ICD-10 Code M45.6: Ankylosing spondylitis lumbar region
ICD-10 Code M45.6 is the billable ICD-10-CM diagnosis code for ankylosing spondy...
Last Updated: August 3, 2026
The anterior drawer test assesses anterior cruciate ligament (ACL) laxity by measuring tibial displacement when the knee is flexed 80-90°
Sensitivity ranges 18-92% and specificity 78-98% depending on acute vs chronic ACL status; comparative testing (Lachman, pivot shift) improves diagnostic accuracy
Tibial displacement is graded using standardized scales (0 to 3+) to document laxity severity and guide treatment decisions
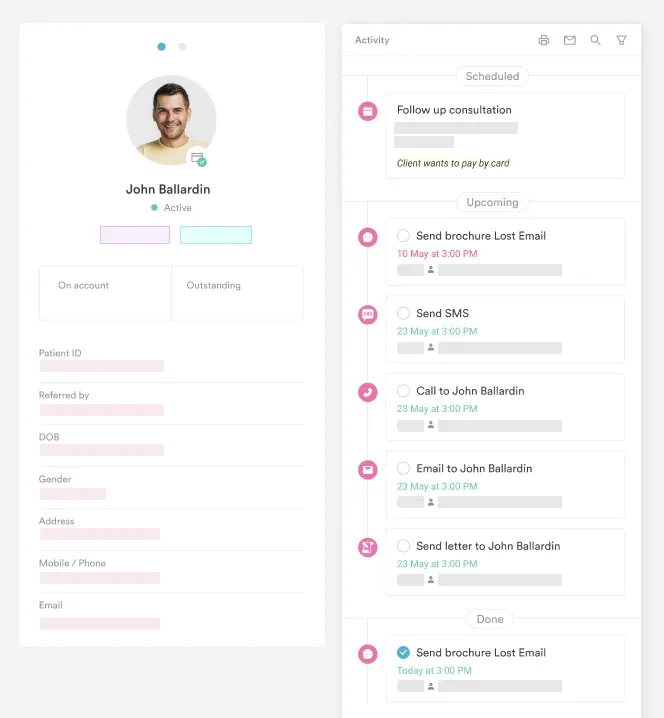
Practice management software like Pabau digitizes these forms and patient records to streamline documentation and keep multi-variant recording consistent across knee, ankle, and shoulder
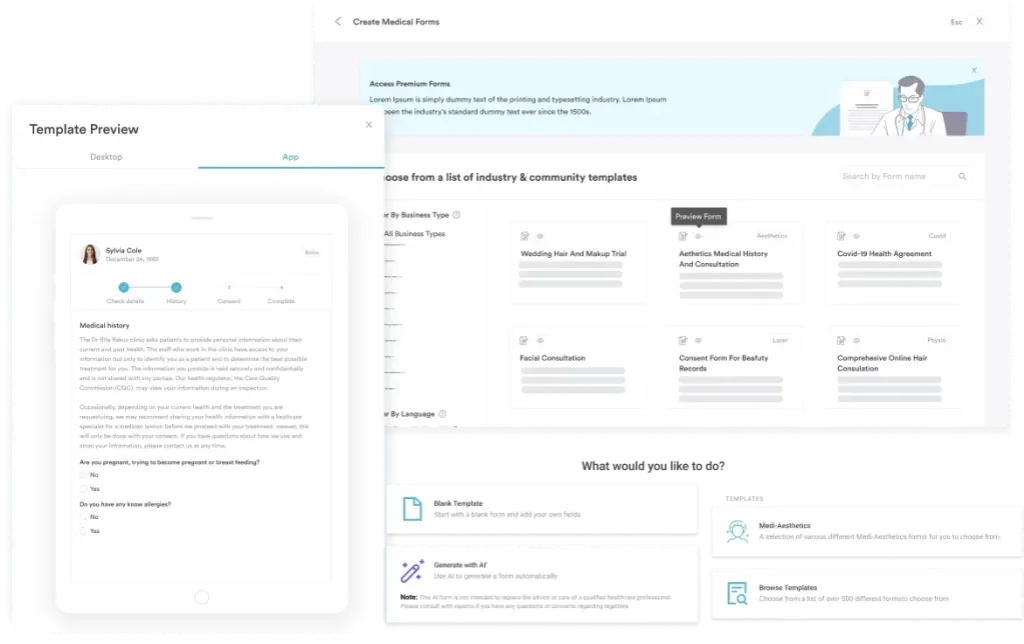
A ready-to-use assessment form covering patient positioning, stabilization technique, positive/negative finding criteria, tibial displacement grading scales, and multi-joint variant recording (knee, ankle, shoulder).
Download templateUse the free anterior drawer test template below to standardize how your practice records ACL, ankle, and shoulder laxity findings. Download it as a printable PDF, then adapt the fields to your practice and rebuild it as a digital form inside your patient records.
The anterior drawer test, also known as the anterior drawer sign, is a fundamental clinical assessment used to evaluate knee and ankle ligament integrity. In the knee, it measures anterior cruciate ligament (ACL) laxity by assessing how far the tibia (shin bone) slides forward relative to the femur (thighbone) when a posterior-to-anterior force is applied.
Standardized documentation of these tests supports physical therapy practice management, and this template gives you a structured way to record findings consistently across sessions.
The test is performed with the patient supine and the knee flexed to 80-90°. The clinician stabilizes the patient’s foot and applies a gentle anteriorly-directed force to the tibia, observing and grading the degree of tibial displacement.
Unlike the Lachman test (performed at 20-30° flexion), the anterior drawer test is sensitive to both acute and chronic ACL injuries, though sensitivity varies widely across patient populations and injury chronicity.
Beyond the knee, the anterior drawer test is also adapted for the ankle (assessing the anterior talofibular ligament after inversion trauma) and occasionally the shoulder (evaluating glenohumeral translation). A comprehensive assessment template captures all variants in one structured format, enabling multi-joint evaluation in a single patient record.
Correct technique is essential for reliable findings. Begin by positioning the patient supine on the examination table with the knee flexed to 80-90° and the foot flat on the table. This relaxed position allows passive tibial translation without muscle guarding.
The test should be repeated with the foot in neutral, external rotation, and internal rotation to assess different ligament contributions. Clinical documentation best practices recommend recording the patient’s position, foot position, force applied (qualitative: gentle, moderate, firm), and observed displacement in the assessment form to ensure reproducibility across sessions.
A positive anterior drawer test indicates ACL laxity or rupture. However, sensitivity varies considerably. Research shows sensitivity ranges from 18-92% depending on whether the injury is acute or chronic: acute ACL tears often show lower sensitivity (around 22%) because muscle guarding limits tibial translation, while chronic ACL deficiency shows higher sensitivity (92%) as muscular support is diminished over time.
A positive anterior drawer test typically produces a soft or mushy endpoint as the tibia translates forward, in contrast to the firm endpoint felt when the ACL is intact.
Specificity is consistently high (78-98%), so a positive test is highly predictive of ACL pathology. A negative test does not rule out ACL injury, though. Many acute tears are missed by the anterior drawer test alone.
The Lachman test (sensitivity ~84%) or pivot shift test (sensitivity ~60%) often provides better diagnostic accuracy and should be performed alongside the anterior drawer test for comprehensive assessment.
A negative anterior drawer test suggests ACL integrity, but clinicians should interpret this cautiously in acute injury settings. SOAP note format documentation should always note the clinical context (acute vs chronic presentation, pain level, muscle guarding) alongside test findings to support clinical reasoning.
Standardizing the grade of tibial displacement enables consistent communication between clinicians and supports treatment decision-making. The most widely used scale is the Lachman-test-derived 0 to 3+ grading system, adapted here for the anterior drawer test:
Grading should be recorded alongside patient factors that influence displacement: acute injuries often show less laxity due to muscle guarding and pain, while chronic ACL-deficient knees demonstrate greater translation. This contextual information aids clinical interpretation and supports the decision to pursue advanced imaging (MRI) or specialist referral.
The anterior drawer test principle extends beyond the knee to the ankle and shoulder, allowing clinicians to assess ligament integrity across multiple joints using a consistent assessment approach.
The ankle anterior drawer test assesses passive stability of the lateral ankle joint, particularly the anterior talofibular ligament (ATFL), after inversion trauma or ankle sprain. The patient lies supine with the knee extended. The examiner stabilizes the distal tibia and applies an anteriorly-directed force to the foot, observing how far the talus translates forward in the ankle mortise.
A positive test (increased anterior translation) suggests ATFL injury. Ankle injury assessment protocols often complement anterior drawer findings with other ligament tests, including the inversion stress test and the talar tilt test, for comprehensive ankle evaluation.
Less commonly performed than knee or ankle variants, the shoulder anterior drawer test evaluates glenohumeral translation. The examiner stabilizes the scapula and applies an anteriorly-directed force to the humeral head, assessing the degree of humeral head subluxation.
Sensitivity and specificity data for the shoulder variant are limited compared to knee and ankle applications, and this test is typically combined with other stability tests (apprehension, relocation) for shoulder instability assessment.
A unified anterior drawer test template that captures all three variants (knee, ankle, and shoulder) lets physical therapists and orthopedic clinicians assess multi-joint stability within a single patient record, so grading stays consistent and documentation time drops across assessments.
Structured documentation of anterior drawer test findings supports clinical communication, audit trails, and medicolegal protection. Structured patient records should capture:
A recommended template structure follows the SOAP note framework: Subjective (symptom history, injury context), Objective (test position, displacement findings, grade), Assessment (ACL status, differential diagnoses), Plan (imaging referral, treatment pathway, follow-up timeline).
Digital assessment forms reduce transcription errors and enable real-time data capture during the examination. AI-assisted documentation tools can auto-populate standard text fields based on observed findings, accelerating note completion while maintaining clinical accuracy and reducing clinician workload after patient sessions.
The anterior drawer test is rarely interpreted on its own. Knee injuries often involve multiple ligamentous and capsular structures, so a thorough assessment integrates findings from complementary tests.
The return-to-sport protocol frameworks used in sports medicine practices typically require a battery of tests (anterior drawer, Lachman, pivot shift, posterior drawer, varus/valgus stress) before clearance for activity, underscoring the anterior drawer test’s role within a broader evaluation strategy.
Anterior drawer test results must be contextualized within the clinical history. Acute knee injuries (first 48-72 hours) often show reduced tibial displacement because muscle guarding and pain limit translation, leading to false negatives. Chronic ACL deficiency (months to years post-injury) produces greater laxity as muscular stabilizers fatigue.
MRI remains the gold standard for ACL imaging and should be considered when clinical suspicion is high and anterior drawer test results are ambiguous.
Because ACL injuries frequently occur alongside medial meniscus tears and capsular damage, a positive anterior drawer test should prompt assessment of meniscal integrity and any patient-reported instability, such as the knee giving way during activity.
Practice management workflows that integrate structured assessment documentation with imaging referral tracking help ensure appropriate next-step decision-making and improve patient outcomes through evidence-based pathways.
Record anterior drawer test findings, grading scales, and multi-joint variants in a structured digital format, reducing transcription time and improving clinical consistency.

Anterior drawer test sensitivity and specificity vary significantly across the published literature. Meta-analyses and systematic reviews report sensitivity of 0.18-0.92 and specificity of 0.78-0.98 for ACL detection, depending on injury acuity, patient population, and examiner experience.
In acute ACL tears, sensitivity is lower (around 22%) because acute muscle guarding and pain limit tibial translation, so a negative result cannot be relied on to rule out an ACL injury in the acute setting.
In chronic ACL deficiency, sensitivity improves to approximately 92% with specificity around 91%, meaning the test becomes more reliable weeks to months after the initial injury when muscle guarding has diminished. This temporal variation underscores why serial testing (acute, subacute, chronic phases) may be more informative than a single assessment.
Comparative testing enhances diagnostic confidence. The Lachman test demonstrates higher mean sensitivity (~84%) than the anterior drawer test (~22%) for acute ACL tears. Pivot shift tests have sensitivity around 60% but near-perfect specificity (98%), making them highly predictive when positive.
Clinicians should use multiple tests in combination rather than relying on any single test result. When manual findings are equivocal, instrumented laxity measurement (arthrometry, such as the KT-1000) and examination under anesthesia can further quantify anterior tibial translation.
A 2022 systematic review and meta-analysis found the diagnostic accuracy of the anterior drawer, Lachman, and pivot shift tests to be broadly comparable, and confirms the anterior drawer test as a standard component of evidence-based knee ligament assessment.
Both tests assess ACL integrity but differ in positioning, sensitivity, and clinical application. The Lachman test is performed with the knee flexed 20-30°, a position that reduces hamstring tension and isolates the ACL. The anterior drawer test uses 80-90° knee flexion, a more relaxed position that allows hamstring co-contraction but may provide additional stability.
Lachman test advantages:
Anterior drawer test advantages:
Clinical best practice combines both tests. Use the Lachman test first in acute presentations (higher sensitivity) and the anterior drawer test as a supplementary measure, especially in chronic cases. The pivot shift test, when positive, provides the highest specificity and should be included if clinical suspicion remains high.
Pabau, practice management software built for healthcare practices, helps physical therapy and sports medicine teams standardize orthopedic assessment documentation. Digital forms tied to patient records capture anterior drawer test findings with the 0 to 3+ grading scale built in, so data collection stays consistent across every practitioner in a multi-location practice. The same forms library extends to other downloadable templates, such as a 12-panel drug test report and a body neutrality worksheet, giving every department one documentation workflow.
Findings feed straight into automated workflows. Record a 2+ or 3+ grade, and Pabau can trigger a task to book MRI imaging or a specialist referral, so nothing stalls after the exam. Pabau Scribe, our AI scribe, can also draft the assessment note from your structured findings, cutting the time you spend writing up after each session.
Need to standardize your ACL assessment workflow? Physical therapy EMR software keeps positioning notes, grading scales, and referral flags together in one patient record.
Looking for a template to document examination findings? Sports medicine software helps orthopedic teams standardize test results and track return-to-play decisions across every practitioner.
Want to reduce post-session documentation time? AI-assisted documentation auto-generates clinical notes from structured assessment findings, freeing clinicians to focus on patient care.
The anterior drawer test remains a foundational orthopedic assessment tool for evaluating ACL integrity and ligament laxity across the knee, ankle, and shoulder. While sensitivity varies by injury acuity (18-92% for knee ACL injuries), knowing the test’s strengths, particularly for chronic ACL assessment, and its limitations supports clinically sound decisions.
Pairing the anterior drawer test with the Lachman test and pivot shift test strengthens diagnostic confidence, and standardized documentation keeps that consistency across every practitioner and location. To see how structured digital templates fit into your practice’s workflow, book a demo with Pabau.
A positive anterior drawer test indicates ACL laxity or rupture. However, sensitivity varies (18-92% depending on acute vs chronic injury), so a positive test should be confirmed with the Lachman test, pivot shift test, or MRI imaging before confirming ACL pathology.
Tibial displacement is graded on a 0 to 3+ scale: 0 = no movement (intact ACL); 1+ = slight (0-5 mm, mild laxity); 2+ = moderate (6-10 mm, significant damage); 3+ = gross movement (>10 mm, complete rupture). Grading guides treatment decisions and specialist referral urgency.
The anterior drawer test has lower sensitivity in acute injuries (around 22%) because muscle guarding and pain limit tibial translation. The Lachman test is more sensitive for acute ACL tears. The anterior drawer test becomes more reliable in chronic ACL deficiency (sensitivity 92%).
Yes. The ankle anterior drawer test assesses the anterior talofibular ligament (ATFL) after ankle sprain. The shoulder variant evaluates glenohumeral translation but has limited published sensitivity/specificity data. Both variants use the same principles: patient positioning, stabilization, and anterior force application.
Yes. Use the Lachman test first in acute injuries (higher sensitivity ~84%), then the anterior drawer test as a supplementary measure. The pivot shift test adds high specificity if clinical suspicion remains. Combining multiple tests improves diagnostic accuracy over any single test alone.
Position the patient supine with the knee flexed to 80-90° and the foot flat on the table or held by the examiner. This relaxed position prevents muscle guarding. Always stabilize the foot to eliminate foot movement as a confounding variable.