CPT code 00103: Anesthesia for eyelid reconstruction billing guide
CPT code 00103 is the anesthesia code for reconstructive procedures on the eyeli...
July 23, 2026
CPT code 99424 covers the first 30 minutes of principal care management (PCM) services per calendar month, personally performed by a physician or qualified healthcare professional (QHP).
Patients must have a single high-risk chronic condition expected to last 3+ months – they cannot be enrolled in chronic care management (CCM) in the same month.
Common billing mistakes include confusing 99424 (physician/QHP time) with 99426 (clinical staff time) and failing to document a disease-specific care plan.
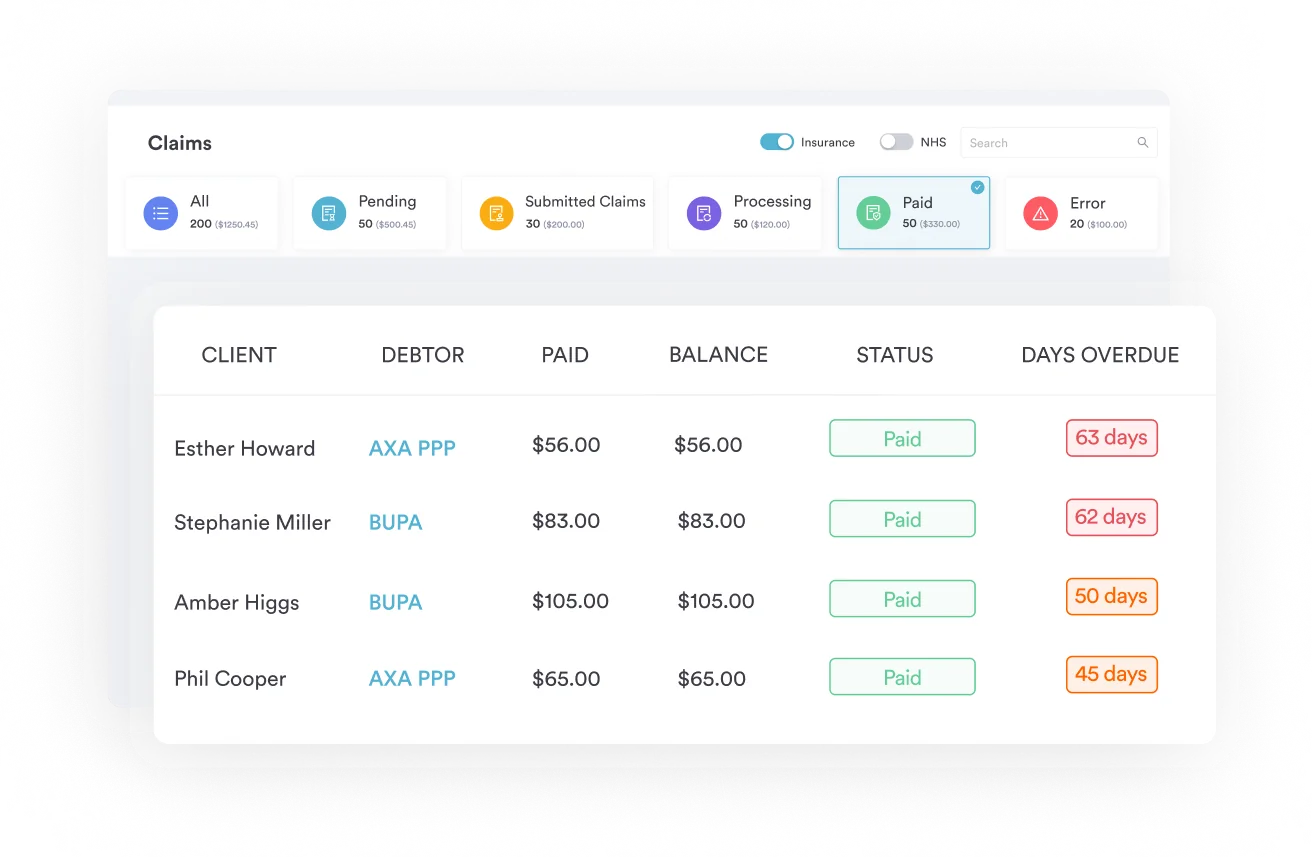
Pabau’s claims management software helps practices track non-face-to-face time, store care plans, and reduce PCM claim denials.
CPT code 99424 is a billable code that covers the first 30 minutes of principal care management (PCM) services per calendar month, personally performed by a physician or qualified healthcare professional (QHP). It applies to patients with a single high-risk chronic condition expected to last at least three months who need structured management but don’t meet the two-condition threshold for chronic care management (CCM).
In plain terms, here’s the 99424 CPT code description: the first 30 minutes of principal care management (PCM) time in a calendar month, personally performed by a physician or QHP for a patient with one high-risk chronic condition. Three related codes cover the rest of the PCM time spectrum:
According to the American Medical Association’s CPT code set, CPT code 99424 is categorized under Principal Care Management Services and covers the first 30 minutes of non-face-to-face time per calendar month. This guide covers the eligibility criteria, time rules, documentation requirements, reimbursement rates, and how 99424 compares with related codes 99425, 99426, and 99427.
Good patient care management workflows make the difference between clean claims and costly denials.
Not every patient with a chronic condition qualifies. PCM has a specific eligibility profile, and getting it wrong leads to denials that are difficult to appeal retroactively.
Good claims management software makes it easier to flag which patients meet these criteria and track whether concurrent billing restrictions apply each month.
CPT 99424 is time-based, and the time clock is strict. CMS counts only the calendar month, not rolling 30-day windows.
Reimbursement figures are approximate and vary by geographic locality. Always verify current PCM rates using the CMS Physician Fee Schedule lookup tool before billing.
Key time rules to know:
Track non-face-to-face time in real time, not retrospectively. Practices that log minutes at the point of activity – a brief note immediately after a coordination call or care plan update – have far cleaner audit trails than those reconstructing time from memory at month end.
Knowing the eligibility rules and time thresholds is only half of PCM billing. The other half is running the same sequence every month so nothing gets missed before the claim goes out. Here’s the workflow a practice can run for each PCM patient:
Running this sequence as a checklist – rather than leaving PCM billing to memory – is what keeps principal care management services auditable when a payer asks for documentation months later.
The most frequent reason PCM claims fail audit is incomplete documentation, specifically around the disease-specific care plan. CMS requires specific elements in the chart, and auditors check for all of them.
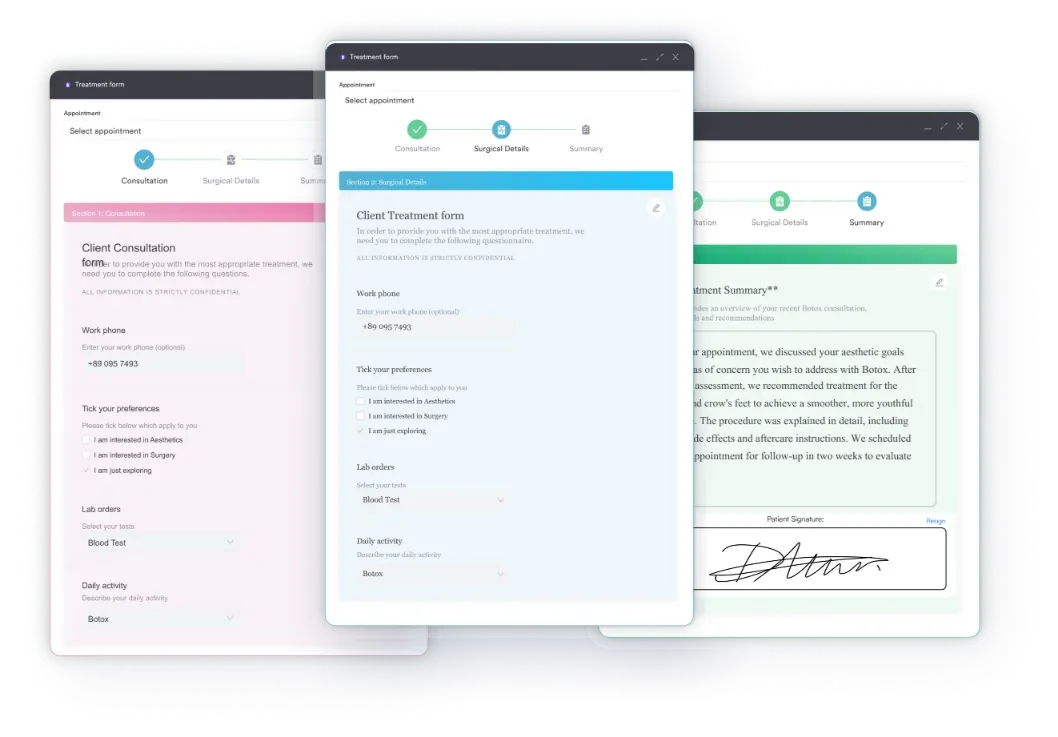
Digital intake forms and structured clinical note templates help practices capture consent, care plan details, and time logs in a consistent, auditable format. Using direct primary care software built for complex patient management also reduces the risk of incomplete documentation at claim time.
Pabau helps physician practices and qualified healthcare professionals document care plans, log non-face-to-face time, and submit clean PCM claims. See how the platform handles the compliance side so your team can focus on patient care.

The four PCM codes divide along two axes: who performs the service and how much time is spent. Getting this wrong is a compliance risk, not just a billing inefficiency.
99424 vs 99426 – the most critical distinction:
99424 is reserved for time personally performed by the billing physician or QHP. 99426 covers the same first-30-minute time block but applies when clinical staff (Nurses, medical assistants) perform the service under general physician supervision. Billing 99424 for services actually delivered by clinical staff is a false claims risk. The distinction matters on every claim, every month.
99424 vs 99425 – base code and add-on:
99425 is an add-on code. It cannot be billed without 99424 on the same claim. When physician or QHP time in a calendar month reaches 60 minutes, the practice bills 99424 plus 99425. Time beyond 60 minutes in a single month is not separately reportable under the current PCM code set.
Practices managing high-acuity panels using primary care software with built-in time tracking can automate the 30-minute threshold alert, reducing the risk of under- or over-billing a given month.
Many practices confuse PCM with CCM because both involve non-face-to-face care management for complex patients. The qualifying conditions are fundamentally different, and billing the wrong code family wastes time on appeals.
PCM was created by CMS for patients with one complex chronic condition who need structured management but are excluded from chronic care management (CCM) because they don’t meet the two-condition threshold. The HCPCS predecessor codes G2064 and G2065 were replaced by the four CPT codes in 2022.
Reviewing your HIPAA compliance checklist for primary care is also worth doing when standing up a PCM program, since patient consent records, care plan storage, and communication logs all fall under protected health information rules.
Review each eligible patient’s chart at the start of the month before assigning a billing code. If the patient now has two or more chronic conditions meeting CCM complexity thresholds, transitioning them to CCM may capture more reimbursement. A monthly eligibility check prevents both underbilling and erroneous PCM claims.
The short answer: physicians and other qualified healthcare professionals who can independently bill Medicare. The nuance matters for multi-practitioner practices.
Incident-to billing rules apply in some cases. When a QHP bills PCM incident-to a physician, the services must still meet CMS incident-to requirements, including direct supervision during the visit where PCM is established.
For practices managing complex billing arrangements, primary care EHR systems that tie time logs to the performing provider’s identity help establish a clean audit trail. Practices using functional medicine software managing high-complexity single-condition patients will find the PCM code set particularly relevant to their billing model.
PCM denials cluster around a handful of avoidable medical billing errors. Knowing them in advance is cheaper than appealing claims after the fact.
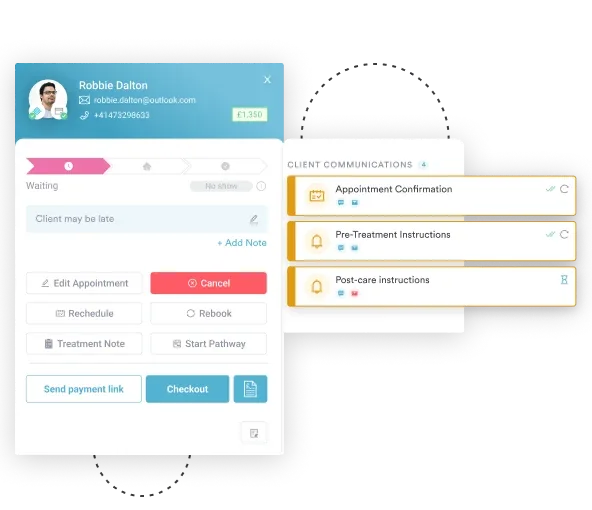
Practices that use automated care workflows to prompt documentation at each touchpoint – rather than relying on month-end reconciliation – have more defensible records when claims are reviewed.
Running a PCM program without a system that tracks time, stores care plans, and flags billing conflicts is operationally unsustainable for most practices. Pabau’s claims management software gives physicians and QHPs a structured way to log non-face-to-face time against individual patient records, attach the disease-specific care plan, and monitor monthly totals before claim submission.
The platform’s compliance tools also help practices manage the documentation requirements that underpin CPT code 99424 audits. For practices already using Pabau for scheduling, records, and billing, adding PCM tracking sits inside the same workflow rather than requiring a separate system.
Find out how well your current setup handles these requirements with a review of established practice management software benchmarks for care management programs.
CPT code 99424 provides a dedicated reimbursement path for patients with a single high-complexity chronic condition. The eligibility rules are specific, the documentation requirements are firm, and the distinction between physician/QHP time (99424) and clinical staff time (99426) is not optional.
Practices that build clean workflows around consent capture, care plan documentation, and time logging will find PCM billing sustainable and auditable. Pabau’s claims management tools are built for exactly this kind of structured, time-based billing. Book a demo to see how the platform handles PCM documentation from consent through claim submission.
Need a structured compliance framework for your practice? HIPAA compliance for medical offices walks through the documentation and consent requirements that overlap with PCM program setup.
Want to reduce claim errors across your billing team? Digital forms help practices capture structured consent and care plan data at the point of care, not retrospectively.
Running a primary care or direct care practice? Direct primary care EHR covers the software features most relevant to practices managing complex chronic patients.
CPT code 99424 is used to bill for the first 30 minutes of principal care management (PCM) services per calendar month for a patient with a single high-risk chronic condition, personally performed by a physician or qualified healthcare professional. Services are non-face-to-face and include care plan development, patient and caregiver communication, and coordination with other providers.
Medicare reimbursement for CPT 99424 is approximately $83 to $88 per month, though the exact amount varies by geographic locality and annual fee schedule updates. Use the CMS Physician Fee Schedule lookup tool to find the current rate for your specific locality before billing.
Both cover the first 30 minutes of PCM per calendar month, but 99424 is for time personally performed by a physician or qualified healthcare professional, while 99426 is for time performed by clinical staff (Such as nurses or medical assistants) under general physician supervision. Billing 99424 for clinical staff time is a compliance error.
Yes, nurse practitioners and physician assistants who meet CMS qualified healthcare professional (QHP) criteria can bill CPT 99424 under their own NPI when they personally perform the PCM services. Eligibility may vary for state Medicaid programs, so verify scope-of-practice rules if billing outside traditional Medicare.
Yes. 99425 is an add-on code for each additional 30 minutes of physician or QHP PCM time beyond the first 30 minutes covered by 99424. When total monthly physician/QHP time reaches 60 minutes, both codes are submitted together on the same claim. 99425 cannot be billed without 99424.
A qualifying patient must have a single high-risk chronic condition expected to last at least three months, require physician-level oversight and a disease-specific care plan, and not be currently enrolled in chronic care management (CCM) in the same calendar month. Written patient consent must be on file before services begin.
Principal care management uses four CPT codes split by who performs the work and how long it takes: 99424 and 99425 cover physician or QHP time (the first 30 minutes and each additional 30 minutes), while 99426 and 99427 cover the same time blocks when clinical staff deliver the service under general supervision. These are the principal care management CPT codes CMS introduced in 2022 to replace the older G2064 and G2065 codes. Together, these principal care management codes let a practice bill for the exact type and amount of non-face-to-face time it delivered that month.
Principal care management and principal illness navigation both apply to a single serious or high-risk condition, but they pay for different work. PCM (99424-99427) pays a physician or QHP, or clinical staff under their supervision, for time spent managing and coordinating a disease-specific care plan. PIN is billed under a separate set of CMS HCPCS codes (G0023 and G0024, plus G0140 and G0146 for peer support) and pays certified or trained auxiliary personnel, such as patient navigators, for helping the patient navigate care rather than for physician-led management. A practice can’t bill PCM and PIN services for the same condition and practitioner in the same month, so confirm which service was actually delivered before choosing a code.