Immunization record form: Free template and what to include
A free immunization record form template, plus the fields schools and employers ...
Last Updated: August 11, 2026
An admission nursing note is the foundational clinical document that captures a patient’s initial assessment, medical history, and baseline health status upon admission to a healthcare facility.
Complete admission notes must include patient identification, medical and medication history, allergies, vital signs, physical examination findings, and a comprehensive nursing assessment with identified care needs.
Documentation accuracy serves as a legal record and establishes the baseline for ongoing treatment planning, quality of care evaluation, and compliance with regulatory standards set by CMS, The Joint Commission, and state nursing boards.
Pabau’s digital forms and automated workflows eliminate manual paperwork, reduce documentation errors, and ensure compliance with HIPAA requirements while enabling secure storage and rapid access to admission notes across multiple care settings.
A comprehensive admission nursing note template covering patient identification, medical history, allergies, vital signs, physical examination findings, nursing assessment, and care planning documentation for initial patient intake across hospital, nursing home, and clinical settings.
Download templateAn admission nursing note is a standardized clinical document that captures a patient’s initial assessment and baseline health status during patient intake at a hospital, nursing home, skilled nursing facility, psychiatric unit, or outpatient clinic. The note establishes a comprehensive record of the patient’s presenting condition, medical history, current medications, allergies, and identified care needs.
This foundational assessment serves multiple critical functions: It documents the patient’s condition at the point of entry into the healthcare facility, creates a legal medical record, establishes baseline data for measuring patient progress, informs the development of the care plan, and supports continuity of care across shifts and departments. The Joint Commission and CMS require that admission assessments be completed within specific timeframes and contain standardized elements to ensure quality care and regulatory compliance.
Unlike progress notes (which document changes in the patient’s condition over time) or physician admission histories (which focus on differential diagnosis and medical decision-making), the admission nursing note prioritizes functional assessment, nursing diagnoses, and the specific interventions needed to support patient safety, comfort, and recovery during the initial care period.
According to the American Nurses Association and CMS documentation standards, every admission nursing note must contain specific core elements. Each section provides essential clinical context required for safe, compliant care:
Writing an effective admission note requires systematic data collection and clear documentation. Follow these five operational steps that mirror actual workflow processes in clinical settings:
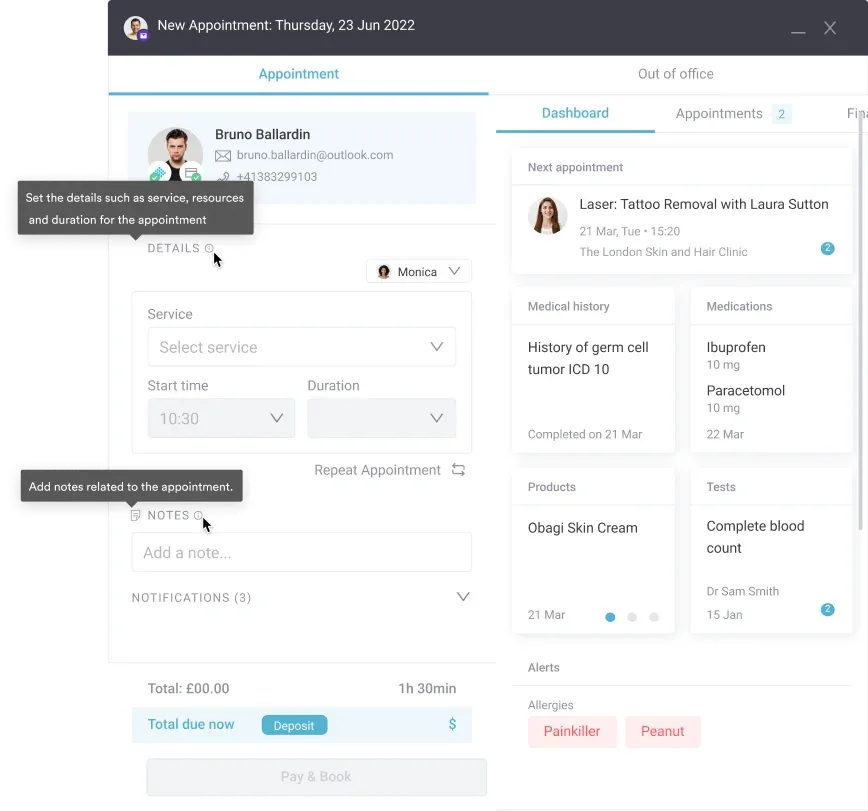
Practice management software like Pabau uses automated workflows to make sure no essential components are missed and to cut the time spent charting after patient contact, so nurses can move on to the next patient instead of catching up on notes at the end of a shift.
An admission nursing note is completed by the registered nurse (RN) or licensed practical nurse (LPN) who first receives the patient. In hospital settings, this is typically an ED nurse (for ED admissions) or a unit nurse (for direct admissions). In skilled nursing facilities and nursing homes, the admitting nurse completes the admission assessment within the first few hours of the resident’s arrival.
Facilities must ensure the admitting nurse has completed relevant training on assessment protocols and documentation standards. The nursing assessment complements (but does not replace) the physician admission history and physical examination. Team management software improves team communication, and clear role assignment prevents duplicate work while making sure every part of the patient evaluation gets covered.
The admission nursing note serves critical functions beyond documentation. It establishes a legal baseline record of the patient’s condition at the time of entry into care—this becomes essential if questions arise about the quality of care provided or the appropriateness of clinical decisions made during hospitalization.
Regulatory agencies including The Joint Commission and CMS require that admission assessments be completed timely (typically within 24 hours of admission) and contain standardized elements. Incomplete or missing admission notes constitute a documentation deficiency during accreditation surveys. Accurate, thorough admission notes also support safer patient care by communicating essential information to all team members involved in treatment planning.
The same core elements look different depending on where a patient is admitted. These admission notes examples show how a hospital, nursing home, and psychiatric unit each document the initial assessment. The first uses a SOAP structure you can copy directly into your charting.
A 68-year-old male admitted via emergency department, documented in SOAP format:
An 82-year-old female admitted from home with her daughter present as interpreter. Alert and oriented ×2 (oriented to person and place, confused about date). Current medications include lisinopril for hypertension and metformin for type 2 diabetes. Known allergies: penicillin (rash). Vital signs stable. Physical exam shows dry skin on bilateral lower extremities, diminished lower-extremity strength, and walker use for mobility. The nursing assessment identifies fall risk (age, mobility limitations, orientation change) and skin integrity risk. Care plan: fall precautions, twice-daily skin assessment, and physical therapy consultation.
A 34-year-old male admitted via emergency department after presenting to his family physician with suicidal ideation and hopelessness. Alert and oriented ×3, denies current intent to harm self but reports a passive death wish. Psychiatric history includes depression managed with sertraline, with baseline mood reportedly stable on the current regimen. Patient states medication compliance is inconsistent. Physical exam unremarkable. The nursing assessment identifies risk for self-harm and the need for suicide precautions, medication reconciliation, and psychiatric nursing evaluation. Initial interventions: 1:1 observation, frequent nursing assessment, and psychiatry consultation within 24 hours.
Reduce paperwork and charting time while ensuring regulatory compliance and patient safety. See how Pabau simplifies nursing documentation across your facility.

The Centers for Medicare & Medicaid Services (CMS) requires that hospitals and skilled nursing facilities complete an admission assessment within specific timeframes (typically 24 hours of admission) and document standardized elements. HIPAA regulations mandate secure storage of all patient documentation, including admission notes, with restricted access limited to those with a legitimate care need.
The American Nurses Association (ANA) standards for nursing documentation and state nursing practice acts require that nurses document assessments accurately, completely, and in a timely manner. Documentation that is incomplete, illegible, or missing required elements can be used as evidence of substandard care if patient outcomes are questioned. Conversely, thorough, specific documentation demonstrates appropriate clinical assessment and informed decision-making.
The admission nursing note is the clinical foundation for safe, compliant, patient-centered care. A thorough, accurate, and timely admission assessment ensures continuity of care, establishes baseline documentation, supports informed clinical decision-making, and demonstrates accountability to regulatory agencies and legal review.
Using standardized templates and digital documentation tools reduces time spent charting, minimizes errors, and helps ensure no essential assessment components are missed. Whether you’re an individual practitioner, a small clinic, or a multi-location facility, investing in structured admission documentation processes and compliant record-keeping systems protects your patients, your staff, and your organization’s reputation and licensure.
Need to streamline patient intake across multiple departments? Digital forms and automated patient intake eliminate paper while ensuring compliance with documentation standards.
Looking to improve care coordination between shifts and departments? Centralized patient records give your entire team instant access to current assessment data and care plans.
Want to reduce administrative burden and focus on patient care? Mental health and clinical EHR software handles documentation workflows so nursing staff spend less time charting and more time with patients.
The admission nursing note documents the nurse’s assessment of the patient’s functional status, nursing diagnoses, and nursing-focused interventions. The admission history and physical (completed by the physician) focuses on medical history, differential diagnosis, and physician-ordered treatment. Both are required for comprehensive admission documentation, but they serve different purposes and are completed by different providers.
The length varies based on the complexity of the patient’s condition and the facility’s specific requirements. A straightforward admission note for a stable patient might be 2-3 pages; a complex admission for a patient with multiple comorbidities and psychosocial issues might be 5-7 pages. Aim for completeness and clarity rather than a specific word count. Include all essential elements without unnecessary repetition or padding.
Late or missing admission notes constitute a documentation deficiency under The Joint Commission and CMS standards. This can result in regulatory findings during accreditation surveys, potential loss of accreditation, loss of Medicare/Medicaid reimbursement, or state licensing sanctions. Beyond regulatory risk, missing or incomplete admission documentation compromises continuity of care and patient safety.
Yes. The admission nursing note concludes with an initial care plan that identifies prioritized nursing diagnoses, specific interventions, frequency of monitoring, patient/family education needs, and expected outcomes. The care plan may be developed as part of the admission note or as a separate but linked document, depending on facility policy.
The admission nursing note is a confidential medical record. Access is restricted to healthcare team members who have a documented need to know for the purpose of providing patient care, conducting quality reviews, or meeting legal/regulatory requirements. Patients have the right to request copies of their medical records, including admission notes, under applicable privacy laws (HIPAA in the US, GDPR in the EU).
An admission note includes patient identification, source of admission, chief complaint, medical and medication history, allergies, vital signs, a head-to-toe physical examination, functional and psychosocial status, nursing diagnoses, and an initial care plan. Together these give every clinician who opens the record a complete baseline of the patient’s condition at intake.
You can download a free, ready-to-use version at the top of this page. It covers patient identification, medical history, allergies, vital signs, physical examination, nursing assessment, and care planning, so you can standardize documentation across hospital, nursing home, and clinical settings.