Initial consultation note: Free sexology form template
Download your free sexology initial consultation note A one-page clinical note f...
Last Updated: August 6, 2026
17-hydroxyprogesterone (17-OHP) is a hormone precursor in the adrenal cortex; elevated levels indicate 21-hydroxylase deficiency and congenital adrenal hyperplasia (CAH).
Specimen is serum collected during follicular phase in females; CPT code 83498 applies; methodology is LC/MS or HPLC-MS/MS.
Reference ranges vary by age, sex, and menstrual phase: follicular females 15-70 ng/dL, luteal 35-290 ng/dL, males 27-199 ng/dL.
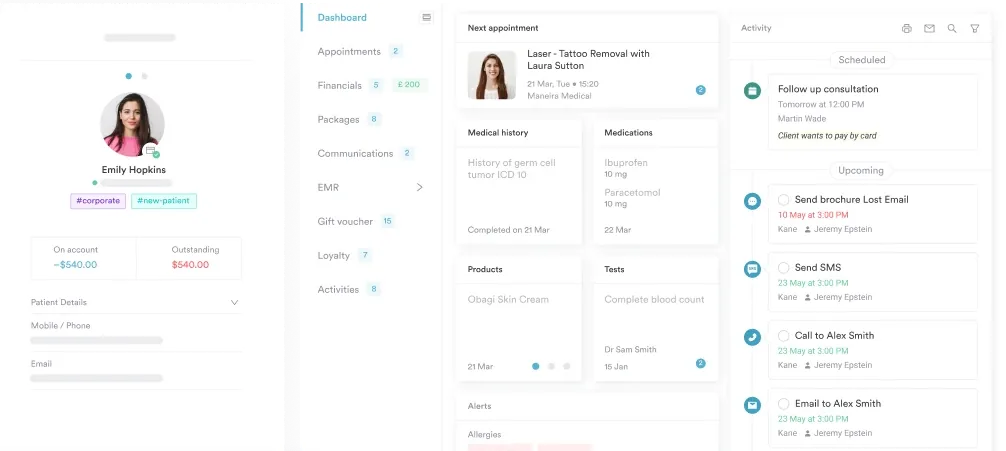
Practice management software like Pabau keeps digital forms and client records in one place, streamlining test ordering and result documentation for CAH, PCOS, and adrenal disorder workups.
A ready-to-use clinical reference covering test indications, reference ranges by age and sex, specimen collection requirements, CPT code 83498, and result interpretation thresholds for CAH, PCOS, and adrenal disorder evaluation.
Download templateThe 17-hydroxyprogesterone test is a cornerstone diagnostic for endocrine conditions affecting reproductive health and adrenal function. This clinical reference guide provides practitioners with essential ordering, interpretation, and documentation information for one of the most frequently ordered hormone tests.
The 17-hydroxyprogesterone (17-OHP) test measures serum levels of 17-hydroxyprogesterone, a hormone intermediate in the cortisol biosynthesis pathway. Produced by the adrenal cortex, this hormone precursor accumulates when the enzyme 21-hydroxylase is deficient or dysfunctional, making 17-OHP measurement the gold standard screening for congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency.
The 17-hydroxyprogesterone test is ordered to evaluate adrenal steroidogenesis, screen newborns for CAH, investigate hyperandrogenic symptoms in reproductive-age females, and assess suspected adrenal insufficiency in adults. It is not a standalone diagnostic but part of a broader hormone panel.
The 17-hydroxyprogesterone test serves multiple diagnostic roles across pediatric and adult medicine:
Modern 17-hydroxyprogesterone testing uses liquid chromatography tandem mass spectrometry (LC/MS or HPLC-MS/MS), which provides superior specificity and accuracy compared to immunoassay. Immunoassay can produce falsely elevated results in neonates due to cross-reactivity with other steroids. LC/MS avoids this pitfall.
Specimen type is serum, not plasma. Collection timing is critical for reproductive-age females. Early follicular phase, days 3-5 of the menstrual cycle, is the standard for comparing results to published reference intervals. Post-ovulation (luteal phase) collections show 3-5 fold higher 17-OHP due to the progesterone rise. If luteal-phase results come back, interpret them against luteal reference ranges, not follicular. Specimen stability is approximately 14 days refrigerated. Verify this with your specific laboratory.
CPT code 83498 is the standard procedural code for 17-hydroxyprogesterone quantification. Reimbursement varies by payer and indication. Verify coverage with the patient’s insurance before ordering. Newborn screening tests are typically covered by state programs and not billed to insurance.
17-OHP reference ranges vary significantly by age, sex, and reproductive status. Results must be interpreted against age- and sex-matched reference intervals. Using the wrong range leads to misinterpretation.
Critical timing note for females: Menstrual cycle phase dramatically affects 17-OHP concentration. Follicular phase (days 3-5) values are lower. Luteal phase (7-10 days after ovulation) values can be 3-5 times higher due to corpus luteum progesterone synthesis. Always document collection date and menstrual cycle phase on requisition forms. Lab reference ranges account for these variations, so confirm your lab’s specific intervals.
Pabau's digital forms and integrated client records keep hormone test requisitions, results, and clinical notes organized in one searchable system.

Elevated 17-OHP in reproductive-age females indicates potential adrenal or ovarian dysfunction. Clinical interpretation depends on degree of elevation and concurrent symptoms.
Low 17-OHP is less commonly clinically significant but may indicate adrenal insufficiency when concurrent with low cortisol and elevated ACTH. Postmenopausal females naturally have lower 17-OHP due to decreased ovarian and adrenal hormone production. Medications, such as glucocorticoids and hormonal contraceptives, suppress 17-OHP. Document medication use on requisition.
Elevated 17-OHP on newborn screening (heel-stick dried blood spot) is the primary marker for CAH in neonates. Screening cutoffs vary by state, typically 30-60 ng/dL depending on assay and birth weight, and are optimized to detect classic CAH while minimizing false positives. Transiently elevated 17-OHP is common in sick neonates, low-birth-weight infants, and premature babies. Confirmatory testing, including serum 17-OHP, ACTH, cortisol, and electrolytes, is always performed before diagnosis.
Diagnosis of neonatal CAH initiates immediate glucocorticoid therapy to prevent adrenal crisis and reduce virilization exposure in affected females. Digital client records ensure tracking of confirmatory test dates and treatment initiation timelines, critical for compliance documentation.
17-OHP monitoring is integral to fertility assessment and treatment in reproductive medicine. Non-classic CAH, detected via elevated 17-OHP, impairs fertility through irregular ovulation, elevated androgens, and abnormal endometrial development. Screening for non-classic CAH is recommended in women with infertility and hirsutism, as glucocorticoid treatment can restore ovulatory cycles.
In fertility treatment cycles, 17-OHP is sometimes measured during baseline assessment to stratify risk for poor ovarian response. Practitioners order the test during follicular phase before cycle initiation to establish baseline adrenal and ovarian steroid function.
Document the following on the requisition to ensure accurate lab interpretation and reference range selection:
The 17-hydroxyprogesterone test is essential for diagnosing and monitoring adrenal disorders, CAH, PCOS, and fertility issues. Understanding reference ranges, collection timing, and result interpretation ensures clinically appropriate ordering and patient care. Download the template above to keep this reference at hand during clinical workflows and patient consultations.
Monitoring ovarian response during fertility treatment? Doppler ultrasound report template documents imaging findings alongside hormone results.
Coordinating care for patients with concurrent endocrine conditions? Diabetes nursing care plan template keeps metabolic monitoring organized alongside hormone panels.
Tracking long-term wellbeing in CAH or PCOS management? Quality of life assessment template gives a structured way to monitor patient-reported outcomes.
The 17-hydroxyprogesterone test measures blood levels of 17-OHP, a hormone intermediate in cortisol production. Elevated 17-OHP indicates 21-hydroxylase enzyme deficiency and is the gold-standard diagnostic marker for congenital adrenal hyperplasia (CAH).
The test screens for and diagnoses congenital adrenal hyperplasia (CAH), evaluates polycystic ovary syndrome (PCOS), investigates hirsutism and irregular periods, detects adrenal tumors, and assesses adrenal insufficiency in both adults and neonates.
Normal adult female 17-OHP ranges from 15-70 ng/dL during the follicular phase of the menstrual cycle; 35-290 ng/dL during the luteal phase; and 7-40 ng/dL if postmenopausal. Collection timing relative to the cycle is critical for interpretation.
Doctors order the 17-hydroxyprogesterone test when evaluating hirsutism, irregular cycles, infertility, newborn screening for CAH, suspected adrenal tumors, or monitoring CAH treatment response. It is also part of comprehensive hormonal panels for reproductive and metabolic assessment.
Yes, elevated 17-OHP on newborn screening (heel-stick dried blood spot) is the primary marker for congenital adrenal hyperplasia. All US states and most developed countries include 17-OHP in mandatory newborn screening panels to detect and treat CAH before adrenal crisis occurs.
CPT code 83498 is the standard billing code for 17-hydroxyprogesterone quantification. Labcorp uses order code 070085, Quest Diagnostics uses test number 17180, and ARUP uses test code 0092332.