HCPCS Code J9070: Cyclophosphamide 100 mg billing guide
HCPCS Code J9070 identifies cyclophosphamide, 100 mg per billed unit, administer...
Last Updated: July 27, 2026
CPT code 96110 reports developmental screening with a standardized, validated instrument, including scoring and documentation. It covers brief tools like ASQ, M-CHAT-R/F, or PEDS at well-child visits. Modifier 25 attaches to the same-day E/M code, never to 96110 itself, and payer age and frequency limits vary widely.
CPT Code 96110 covers developmental screening using a standardized, validated instrument with scoring and documentation – it does not apply to informal observation or casual questioning.
Modifier 25 attaches to the same-day E/M or preventive medicine code, not to 96110 itself; billing it on the wrong code is one of the most common denial triggers.
Age limits and frequency rules vary significantly by payer; Medicare does not typically cover 96110 as a standalone service, while Medicaid policies differ state by state.
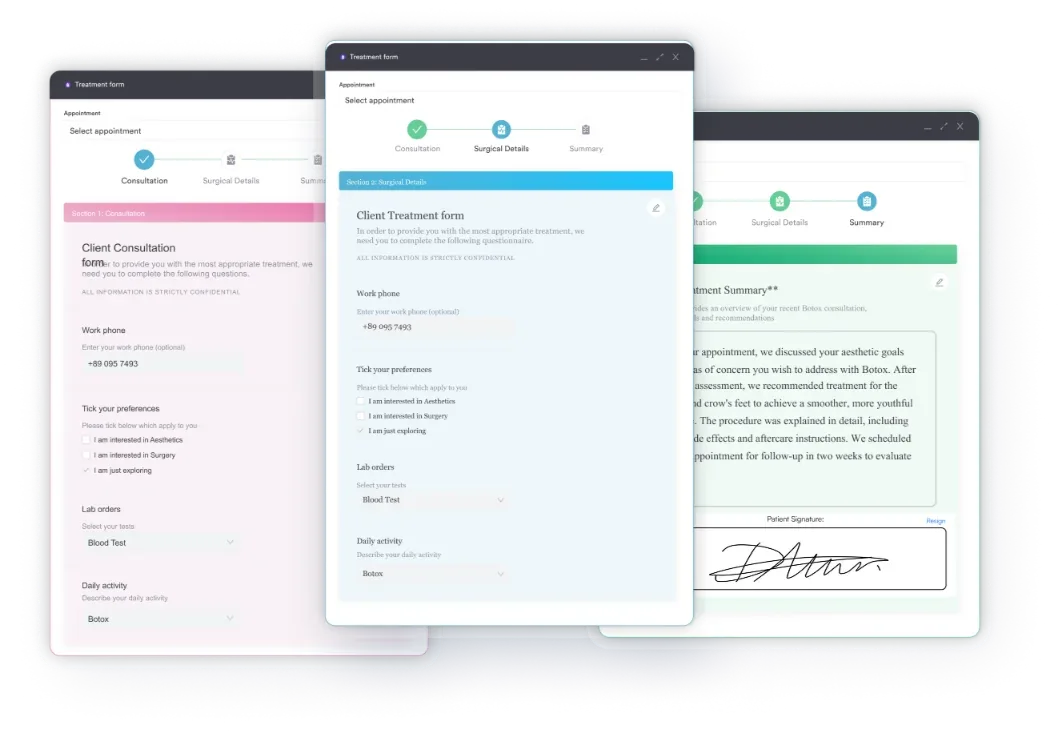
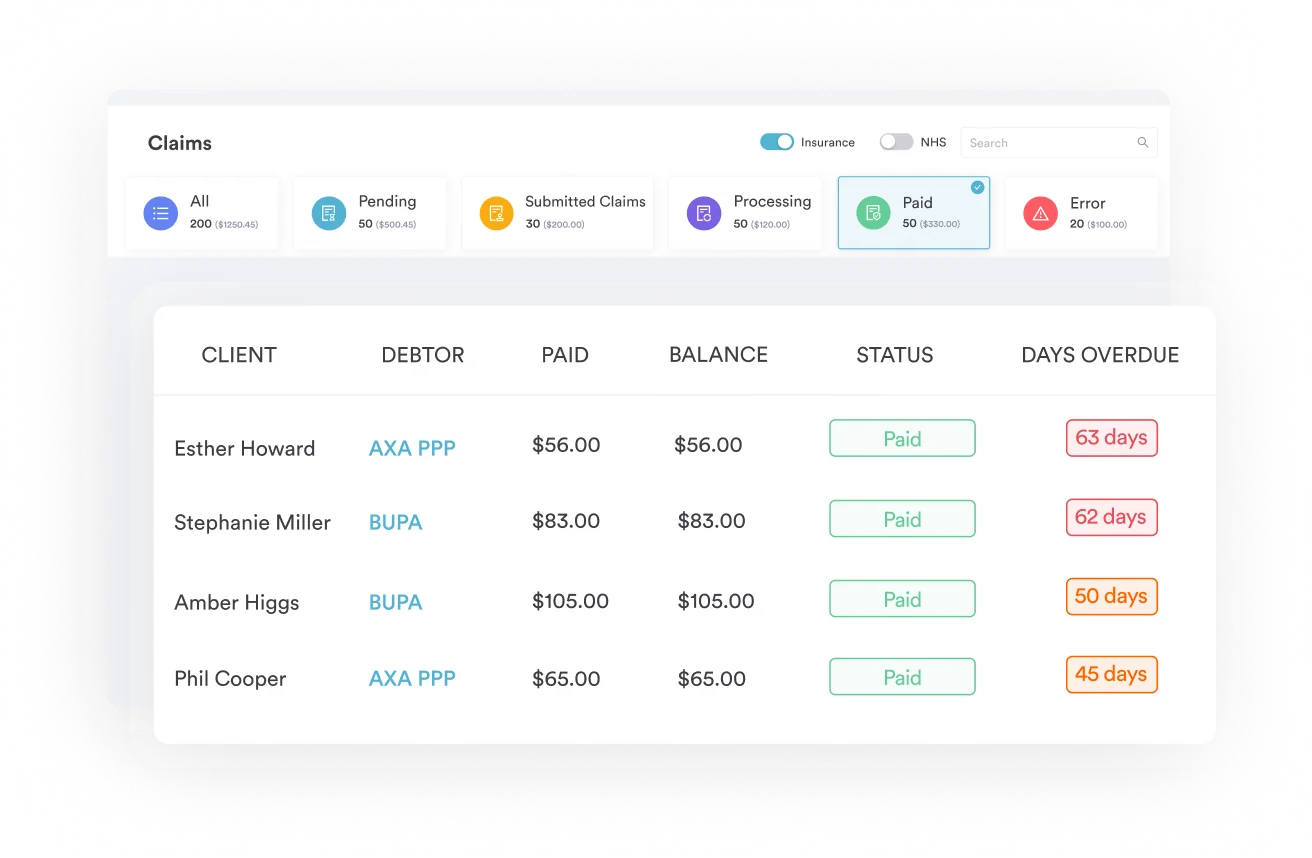
Pabau’s digital forms and claims management software help practices capture screening data and submit 96110 claims accurately from a single workflow.
CPT Code 96110 is a billable code that covers developmental screening using a standardized, validated instrument, with scoring and documentation. It does not apply to informal observation or casual questioning – the screening must use a recognized tool that is scored and recorded in the patient’s record.
The American Medical Association (AMA) defines CPT Code 96110 as: Developmental screening (e.g., developmental milestone survey, speech and language delay screen), with scoring and documentation, per standardized instrument. That last phrase is doing most of the work. Without a validated, scored instrument and clinical documentation, the code does not apply.
CPT Code 96110 sits within the Central Nervous System Assessments/Tests section of the CPT code set, specifically the Developmental and Behavioral Screening and Testing subsection (96110-96113). It is the entry-level code in that family – briefer and less intensive than CPT Code 96112, which requires a trained administrator and covers a broader battery of developmental domains.
96110 applies when a provider administers a formal developmental screening tool, scores it according to the instrument’s instructions, and documents the results in the patient record to support clinical decision-making and to guide referral, though any specialist care that follows is billed under separate code families far removed from screening, such as anesthesia for intracranial vascular procedures (CPT code 00216). Common clinical scenarios include:
The code is not appropriate for informal developmental questions asked during a routine exam, general clinical observation without a scored tool, or chart review without direct patient interaction. Using digital intake forms to pre-populate screening instruments before the encounter helps ensure the screening is captured correctly and consistently across every visit.
Payers require that the tool used is standardized, validated, and appropriate to the patient’s age and clinical presentation. No single national list defines every acceptable instrument, but the following are broadly recognized across commercial, Medicaid, and AAP guidance.
Using multiple instruments in the same visit is allowed. According to guidance from pedstestonline.com, a practice using PEDS, PEDS:DM, and M-CHAT-R/F together may bill 96110 three times on the same date (96110 x 3), provided each instrument is scored and documented separately. Confirm this approach with your specific payer before billing, as not all plans follow this interpretation.
Most CPT 96110 denials trace back to one of three errors: applying the modifier to the wrong code, failing to document the instrument used, or billing 96110 without a same-day E/M when the payer requires one. Getting the billing logic right protects both the claim and any post-payment audit.
CPT Code 96110 is frequently billed on the same date as a well-child visit (preventive medicine E/M) or a problem-focused office visit. When that happens, Modifier 25 is required on the E/M or preventive medicine code, not on 96110. Modifier 25 signals to the payer that the E/M is a separate, distinct service from the developmental screening.
The claim line structure should look like this:
Appending Modifier 25 to 96110 itself is incorrect and will typically result in a denial or reduced payment. The AAP’s coding fact sheet, referenced across multiple authoritative sources, confirms this modifier placement. Review your HIPAA compliance practices for medical offices to ensure documentation supporting Modifier 25 is maintained in the record.
The clinical record must include the name of the screening instrument, the date administered, the score obtained, and the provider’s interpretation or clinical action taken based on results. Documentation that says only “developmental screening performed” without naming the tool or recording a score does not support billing CPT Code 96110.
A structured note should capture: instrument name, version, score per domain (where applicable), total score or risk category, and next steps (e.g., monitoring at next visit, referral to early intervention, or parental education provided). Practices using a mental health EMR or pediatric practice management system with built-in screening templates can standardize this documentation across all providers.
Flag every 96110 claim for chart documentation before submission. Confirm the instrument name, score, and clinical interpretation are present in the note. A claim that passes initial adjudication can still be recouped on audit if the record doesn’t substantiate the service.
Reimbursement for CPT Code 96110 varies by payer, geographic locality, and contract terms. The figures below reflect general 2026 benchmarks; verify current rates using the CMS Physician Fee Schedule lookup tool or your payer-specific fee schedule before billing.
For a precise 2026 RVU lookup and geographic locality adjustment, the PCC free 2026 RVU/RBRVS calculator imports CMS fee schedule data and accounts for location multipliers. This is particularly useful for practices billing across multiple sites or states.
When billing for ADHD screening billing requirements alongside 96110, confirm whether your payer bundles behavioral screening instruments under a single unit of 96110 or allows separate reporting per instrument administered.
Pabau's claims management tools help pediatric and family medicine practices capture developmental screening data, attach the right modifiers, and submit clean claims from a single workflow.

Age limits for CPT Code 96110 are one of the most payer-variable aspects of billing this code. There is no single universal rule: commercial plans, state Medicaid programs, and managed care organizations each set their own parameters. Assuming a universal age cutoff is a fast path to denials.
Two well-documented state-specific rules illustrate how much variation exists:
Other states take a broader view and allow 96110 up to age 21 within Medicaid EPSDT (Early and Periodic Screening, Diagnostic, and Treatment) benefit structures. Check your state Medicaid agency’s billing manual or fee schedule before assuming any universal upper age limit applies to your patient population.
Frequency rules are similarly payer-specific. Many plans limit 96110 to once per rolling 12-month period outside of specific screening schedules tied to well-child visit protocols.
Some state Medicaid programs align frequency with AAP Bright Futures guidelines, which recommend developmental screening at 9, 18, and 24-30 months, plus autism-specific screening at 18 and 24 months. Billing 96110 more frequently than the payer allows without documentation of clinical necessity is a common audit trigger.
Practices seeing children with known developmental concerns or those enrolled in early intervention should document the medical necessity for any screening that falls outside standard well-child visit intervals. For practices also managing ICD-10 codes for autistic disorder — or a developmental disorder of motor function (F82) flagged by a milestone screen — alongside developmental screenings, accurate cross-referencing between the screening result and the diagnosis code strengthens medical necessity documentation.
Run a quarterly payer policy audit on 96110. Medicaid programs update age and frequency rules with little notice – a policy that allowed annual billing last year may have shifted to once every 18 months. Catching policy changes before they generate denials is cheaper than working reconsiderations.
CPT Code 96110 is the least intensive code in the developmental and behavioral screening family. Knowing when to use the related codes prevents both undercoding (leaving revenue on the table) and overcoding (billing a more intensive service than what was delivered).
The critical distinction is who administers the test and how long it takes. CPT Code 96110 covers brief, standardized screeners – the kind a parent fills out in the waiting room or a provider completes in five to ten minutes. CPT Code 96112 requires a trained examiner conducting a systematic evaluation across multiple developmental domains, typically taking at least 60 minutes.
Using 96112 for a service that was actually a brief screening tool administered at a well-child visit is overcoding. Conversely, using 96110 for a full developmental testing battery lasting an hour or more leaves significant reimbursement uncaptured. Document the time spent and the instruments used to support whichever code you bill. For guidance on similar behavioral health billing patterns, see related behavioral health CPT codes and how they interact with screening and assessment services.
96127 covers emotional and behavioral assessments (such as PHQ-A for adolescent depression or the Pediatric Symptom Checklist). It is distinct from 96110 and can be billed on the same date when a provider administers both a developmental screening and a separate emotional/behavioral instrument. Each must be independently scored and documented. Some payers bundle these under a single unit; review your payer’s MUE (medically unlikely edit) policy before billing both on the same date.
For practices managing pediatric developmental workflows alongside autism spectrum coding, the clinical guidance on autism and speech delay assessment provides context on how diagnostic and screening codes interact in a complete patient workup — one that may also reach other F-chapter diagnoses, from a brief psychotic disorder (F23) to an unspecified dissociative and conversion disorder (F44.9), when the clinical picture warrants. Practices running multi-provider pediatric settings benefit from claims management software that flags bundling conflicts automatically before claims leave the practice.
For practices managing ADHD evaluations alongside developmental screenings, see how Vanderbilt ADHD Rating Scale scoring intersects with the 96110-96127 billing decision, particularly when both instruments are administered at the same well-child visit. Practices running ADHD-focused services can also explore dedicated ADHD clinic software to streamline screening workflows and documentation requirements across both code types.
CPT Code 96110 denials almost always come down to the same issues: a modifier on the wrong code, documentation that names a screening but not a standardized instrument, or a billing pattern that exceeds payer-specific age or frequency limits. None of these are hard to fix once the rules are clear.
Pabau’s automated billing workflows and built-in digital forms help pediatric and family medicine practices standardize how developmental screenings are documented, modifier rules are applied, and claims are submitted. To see how it works in practice, book a demo with the team.
Curious how a pediatric-focused practice management platform handles screening workflows? Digital forms shows how Pabau captures standardized instrument results at the point of care and feeds them directly into clinical documentation.
CPT Code 96110 is used to bill for developmental screening using a standardized, validated instrument with scoring and documentation. It applies when a provider administers a recognized tool (such as ASQ, M-CHAT-R/F, or PEDS), scores it according to the instrument’s protocol, and documents the results and clinical interpretation in the patient record. It does not apply to informal developmental questions or observation without a scored instrument.
Age limits vary by payer. California Medi-Cal restricts 96110 to patients through age 6 for general developmental screenings (per DHCS bulletin 20-687). Texas Medicaid restricts it to age 6 outside of Texas Health Steps. Many commercial plans cover 96110 for pediatric patients broadly, and some state Medicaid programs allow billing up to age 21 under EPSDT benefits. Always verify with the specific payer.
CPT Code 96110 itself does not typically carry a modifier. When billed on the same day as a well-child visit or other E/M service, Modifier 25 attaches to the E/M or preventive medicine code, not to 96110. Placing Modifier 25 on 96110 is a common error that causes denials.
Reimbursement varies by payer and geographic locality. Medicaid rates typically range from $15-$35 per unit; commercial plans generally pay $20-$50 per unit. Medicare does not typically cover 96110 as a standalone service. Use the CMS Physician Fee Schedule lookup tool or your payer’s fee schedule for current, location-specific rates.
CPT Code 96110 covers a brief standardized screening tool (typically parent-completed or completed in under 15 minutes), while CPT Code 96112 covers a more intensive developmental test administered by a trained examiner over at least one hour across multiple developmental domains. Using 96112 for a brief screener is overcoding; use 96110 for screeners like ASQ or M-CHAT and 96112 for comprehensive developmental testing batteries.
Yes. CPT Code 96110 may be billed on the same date as a well-child visit (preventive E/M) or problem-focused office visit. The E/M or preventive medicine code must carry Modifier 25 to indicate it is a separate, distinct service. Some payers may still bundle the screening into the E/M; verify your payer’s specific policy before billing both on the same date.