HCPCS Code A4208: Sterile syringe with needle, 3 cc billing guide
Incorrect unit reporting is the most common reason A4208 claims get denied on fi...
July 27, 2026
CPT code 80307 reports presumptive drug tests performed using instrumented chemistry analyzers, chromatography, or mass spectrometry, covering any number of drug classes from a single specimen in one billable unit.
Bill 80307 only once per date of service regardless of how many drug classes are tested; definitive testing codes (G0480-G0483) cannot be separately billed on the same date of service.
Medicare does not reimburse 80307 and G0480 on the same DOS; pass-through billing of drug testing services performed by another entity is prohibited by payers including BCBS.
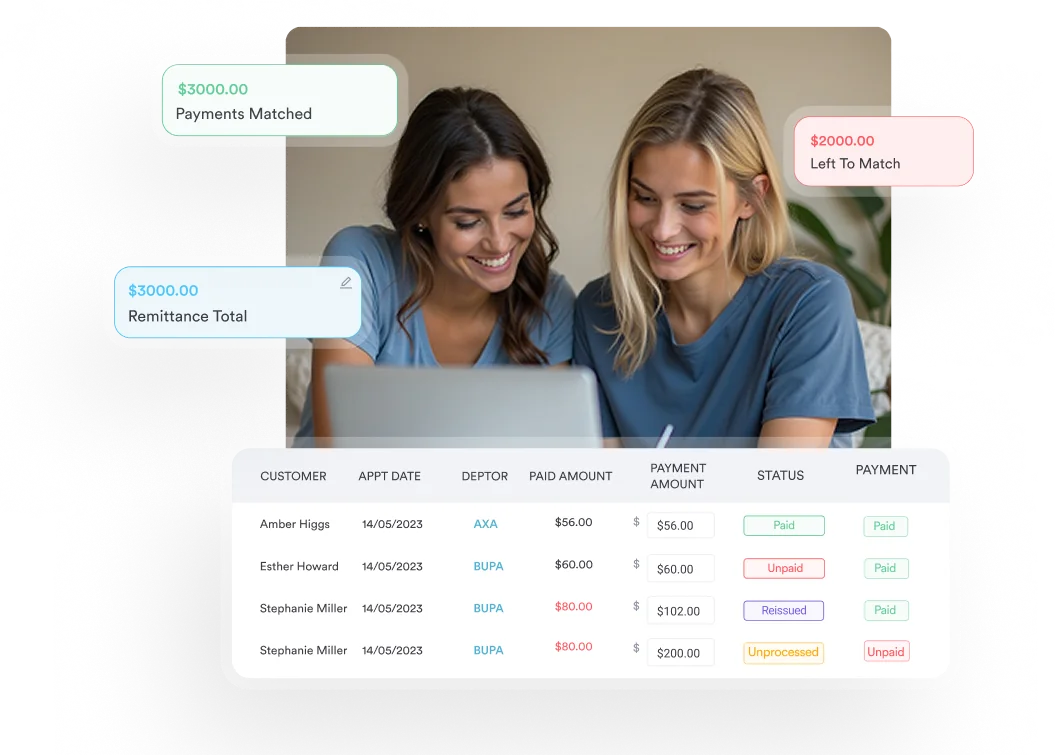
Pabau’s claims management software helps practices document medical necessity, flag same-day bundling conflicts, and reduce denial rates on 80307 claims before submission.
CPT code 80307 reports a presumptive drug test run on an instrumented chemistry analyzer, covering any number of drug classes from a single specimen and billed once per date of service. It is a qualitative screen: the result shows whether a drug class is present or absent, not the concentration.
The American Medical Association (AMA) descriptor reads: Drug test(s), presumptive, any number of drug classes, any number of devices or procedures; by instrument chemistry analyzers (eg, utilizing immunoassay [EIA, ELISA, EMIT, FPIA, IA, KIMS, RIA]), chromatography (eg, GC, HPLC), and mass spectrometry either with or without chromatography; includes sample validity testing, per date of service, any number of drug classes.
Pain management practices, substance use disorder programs, and medication-assisted treatment (MAT) practices are the primary settings where 80307 appears on claims.
80307 screens for the presence or absence of a drug or drug class. It does not confirm the specific drug’s identity or quantify concentration, which is the job of definitive testing. The analyzer technology separates 80307 from the simpler 80305 and 80306 codes.
Common drug classes screened under CPT code 80307 include:
The code covers any number of drug classes tested in a single encounter. A 10-panel screen and a 20-panel screen are both reported as one unit of 80307. The technology level, not the panel size, determines the correct code.
The three presumptive drug testing codes are separated by the method used to read results. Choosing the wrong one is the most common reason practices face medical-necessity downcodes on drug screen claims. The table below maps each code to its method:
Key distinction for 80306 vs 80307: 80306 is read by an instrument that assists direct optical observation (the device highlights the color change), while CPT code 80307 requires a full instrumented chemistry analyzer that processes the reaction and reports a digital result. If your practice uses a benchtop analyzer rather than a handheld optical reader, 80307 is the correct code.
Sample validity testing (creatinine, pH, oxidant, specific gravity) is included in all three codes when performed and cannot be separately billed. The same complexity-tier logic governs other screening families; see our guide to ADHD screening CPT codes.
For Medicare patients, definitive drug testing is billed with HCPCS G-codes, not the CPT 80320-80377 series. The definitive codes are:
The critical billing rule: CPT code 80307 and G0480 cannot both be reimbursed on the same date of service for a Medicare beneficiary. The presumptive screen (80307) and the definitive confirmation (G0480 tier) are mutually exclusive on the same DOS. Per Fidelis Care clinical policy and confirmed by BCBS IL CPCP020 (2026), only one definitive drug testing code is eligible for reimbursement when reported for the same patient on the same date.
Many commercial payers follow the same logic even when they are not bound by Medicare rules. Before submitting both on the same DOS, verify the specific payer’s drug testing policy, which is a frequent point of variation for state Medicaid programs. Practices billing fertility services face a similar payer-specificity challenge, covered in our guide to IVF CPT codes.
Flag all drug testing claims for same-day DOS review before submission. Build a pre-submission check in your billing workflow: if 80307 and any G0480-G0483 code appear on the same claim, hold for review. A five-minute audit before submission prevents a 30-day denial cycle.
80307 is priced on the Medicare Clinical Laboratory Fee Schedule (CLFS), which sets a single national payment rate. There are no relative value units (RVUs), no geographic or locality adjustment, and no facility versus non-facility split. The current rate is published on the CMS Clinical Laboratory Fee Schedule.
For 2026, the national CLFS rate for 80307 is approximately $62 (about $62.14), and Medicare generally pays in the range of $60 to $80. Because the rate is national, it does not change by MAC jurisdiction or place of service. Confirm the current figure on the CLFS before using it in financial projections, since CMS updates the lab fee schedule annually.
Reimbursement points to keep in mind:
Because 80307 has no RVUs, RVU and conversion-factor lookup tools do not apply to it. To confirm current payment, look up code 80307 on the CMS Clinical Laboratory Fee Schedule for the current year.
Pabau's claims management tools help pain management and substance use disorder practices catch same-day bundling conflicts, document medical necessity, and submit cleaner drug testing claims from day one.

Payers require medical necessity documentation for every 80307 claim, with diagnosis codes linked to the clinical rationale for testing. These ICD-10-CM categories are the ones payers most commonly accept for 80307:
| ICD-10-CM Code | Description | Common use case |
|---|---|---|
| F11.10-F11.99 | Opioid use disorder | MAT monitoring, pain management |
| F12.10-F12.99 | Cannabis use disorder | Substance use program monitoring |
| F14.10-F14.99 | Cocaine use disorder | SUD program monitoring |
| F19.10-F19.99 | Other/multiple substance use disorder | Multi-drug SUD programs |
| Z79.891 | Long-term (current) use of opiate analgesic | Chronic pain management adherence |
| G89.29 | Other chronic pain | Chronic pain patient monitoring |
| Z04.89 | Encounter for examination for other purposes | Pre-employment or forensic screening |
CMS guidance (Medicare Coverage Database articles A56915 and A56818) specifies that diagnosis codes must be coded to the highest level of specificity. Submitting F11.10 when the patient’s documented status is F11.20 (opioid use disorder, moderate, uncomplicated) is a documentation mismatch that auditors flag.
Practices treating patients with mental health conditions such as brief psychotic disorder that require medication monitoring should ensure their ICD-10 codes reflect the treating diagnosis, not just the reason for the screen. Substance use disorder programs that pair testing with structured intake can standardize screening using validated instruments such as the AC-OK screen for co-occurring disorders or an internet addiction test for co-occurring behavioral concerns.
When 80307 is ordered during an evaluation and management visit, such as a new patient office visit, the note for that encounter should carry the ordering rationale. Medical necessity documentation should include:
Structured clinical documentation saves the most time during audits. Digital intake forms that capture patient consent and clinical rationale at the point of care keep the supporting detail attached to each claim. For practices managing HIPAA obligations alongside billing, the HIPAA compliance checklist for primary care covers the documentation retention rules that apply to drug testing records.
These billing rules govern how 80307 is submitted and what triggers a denial.
80307 may only be billed once per date of service, regardless of how many drug classes are screened or how many specimens are collected. A 10-panel and a 12-panel run on the same patient on the same day count as one unit of 80307. This is confirmed by both Fidelis Care clinical policy and BCBS IL CPCP020 (2026).
A provider may only bill for services the provider (or the provider’s staff under direct supervision) actually performs. If a practice sends specimens to a reference lab and the lab performs the 80307 analysis, the practice cannot bill 80307 as if it performed the test itself.
BCBS IL CPCP020 (2026) explicitly prohibits pass-through billing. Violating this rule creates compliance exposure beyond simple claim denial. The full scope of HIPAA compliance for medical offices shows where billing and documentation obligations intersect.
Drug confirmation testing is considered included in CPT codes 80305 through 80307. You cannot bill a separate confirmation code alongside 80307 on the same DOS. Per Moda Health RPM016 policy, any confirmation or definitive testing claimed on the same date as 80307 will be bundled and denied.
Modifiers for 80307 are relatively uncommon compared to procedure codes, but the following apply in specific scenarios:
A pain management practice runs a 12-panel presumptive screen on a benchtop chemistry analyzer for a Medicare patient on long-term opioid therapy. Here is how the single claim line resolves:
Review your payer contracts annually for drug testing policies. BCBS, Aetna, Anthem, and Moda Health all maintain clinical payment and coding policies (CPCPs) that specify 80307 coverage criteria, frequency limits, and documentation requirements. Policies update mid-year without notice, so schedule a quarterly policy review as a standing task.
Most 80307 denials fall into three categories: missing medical necessity, same-day bundling, and pass-through billing errors. A fourth category, frequency violations, is less common but increasingly audited by Medicaid programs.
When 80307 claims are denied for medical necessity, the appeal should include:
Practices that use claims management software with built-in denial tracking can identify patterns in 80307 rejections across providers, pinpointing whether denials cluster around a specific ICD-10 code, provider, or payer. That visibility turns reactive denial handling into a repeatable process, the same discipline covered in our guide to CPT code 97014 billing and denial prevention.
Teams comparing systems before they build these checks can start with our roundup of the best medical billing software in the US.
Federal payer rules set the floor. Commercial payers can be more restrictive. These are the most commonly referenced payer-specific positions on 80307:
Behavioral health programs that bill alongside drug testing, such as community support services under HCPCS H2015, face the same payer-specific documentation demands. Practices billing across multiple states or payers should maintain a payer-specific policy matrix updated at least quarterly. Automated billing workflows can route claims to payer-specific rule sets before submission, reducing manual policy lookups.
For practices choosing a system to manage documentation across multi-payer environments, the billing-rule flexibility described in our guide to practice management software applies directly to drug testing complexity.
CPT code 80307 denials follow predictable patterns: same-day bundling with G0480, missing medical necessity documentation, pass-through billing errors, and once-per-DOS violations. Each is preventable with the right billing rules in place before submission. For teams new to revenue cycle work, our overview of what medical billing involves covers the fundamentals behind these rules.
Pabau’s claims management software helps practices that bill 80307 regularly build pre-submission checks that catch same-day conflicts, track denial reasons by payer, and document medical necessity at the point of care. To see how it works in a pain management or substance use disorder billing workflow, book a demo with the team.
List Item #1
List Item #2
CPT code 80307 is a presumptive drug testing code used to report qualitative drug screens performed using instrumented chemistry analyzers, chromatography, or mass spectrometry. It covers any number of drug classes tested from a single specimen on a single date of service and includes sample validity testing when performed.
All three are presumptive drug testing codes, but the reading method differs. 80305 uses direct visual observation (the provider reads the result with the naked eye), 80306 uses instrument-assisted optical observation (a device highlights the result), and 80307 uses a full instrumented chemistry analyzer that processes and reports results digitally. The method, not the number of drugs tested, determines the correct code.
No, not for Medicare patients. CMS and multiple commercial payers prohibit reimbursement of both a presumptive screen (80307) and a definitive test (G0480) on the same date of service for the same patient. If both are submitted, the payer will typically pay only the higher-valued service and deny the other.
80307 is priced on the Medicare Clinical Laboratory Fee Schedule (CLFS) at a single national rate of approximately $62 (about $62.14) for 2026, with Medicare generally paying in the range of $60 to $80. The rate does not vary by MAC jurisdiction, geographic locality, or place of service. Confirm the current amount on the CMS Clinical Laboratory Fee Schedule before use in financial projections.
Once. Regardless of how many drug classes are tested, how many panels are run, or how many specimens are collected, 80307 is billed as a single unit per date of service. Multiple units on a single DOS will be denied by Medicare and most commercial payers.
The most common ICD-10 pairings are opioid use disorder codes (F11.10-F11.99), other substance use disorder codes (F12-F19), long-term opioid use (Z79.891), and chronic pain (G89.29). The diagnosis code must reflect the clinical condition that makes drug monitoring medically necessary, coded to the highest level of specificity.
Modifier 59 (distinct procedural service) may apply in specific payer-required unbundling scenarios, and modifier 91 (repeat clinical diagnostic test) can be used when a test is legitimately repeated on the same DOS for a clinical reason such as a dilute specimen. Modifier QW does not apply to 80307, which is a moderate- or high-complexity test; QW is used with 80305 for CLIA-waived point-of-care screening.
80307 most commonly applies to urine specimens, but the code itself does not specify specimen type. It can be used for other specimen types (oral fluid, blood) when the testing method involves an instrumented chemistry analyzer, chromatography, or mass spectrometry. Urine remains the dominant specimen type in pain management and SUD program billing.