Crisis communication plan
Download your free crisis communication plan A comprehensive template covering c...
Last Updated: July 28, 2026
Administrative requirements for surgery are mandatory regulatory standards that practices and ambulatory surgery centers must follow before, during, and after operative procedures.
Pre-operative documentation must include informed consent, insurance verification, patient intake forms, and prior authorization to prevent billing denials and regulatory violations.
Operating room registers, operative reports, and post-operative care documentation are required under CMS rules — 42 CFR §482.51 for hospitals, and the separate CMS Conditions for Coverage at 42 CFR Part 416 for freestanding ambulatory surgery centers — plus state licensure boards.
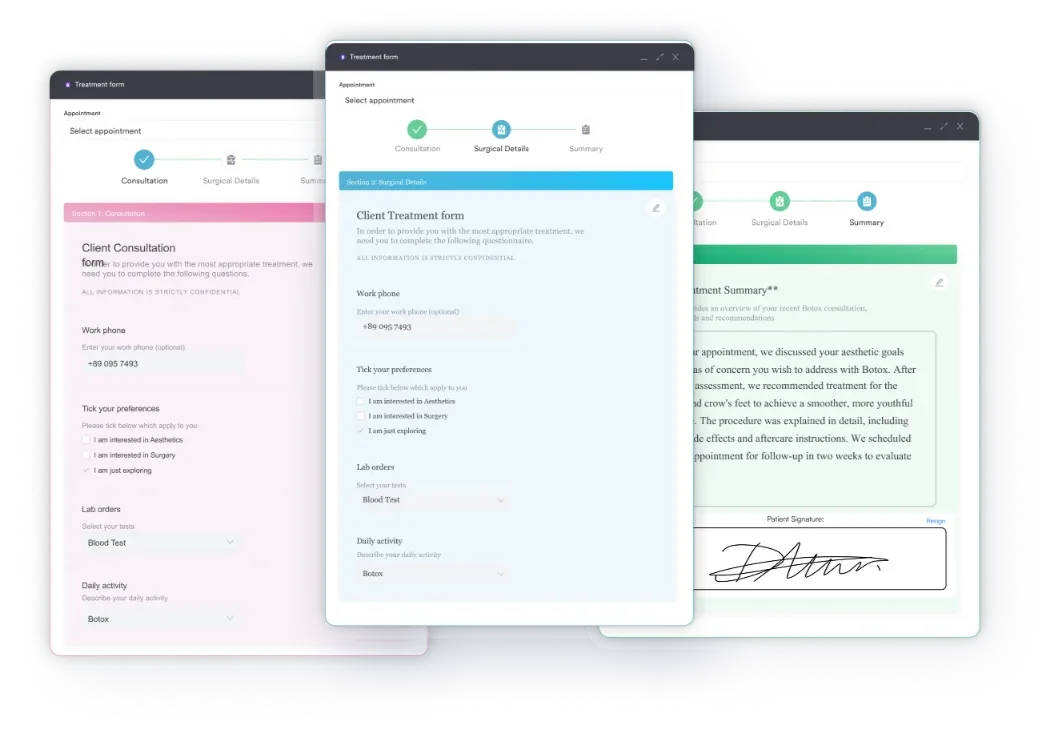
Practice management software like Pabau offers digital forms and automated workflows that streamline compliance documentation, reduce administrative burden, and ensure all required records are complete before surgery.
A comprehensive template covering patient intake, informed consent, pre-operative assessment, insurance verification, prior authorization, operative documentation, and post-operative care requirements for surgical practices and ambulatory surgery centers.
Download templateSurgical practices operate under strict regulatory oversight. The administrative requirements for surgery span every stage of patient care — from the initial consultation through discharge documentation. Missing a step can trigger compliance violations, billing delays, and patient safety risks.
This guide covers the administrative workflows, documentation standards, and regulatory obligations that keep surgical practices compliant and efficient.
The administrative requirements for surgery refer to the formal documentation, regulatory compliance standards, and workflow processes that healthcare facilities must maintain before, during, and after surgical procedures.
These requirements exist across multiple regulatory tiers: federal rules (CMS Conditions of Participation for hospitals and CMS Conditions for Coverage for ambulatory surgery centers), state licensure boards, accreditation bodies, and facility-specific policies.
Hospitals must comply with 42 CFR §482.51, the CMS Condition of Participation for Surgical Services, which requires documented preoperative assessments, informed consent, operative reports, and post-operative care plans.
Freestanding ambulatory surgery centers (ASCs) are governed by a separate framework, the CMS Conditions for Coverage at 42 CFR Part 416. It covers the same core documentation areas under different section numbers. State boards and accreditation bodies (The Joint Commission, AAAHC, AAAASF) add credentialing, facility design, and quality assurance standards on top of whichever federal framework applies.
These requirements serve two purposes. They protect patient safety by keeping clinical decisions consistent and care continuous, and they keep billing accurate and audit-ready by documenting every administrative touchpoint.
Implementing an administrative requirements for surgery checklist across your practice requires five core operational steps. Each step maps to specific form sections, staff responsibilities, and regulatory touchpoints.
Use digital intake forms to automate steps 1-3, reducing manual data entry and ensuring no required fields are left blank. Automated workflows can trigger pre-authorization reminders and prompt clinicians to complete documentation before discharge.
Anesthesia documentation also feeds directly into billing. The complexity and duration recorded in the anesthesia plan determine which code applies — compare how CPT code 00950 covers vaginal endoscopy anesthesia against CPT code 01234 for anesthesia during radical femur resection to see how much that varies by procedure.
Pro tip: Assign a dedicated staff member to verify checklist completion 24 hours after each surgical procedure. This catches missing or incomplete documentation while details are still fresh and allows rapid correction before billing submission.
Managing administrative requirements for surgery manually creates bottlenecks and compliance risk. Practice management software like Pabau automates pre-registration, consent management, and post-operative documentation so your team stays compliant without the paperwork. See how surgical practices reduce administrative overhead with Pabau.
This template is essential for any healthcare facility performing surgical procedures. It applies across multiple practice types and regulatory contexts.
Practice managers, surgical coordinators, compliance officers, and practice administrators use this template to design their administrative infrastructure. Surgical practice management software can centralize these workflows across multiple teams and locations.
Structured administrative documentation delivers measurable operational and financial returns. Practices implementing comprehensive administrative requirements for surgery frameworks report faster billing cycles, fewer claim denials, and cleaner regulatory audits.
Compliance and audit readiness: A complete administrative record demonstrates to regulators (CMS, state boards, accreditation bodies) that your facility meets legal standards. Audits run faster when documentation is organized and accessible. A broader HIPAA compliance checklist or medical spa compliance checklist can help confirm nothing outside surgical documentation gets overlooked.
Reduced billing delays and denials: Missing pre-authorization, incomplete insurance verification, or absent informed consent often trigger claim rejections. A significant share of denied surgical claims trace back to these kinds of administrative errors. A checklist ensures every required field is completed before the patient leaves the facility.
Improved patient safety: Documented preoperative assessments catch contraindications and drug interactions. Operative reports with detailed findings support accurate billing code selection and create a clear clinical record for post-operative follow-up.
Faster staff onboarding: New administrative staff learn the required workflow steps immediately rather than discovering missing steps through trial and error. Compliance management workflows can standardize processes across teams, meaningfully reducing training time.
The moment a patient books a surgical procedure, trigger an automated checklist: insurance card scan due, pre-authorization deadline, consent form signing appointment, and pre-operative testing dates. Front desk staff follow a single list instead of juggling multiple spreadsheets. This markedly reduces missed steps and eliminates last-minute documentation scrambles.
Surgical administrative requirements follow three distinct phases, each with specific documentation standards and regulatory obligations.
Pre-operative requirements begin at scheduling and extend through the 24 hours before surgery. Medical forms at your healthcare practice form the backbone of this phase. Key documents include:
CMS requires that all preoperative assessments be completed and documented in the patient record before surgery begins. Missing or incomplete documents can delay the surgical schedule and trigger compliance findings during audits.
During surgery, the operating room nurse maintains the operating room register — a real-time log of every procedure performed, personnel present, start/end times, and equipment used. This document is legally required under 42 CFR §482.51 for hospitals, and under the parallel CMS Conditions for Coverage at 42 CFR Part 416 for freestanding ASCs. It must be complete and up to date.
Immediately after surgery, the surgeon dictates or writes the operative report. The report must describe the procedure performed, techniques used, findings (including tissues removed or altered), estimated blood loss, complications encountered, and recommendations for post-operative care.
The operative report is the clinical foundation for accurate billing code assignment and is the primary document reviewed during medical coding audits.
Post-operative requirements include:
All post-operative documentation must be completed before the patient is discharged and filed in the medical record within 24 hours. Hospital-based discharges also follow time-based billing codes, such as CPT code 99239 for hospital discharge day management over 30 minutes.
Administrative requirements for surgery operate under multiple overlapping regulatory frameworks. Understanding each one ensures your documentation strategy covers all bases.
Practices must identify which regulatory tiers apply to their specific setting (hospital, ASC, office-based, specialty practice) and build documentation checklists accordingly. A multi-location surgical network may face different state requirements per location, necessitating location-specific protocols with a standardized core template.
The administrative requirements for surgery span preoperative verification and consent, intra-operative documentation, and post-operative care planning. Compliance is non-negotiable: it protects patient safety, enables accurate billing, and demonstrates regulatory readiness during audits.
A comprehensive administrative checklist — supported by digital forms, automated workflows, and practice management systems — transforms these requirements from a source of stress into a streamlined operational backbone. Download the template above and adapt it to your facility’s specific regulatory context, patient volume, and surgical specialties.
Need a structured clinical documentation system? Patient records and clinical documentation centralizes all administrative and clinical notes in one searchable record.
Looking to automate appointment reminders and pre-registration? Appointment scheduling and pre-registration systems reduce manual follow-up and ensure no patient is overlooked.
Concerned about compliance visibility across multiple teams? Surgical practice business planning guides include compliance infrastructure as a foundational component.
State regulations and federal law require documented preoperative assessment, informed consent, an operative report describing techniques and findings, an operating room register, and a post-operative care plan. Hospitals must comply with 42 CFR §482.51, while freestanding ambulatory surgery centers are governed by the separate CMS Conditions for Coverage at 42 CFR Part 416. Every surgical facility must maintain these documents in the patient’s medical record.
The operative report must describe the surgical procedure performed, techniques used, findings (tissues removed or altered), estimated blood loss, any intra-operative complications, and recommendations for post-operative management. It must be written or dictated immediately following surgery and signed by the surgeon.
Insurance verification and pre-authorization typically happen 3-5 days before surgery. The practice submits the procedure code and patient demographics to the insurance payer, receives an authorization number and confirmation of coverage, and documents this in the patient’s administrative record to prevent billing denials.
Informed consent must be documented in writing, include the specific procedure name and risks, confirm patient understanding of alternatives, and be signed by the patient (or legally authorized representative) and a witness. The signed form remains in the patient’s medical record.
ASCs must maintain preoperative assessments, informed consent, operative reports, operating room registers, credentialing files for all providers, facility licensure certificates, accreditation documentation, and quality assurance records. Records are subject to state health department audits and accreditation body reviews.