








HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
CPT Code 01502 covers anesthesia for procedures on arteries of the lower leg, including bypass graft and embolectomy, direct or with catheter.
The code carries 6 anesthesia base units, confirmed across VA Community Care, Massachusetts MassHealth, and Arizona ICA fee schedules.
Always append an anesthesia personnel modifier (AA, QK, QX, or QZ) – missing modifiers are the most common reason for claim denial on this code.
Pabau’s claims management software helps anesthesia practices track base units, time units, and modifier requirements across complex vascular billing workflows.
Most anesthesia claim denials for lower leg vascular procedures trace back to one root cause: the modifier was missing, the base unit count was wrong, or the ICD-10 pairing did not satisfy medical necessity. CPT Code 01502 sits in one of the higher-complexity families within the anesthesia section, covering arterial procedures below the knee where surgical risk and anesthesia time both run high. Getting the billing right requires understanding what the code actually covers, how reimbursement is calculated, and what documentation supports the claim.
This reference covers the official descriptor, base unit value, applicable modifiers, commonly paired ICD-10 diagnosis codes, and documentation requirements for specialty CPT anesthesia billing involving CPT Code 01502.
CPT Code 01502 has an official full descriptor of: Anesthesia for procedures on arteries of lower leg, including bypass graft; embolectomy, direct or with catheter. The code is published by the American Medical Association (AMA) as part of the Current Procedural Terminology code set and falls within the “Anesthesia for Procedures on the Lower Leg (Below Knee)” subsection, which begins at CPT 01500.
The code applies specifically when anesthesia is provided for an arterial embolectomy of the lower leg. An embolectomy is the surgical removal of a clot (embolus) blocking an artery. Surgeons may perform it via direct arterial incision or using a catheter technique, such as the Fogarty balloon catheter method. CPT 01502 captures both approaches and does not require separate codes to distinguish the technique.
The parent section heading “including bypass graft” indicates that 01502 is the correct code when anesthesia is provided for arterial bypass graft surgery on arteries of the lower leg, in addition to direct embolectomy procedures. The clinical setting is almost always a hospital operating room or a vascular surgery suite, with the surgical team typically including a vascular surgeon and an anesthesiologist or Certified Registered Nurse Anesthetist (CRNA).
| Code Element | Detail |
|---|---|
| CPT Code | 01502 |
| Full Descriptor | Anesthesia for procedures on arteries of lower leg, including bypass graft; embolectomy, direct or with catheter |
| Code Section | Anesthesia for Procedures on the Lower Leg (Below Knee) |
| Anesthesia Base Units | 6.0 |
| Procedure Type | Arterial: embolectomy (direct or catheter), arterial bypass graft |
| Setting | Operating room / vascular surgery suite |
| Provider Types | Anesthesiologist, CRNA |
Acute limb ischemia is the most common clinical context for this procedure. Peripheral artery disease (PAD) that progresses to acute occlusion, thrombotic or embolic events originating from cardiac sources, and failed vascular interventions can all result in the emergency or urgent arterial embolectomy that triggers a 01502 claim. The urgency of these cases often raises additional billing considerations, addressed in the modifiers section below.
CPT Code 01502 carries 6 anesthesia base units. Multiple independent fee schedules confirm this figure: the VA Community Care National Base Units table, Massachusetts MassHealth anesthesia service codes (effective August 2021), and the Arizona Industrial Commission (ICA) Physicians’ Fee Schedule (2020-2021). All three sources report 6.0 base units for 01502 without exception.
Providers calculate anesthesia reimbursement using the formula: (Base Units + Time Units + Qualifying Circumstance Units) x Conversion Factor = Reimbursement. Providers add time units for the actual duration of anesthesia service. Most payers, including Medicare, use 1 time unit per 15 minutes of anesthesia time, though some commercial payers use different intervals. Anesthesia start time begins when the anesthesiologist takes responsibility for the patient (typically at patient arrival in the operating room) and ends when the patient is safely transferred to postoperative care.
Using the Arizona ICA example: 6 base units x $61.00 conversion factor = $366.00 base reimbursement before time units are added. The final payment rises with the duration of the anesthesia service. For a 90-minute embolectomy, that adds 6 time units ($366.00 additional at the $61.00 conversion factor), bringing the total closer to $732.00 under that specific schedule. CMS publishes Medicare rates annually through the Physician Fee Schedule lookup tool, and rates vary by geographic area.
Anesthesia billing also involves tracking and documenting anesthesia start and stop times precisely, since any discrepancy between the operative note and the anesthesia record creates a denial risk. Practices using structured workflows around claims management software catch these timing gaps before submission rather than in an appeal cycle.
Review anesthesia start and stop times documented in the anesthesia record against the operating room log before submission. A 15-minute discrepancy costs one time unit and, at $61.00 per unit, that is a recoverable billing error that compounds across high-volume vascular practices.
Anesthesia codes require a personnel modifier on every claim. Without one, payers cannot determine whether an anesthesiologist personally administered the care, medically directed a CRNA, or supervised concurrent cases. This missing modifier is the most frequent denial trigger for CPT Code 01502 claims. The AAPC Codify CPT lookup provides guidance on which modifiers apply by provider type.
When an anesthesiologist and CRNA both provide services under a medical direction arrangement, the anesthesiologist appends QK and the CRNA appends QX. Providers submit both claims, and Medicare splits the reimbursement. The total combined payment equals what a single AA claim would produce, not double payment.
Qualifying circumstances (QC) are reported using additional CPT codes rather than letter modifiers. They recognize that certain patient or procedural conditions significantly increase the complexity of anesthesia. For lower leg embolectomy cases, the most relevant qualifying circumstances are emergency conditions and extreme age.
The medical record must clearly support any qualifying circumstance claimed. For 99140, the documentation should reflect the urgency of the embolectomy (limb-threatening ischemia, time-sensitive intervention) and reference to the emergency nature of the case in the anesthesia or surgical notes. Payer audits routinely flag qualifying circumstance codes without supporting documentation.
For vascular surgery practices using digital anesthesia intake forms and pre-procedure documentation tools, capturing qualifying circumstance information at the point of care reduces the post-claim documentation burden significantly.
Pabau helps vascular and surgical practices track CPT codes, modifiers, and documentation requirements in one place. See how it works for your practice.

Every anesthesia claim requires a supporting ICD-10-CM diagnosis code that establishes medical necessity. For CPT Code 01502, the diagnosis must reflect the vascular condition requiring the arterial procedure. Payers will deny claims where the diagnosis does not clinically support an embolectomy or arterial bypass procedure of the lower leg. Accurate ICD-10 diagnosis code documentation is a parallel requirement to the CPT billing itself.
| ICD-10-CM Code | Description | Relevance to 01502 |
|---|---|---|
| I74.3 | Embolism and thrombosis of arteries of lower extremities | Primary diagnosis for embolectomy cases |
| I74.4 | Embolism and thrombosis of arteries of lower extremity, unspecified | When specific artery laterality or type not specified |
| I70.209 | Unspecified atherosclerosis of native arteries of extremities, unspecified extremity | PAD as underlying cause, bypass graft context |
| I70.213 | Atherosclerosis of native arteries of extremities with intermittent claudication, bilateral legs | PAD with claudication requiring bypass |
| I70.234 | Atherosclerosis of native arteries of extremity with rest pain, bilateral legs | Critical limb ischemia, bypass indication |
| I70.262 | Atherosclerosis of native arteries of extremities with gangrene, left leg | Advanced PAD with tissue loss |
| I73.9 | Peripheral vascular disease, unspecified | Supporting diagnosis; may be insufficient as sole code |
| I82.4- | Acute embolism and thrombosis of deep veins of lower extremity | Venous thrombectomy (use 01522, not 01502) |
Coders should select the most specific ICD-10-CM code available. I74.3 is appropriate for acute arterial embolism requiring embolectomy. The I70.2xx codes are more appropriate when the underlying condition is chronic atherosclerosis requiring bypass graft surgery. Documenting laterality (left leg, right leg, bilateral) increases specificity and reduces audit exposure. For acute vascular condition coding, the primary diagnosis should reflect the acute presentation, not just the underlying chronic condition.
Payers will deny claims submitted with I82.4x codes (venous thrombosis) paired with 01502, because the code family covers arterial procedures. Venous thrombectomy of the lower leg maps to CPT 01522 (see related codes section below).
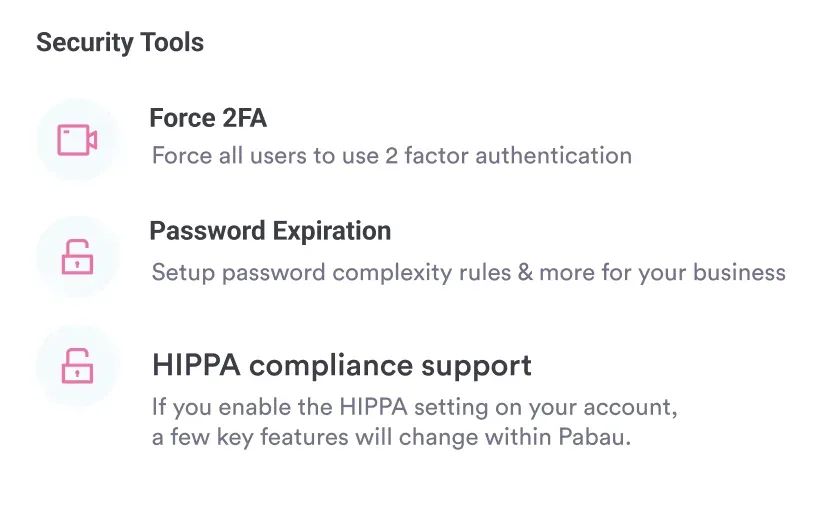
Anesthesia documentation must meet both payer requirements and HIPAA-compliant documentation practices for patient record integrity. The Centers for Medicare and Medicaid Services (CMS) requires specific elements in the anesthesia record to support payment for CPT Code 01502.
The ASA physical status classification is particularly important for CPT Code 01502 claims because many vascular embolectomy patients are ASA class III or IV (severe systemic disease or life-threatening condition). This classification supports the clinical complexity of the case and, where applicable, supports qualifying circumstance claims such as 99100 for extreme age. Structured clinical documentation embedded into the pre-procedure workflow reduces the risk that any required element is omitted under time pressure in emergency cases.
The National Correct Coding Initiative (NCCI) publishes procedure-to-procedure (PTP) edits that determine which codes can be billed together. For anesthesia codes, the primary bundling concern is that anesthesia services are global: the base units for 01502 already include pre- and post-anesthesia care for the procedure. Separately billing pre-anesthesia evaluation codes on the same date of service will typically trigger an NCCI edit denial.
Anesthesia practices should verify their billing compliance tools include current NCCI edit tables. CMS updates NCCI edits quarterly and periodically revises vascular anesthesia codes. A claim that passed edits in Q1 may fail in Q3 of the same year if an edit was added mid-year.
Flag all CPT Code 01502 claims for pre-submission review against the current NCCI edit table. Vascular anesthesia codes in the 01500-01522 family are frequently updated, and a single missed edit update can produce a string of denials before the issue is identified.
Understanding where CPT Code 01502 sits within the lower leg anesthesia code family helps coders select the correct code and avoid crossover errors. The codes below cover related procedures that anesthesia providers in vascular surgical settings regularly encounter. Reviewing surgical procedure anesthesia billing structures shows how these code families are structured across procedural specialties.
| CPT Code | Description | Base Units | Key Difference from 01502 |
|---|---|---|---|
| 01500 | Anesthesia for procedures on arteries of lower leg, including bypass graft; not otherwise specified | Not specified in reviewed schedules | General arterial procedures; 01502 is the specific embolectomy sub-code |
| 01502 | Anesthesia for procedures on arteries of lower leg, including bypass graft; embolectomy, direct or with catheter | 6.0 | This code |
| 01520 | Anesthesia for procedures on veins of lower leg; not otherwise specified | 3.0 | Venous (not arterial); lower complexity, fewer base units |
| 01522 | Anesthesia for procedures on veins of lower leg; venous thrombectomy, direct or with catheter | 5.0 | Venous thrombectomy counterpart to 01502; use when the vessel is venous, not arterial |
The most common coding error in this family is confusing 01502 (arterial embolectomy) with 01522 (venous thrombectomy). The operative report will specify whether the procedure involved an artery or a vein. Arterial procedures route to 01502; venous procedures route to 01522. The 3-unit difference in base values between 01520 and 01502 reflects the higher complexity and risk profile of arterial surgery versus general venous procedures.
CPT 01500 functions as the “not otherwise specified” catch-all for arterial lower leg procedures. When the procedure is specifically an embolectomy (direct or catheter-based), 01502 is the correct specific code and should always be preferred over 01500 to maximize appropriate reimbursement and support clinical documentation accuracy. Practices managing specialty CPT billing workflows across multiple code families benefit from systematic code selection checklists built into their billing process.
Vascular anesthesia billing is unforgiving of small errors. A missing personnel modifier, an imprecise anesthesia time record, or a mismatched ICD-10 code will result in a denial that costs more to appeal than the original claim is worth. CPT Code 01502, with its 6 base units and specific embolectomy descriptor, has a clearly defined billing pathway, but that pathway requires consistent documentation and modifier discipline at every claim.
Practices managing high volumes of vascular anesthesia claims benefit from anesthesia practice management tools that connect clinical documentation directly to the billing workflow, reducing the manual handoffs where errors accumulate. To see how Pabau supports claims workflows for surgical and vascular practices, book a demo.
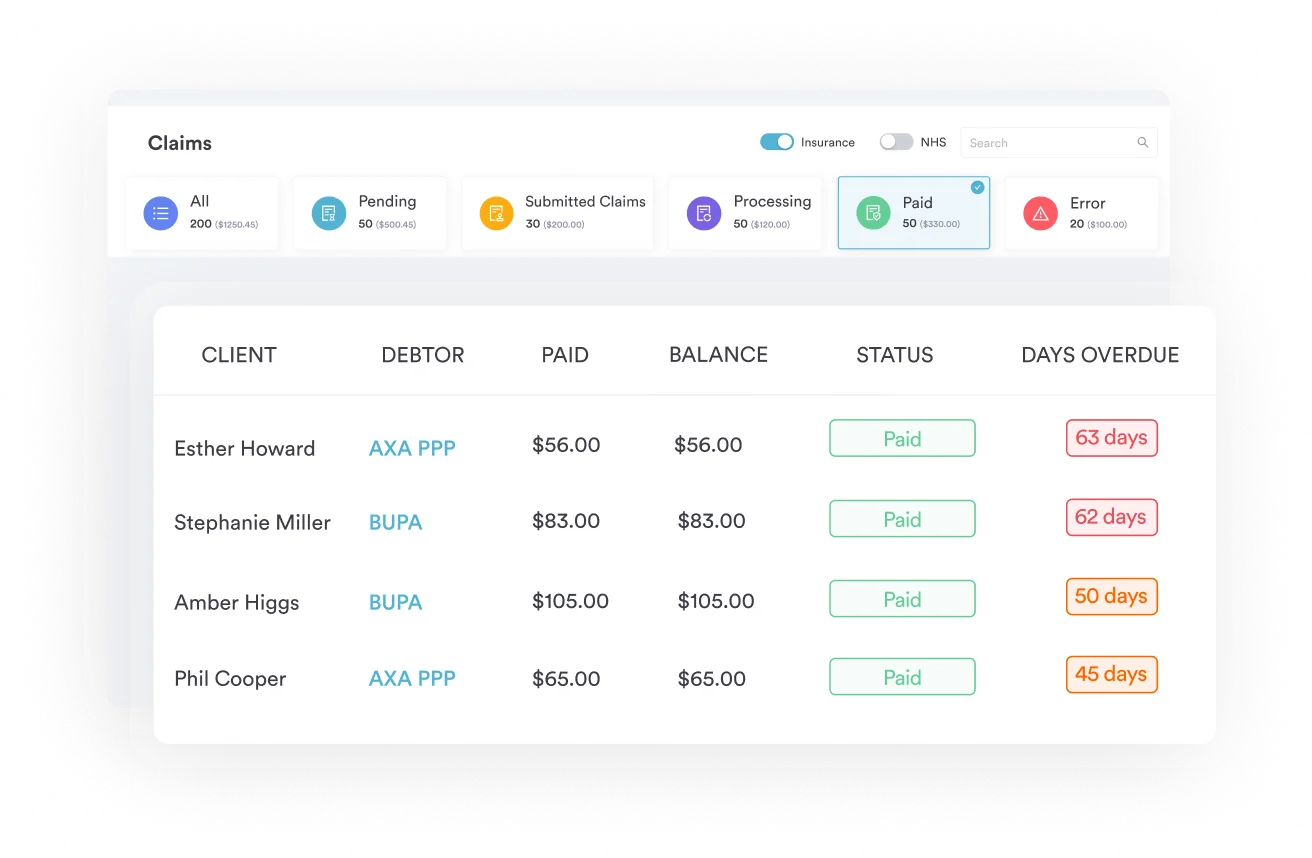
Need to manage complex vascular billing documentation? Claims management software provides end-to-end visibility across CPT codes, modifiers, and payer-specific rules.
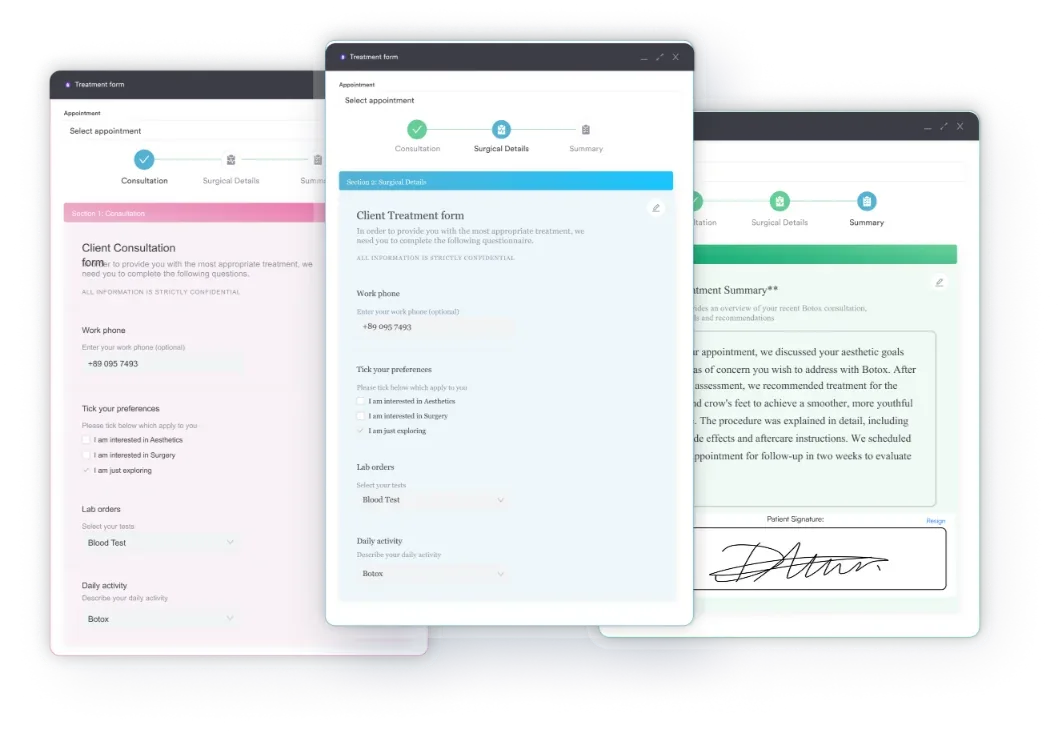
Looking for a structured pre-anesthesia documentation workflow? Medical forms for healthcare practices covers how digital intake and pre-procedure forms reduce documentation gaps.
Managing a surgical or plastic surgery practice? Plastic surgery EMR software outlines the practice management features most relevant to procedure-intensive specialties.
CPT Code 01502 is an anesthesia procedure code for embolectomy of the lower leg arteries, including bypass graft, performed directly or with a catheter. It carries 6 anesthesia base units and is published by the AMA as part of the Current Procedural Terminology code set.
CPT Code 01502 has 6 anesthesia base units, confirmed across multiple fee schedules including VA Community Care and Arizona ICA. Time units are added based on the duration of anesthesia service.
Use AA when an anesthesiologist personally performs the service, QK when medically directing two to four concurrent CRNA cases, QX for the CRNA under medical direction, or QZ for a CRNA without physician direction. A missing modifier is the most common denial trigger for this code.
CPT 01502 covers arterial embolectomy (6 base units); CPT 01522 covers venous thrombectomy (5 base units). The operative report determines which applies based on whether the vessel involved is an artery or a vein.
Yes. 99100 (extreme age) and 99140 (emergency conditions) are frequently applicable given the elderly patient population and urgent nature of many embolectomy cases. The medical record must contain supporting documentation.
I74.3 is the primary code for acute arterial embolism requiring embolectomy. I70.2xx codes apply when the underlying cause is atherosclerosis requiring bypass graft. Select the most specific code available and include laterality where possible.



