognitive or autonomic dysfunction.
No FDA-approved blood test currently confirms ME/CFS. Diagnosis relies on symptom criteria and ruling out mimicking conditions through structured assessment and recommended lab panels.
Common initial labs include a CBC, a metabolic panel, ferritin, TSH, HbA1c, and inflammatory markers such as CRP or ESR, in line with US ME/CFS Clinician Coalition guidance. Additional tests such as ANA, EBV serology, B12 or folate, and cortisol depend on the clinical picture.
The IOM criteria require fatigue lasting at least six months. Shorter-duration fatigue may reflect acute viral illness or treatment side effects rather than ME/CFS.
PEM is a disproportionate worsening of symptoms following physical or mental exertion, typically delayed by 24–48 hours. It is required for ME/CFS diagnosis and is the feature most clearly distinguishing it from other fatigue conditions.
Depression and anxiety can coexist with ME/CFS but do not cause it. Symptom timeline and pattern help clinicians distinguish primary psychiatric illness from comorbid mood disorders in an ME/CFS patient.
Online chronic fatigue syndrome tests and quizzes can flag symptoms worth reviewing, but they cannot diagnose ME/CFS. A diagnosis needs a clinician to confirm the symptom criteria and rule out other conditions through examination and lab work.
The core symptoms are disabling fatigue lasting at least six months, post-exertional malaise, unrefreshing sleep, and either cognitive impairment or orthostatic intolerance. Muscle and joint pain, headaches, and a sore throat often accompany them.