








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT code 44227 describes laparoscopy, surgical, closure of enterostomy, large or small intestine, with resection and anastomosis, maintained by the American Medical Association (AMA).
44227 appears on the CMS Medicare Inpatient-Only Procedure List, meaning it cannot be billed for outpatient or ambulatory surgery center cases under Medicare.
Common coding errors include confusing 44227 with open counterpart CPT 44620, incorrectly sequencing it with 44207, and missing documentation of anastomosis technique.
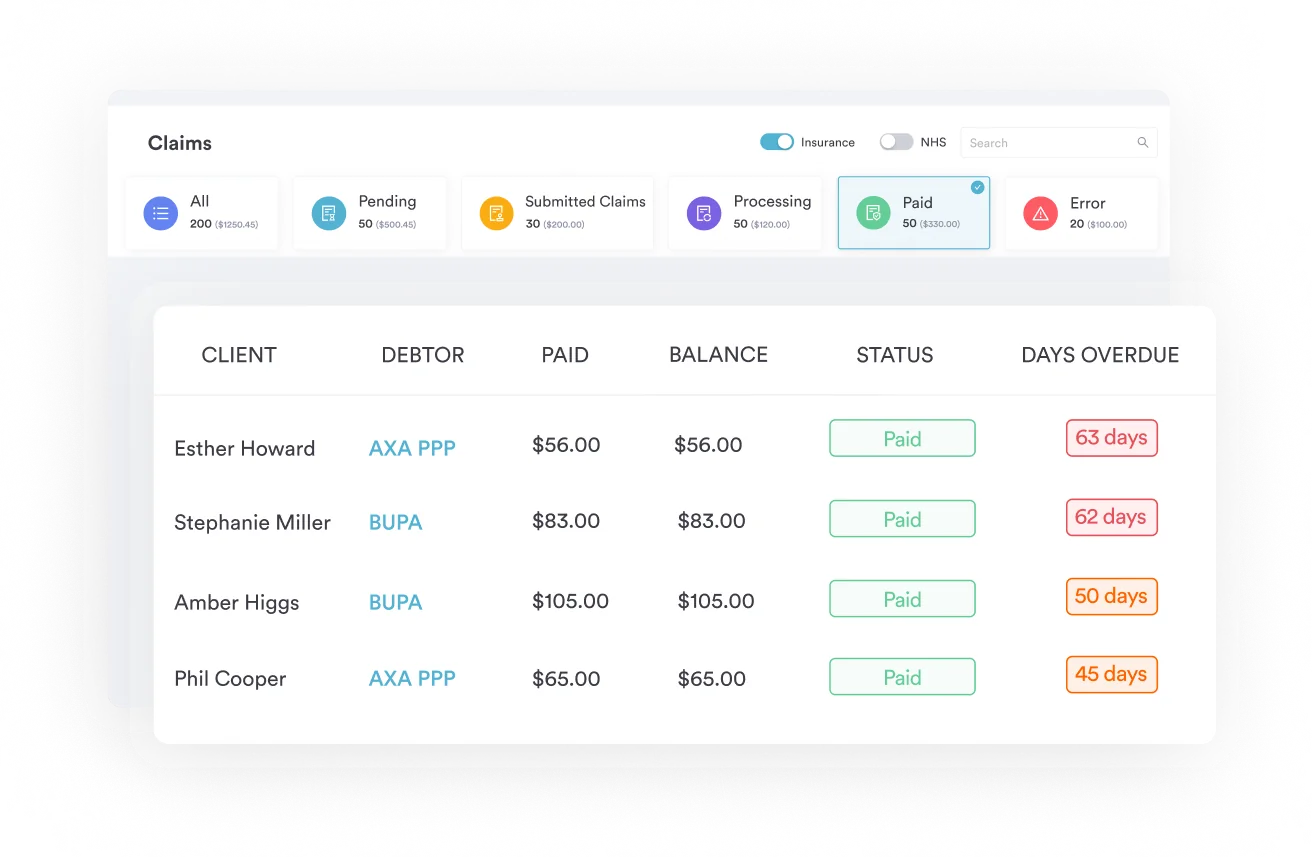
Pabau’s claims management software and digital surgical documentation forms help general surgery practices reduce claim denials and maintain compliant operative records for 44227 submissions.
CPT code 44227 is the code for laparoscopy, surgical, closure of enterostomy of the large or small intestine, with resection and anastomosis. It carries an inpatient-only Medicare designation, specific modifier rules, and several adjacent codes that are easy to confuse.
Surgical coders working in general surgery and colorectal practices encounter 44227 most frequently in the context of stoma reversals following Hartmann’s procedure, diverting ileostomy takedowns, and colostomy closures. Getting the code right requires understanding what the descriptor actually requires, how it differs from open and unlisted alternatives, and what CMS says about its inpatient-only status.
CPT code 44227 describes: Laparoscopy, surgical, closure of enterostomy, large or small intestine, with resection and anastomosis. This descriptor appears in the Laparoscopic Repair Procedure on the Intestines (Except Rectum) section of the AMA CPT code set, as confirmed by AAPC Codify and the NIH Value Set Authority Center.
Three elements must all be present to justify this code:
If anastomosis is not performed or the approach is open rather than laparoscopic, a different code applies. The resection-and-anastomosis requirement is the most commonly missing documentation element that triggers claim denials.
Surgeons use CPT code 44227 in several distinct clinical scenarios. Understanding those scenarios helps coders verify that the reported code matches what was actually performed.
The most common use case is laparoscopic Hartmann’s reversal. In a Hartmann’s procedure, the sigmoid colon is resected and an end colostomy is created. Reversal involves closing that colostomy and reconnecting the colon to the rectal stump via anastomosis, all performed laparoscopically.
Peer-reviewed research published in the Journal of the American College of Surgeons (2023) and a SAGES abstract (2014) both used CPT 44227 to identify laparoscopic-assisted Hartmann’s reversal cases in the ACS-NSQIP database.
The second scenario is loop ileostomy or colostomy takedown with anastomosis. When a temporary diverting stoma created to protect a downstream anastomosis is reversed laparoscopically with bowel resection and reconnection, 44227 is appropriate.
A 2023 NSQIP analysis distinguished loop stoma reversals (CPT 44227, 44620, 44625) from Hartmann’s reversal (CPT 44626), confirming 44227’s scope in both contexts.
For teams managing plastic and general surgery EMR software, linking operative notes directly to CPT codes in the workflow reduces the risk of miscoding at the point of scheduling or charge capture.
Choosing between 44227 and its related codes is where most coding errors occur. The table below compares the most commonly confused codes.
The critical distinction between 44227 and 44626 comes up most often in Hartmann’s reversal billing. CPT 44626 is specifically designated for open Hartmann’s reversal with coloproctostomy. When the same procedure is performed laparoscopically, 44227 is the correct code, not 44626 — the same laparoscopic-versus-open distinction that governs codes such as CPT code 47562 for gallbladder removal. The 2023 NSQIP study explicitly separated these two codes to distinguish laparoscopic from open approaches.
For ICD-10 diagnostic code pairing with procedural codes, accurate code selection depends on matching the operative approach documented in the clinical record. When the approach code and the procedure code conflict, payers routinely reject the claim.
Modifier selection for 44227 requires careful review of what was performed alongside the stoma closure. Misapplied modifiers are a leading cause of downcoded or denied claims for this procedure.
Always verify current HIPAA compliance for medical offices requirements when sharing modifier documentation across care team members or with billing partners. NCCI edit tables are updated quarterly, so a modifier combination that was appropriate last year may now be bundled.
Before appending modifier 59 to any combination involving 44227, run both codes through the CMS NCCI edit tables for the current quarter. The tables specify whether an edit is ‘with modifier’ or ‘without modifier’ and which modifier indicator applies. Submitting without checking the current edit is the single fastest way to generate a denial that takes 60-plus days to appeal.
CPT 44227 is a major surgical procedure with substantial relative value units (RVUs). Reimbursement rates vary by geographic location, payer contract, and the CMS Medicare Physician Fee Schedule (MPFS) conversion factor for the applicable year. Coders and practice managers should verify current figures directly through the CMS Physician Fee Schedule lookup tool.
Key reimbursement factors for CPT 44227:
Commercial payer rates for 44227 typically exceed Medicare rates, though the differential varies significantly by contract. Practices with claims management software can track payer-specific reimbursement patterns for high-RVU codes like 44227 and flag underpayments before the appeal window closes.
CPT 44227 appears on the CMS Medicare Inpatient-Only (IPO) Procedure List. This designation has direct billing consequences that general surgery practices must understand.
Under the Hospital Outpatient Prospective Payment System (OPPS), procedures on the inpatient-only list are excluded from Medicare payment when performed in an outpatient or ambulatory surgery center (ASC) setting. Specifically:
The inpatient-only designation is published annually in CMS Addendum E and reviewed each year as part of the OPPS final rule. Practices should verify 44227’s IPO status against the current CMS OPPS Addendum E at the start of each calendar year, as designations can change.
For related stoma and intestinal procedure coding, the inpatient-only rule is one of the most consequential compliance factors in surgical billing, because a single inadvertent outpatient claim can generate a Medicare overpayment that triggers a full repayment demand.
Pabau's claims management tools help general surgery practices track modifier usage, link operative documentation to CPT codes, and flag high-risk claims before submission. See how it works for your practice.

Pairing the correct ICD-10-CM diagnosis code with CPT 44227 is a medical necessity requirement. Payers use the diagnosis code to determine whether the procedure was clinically indicated. A mismatch between the ICD-10 code and the operative indication is one of the most common reasons surgical claims are returned for additional documentation.
Commonly paired ICD-10-CM codes for CPT 44227 include:
Always document the specific clinical indication in the operative report and pre-operative note, not just the stoma status. Payers expect the underlying condition that led to the original stoma creation to be reflected in the diagnosis code selection, not only the presence of the stoma itself.
Insufficient operative documentation is the most preventable cause of 44227 claim denials. The operative report must support every element of the code descriptor.
Required documentation elements:
Pre-operative documentation should include the clinical indication for stoma reversal, the patient’s history of the original stoma creation procedure, and any pre-authorization obtained from the payer. Using digital surgical documentation forms that capture structured pre-operative and operative data reduces the risk of incomplete records at the time of claim submission.
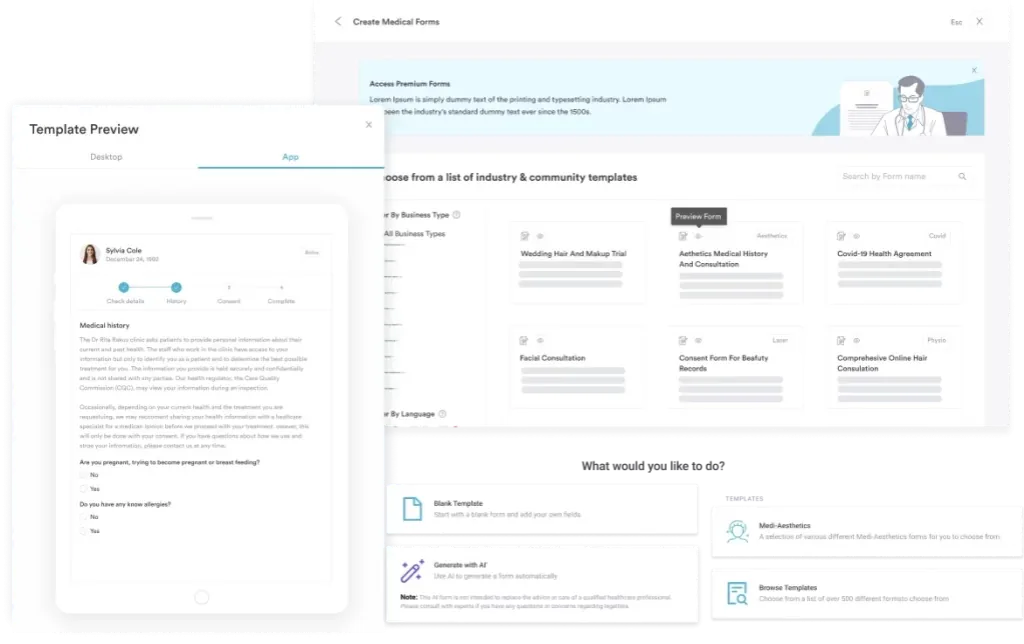
Teams that standardize medical forms and documentation workflows across their surgical practice report fewer audit findings and faster claim resolution cycles. Structured templating for operative reports is particularly valuable for high-complexity laparoscopic codes like 44227, where every element of the descriptor must be supported by the clinical record.
Create a procedure-specific documentation checklist for every CPT code your surgical team uses regularly, including 44227. The checklist should map each required documentation element directly to its corresponding code descriptor component: laparoscopic approach, enterostomy closure, resection performed, anastomosis technique. Attach it to your operative note template so surgeons capture all necessary elements before leaving the OR.
The National Correct Coding Initiative (NCCI) edits govern which procedure codes can and cannot be billed together. For CPT 44227, several bundling considerations affect surgical claims. Coders should verify current NCCI edit tables through the AMA CPT code set overview and CMS resources before submitting any combination involving 44227. Anesthesia is reported separately by the anesthesia provider under the site-specific 00100-01999 series, matched to the operative field, so an abdominal case draws a different code than the intraoral anesthesia billed with CPT code 00176.
Pre-authorization requirements for CPT 44227 vary by payer. Commercial insurers typically require pre-authorization for major inpatient surgical procedures. The documentation submitted for billing during the prior authorization process should match the code ultimately billed. A pre-authorization obtained for 44625 (open approach) does not cover 44227 (laparoscopic approach) if the payer treats these as distinct procedures.
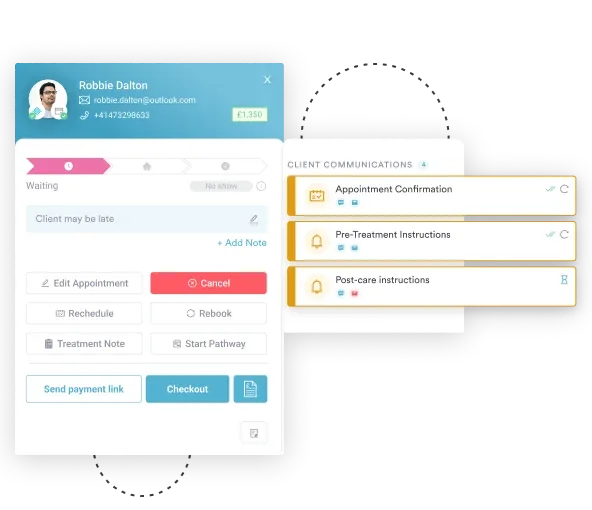
Using automated billing workflows that flag high-RVU codes for pre-authorization review before the procedure date can prevent claim denials that cannot be corrected after the service has been rendered.
General surgery and colorectal practices face heightened billing complexity when dealing with inpatient-only codes, 90-day global periods, and NCCI edit scrutiny. Pabau’s revenue cycle management tools help practices manage that complexity at the workflow level rather than catching errors only after denial.
Key capabilities relevant to CPT 44227 billing include structured operative documentation, modifier tracking, and pre-authorization workflow management. Practices using surgical practice management software that integrates clinical documentation with billing workflows report fewer modifier-related denials and faster reimbursement cycles for complex laparoscopic procedures.
CPT code 44227 is one of the highest-complexity laparoscopic intestinal codes in surgical billing, and its inpatient-only designation makes correct documentation and pre-submission review non-negotiable. The most common failure points are incomplete operative documentation, incorrect modifier application, and confusion with open-approach codes like 44625 and 44626.
Pabau’s claims management and digital documentation tools give surgical practices a structured way to capture, verify, and submit 44227 claims accurately. To see how Pabau handles high-complexity surgical billing documentation, book a demo with the team.
Managing billing across a multi-surgeon general surgery practice? Best EMR software for surgical specialties compares platforms for documentation-to-billing workflow integration.
Want to understand how claims management software reduces denials? Practice management for surgical teams explains how integrated billing workflows reduce high-RVU code denials.
CPT code 44227 is used to report a laparoscopic surgical closure of an enterostomy of the large or small intestine, with resection and anastomosis. It applies to laparoscopic stoma reversals including colostomy and ileostomy takedowns where bowel is resected and reconnected using a minimally invasive approach.
CPT 44227 is the laparoscopic approach to enterostomy closure with resection and anastomosis, while CPT 44620 is the open (non-laparoscopic) approach to enterostomy closure without resection. The key differences are surgical approach and whether bowel resection is included. Use 44227 when the procedure is laparoscopic and includes resection; use 44620 for open enterostomy closure without resection.
CPT 44227 covers laparoscopic enterostomy closure with resection and anastomosis, including laparoscopic Hartmann’s reversal. CPT 44626 covers open Hartmann’s reversal specifically, with coloproctostomy. When a Hartmann’s reversal is performed laparoscopically, 44227 is correct. When performed open with coloproctostomy, 44626 is correct. The 2023 NSQIP analysis used these codes specifically to separate laparoscopic from open Hartmann’s reversal cases.
Yes, CPT 44227 appears on the CMS Medicare Inpatient-Only (IPO) Procedure List under Addendum E. Medicare will not reimburse this procedure when performed in an outpatient hospital department or ambulatory surgery center. The IPO list is reviewed and updated annually, so coders should verify 44227’s current designation at the start of each calendar year.
Modifier 22 applies when the procedure is significantly more complex than typical, such as when dense adhesions substantially extend operative time. Modifier 51 applies when 44227 is performed alongside another distinct procedure in the same operative session. Modifier 59 (or X-modifiers) may apply when 44227 is billed with a code that would otherwise be bundled, but verify current NCCI edits before appending modifier 59 to any combination.
Whether CPT 44207 (laparoscopic colectomy with coloproctostomy) and CPT 44227 can be billed together with modifier 59 is not authoritatively confirmed. AAPC community discussions raised this question but no official NCCI ruling has been published. Practices should verify the current NCCI edit for this pair before submitting and document clearly why the two procedures were distinct if billing both.



