CPT Code 00802: Anesthesia for panniculectomy on the lower abdomen
Most anesthesia claim denials for panniculectomy procedures trace back to the sa...
Last Updated: July 28, 2026
HCPCS Code J1626 describes Injection, Granisetron Hydrochloride, 100 mcg—a 5-HT3 receptor antagonist antiemetic used to prevent chemotherapy-induced and postoperative nausea and vomiting.
Bill one unit of J1626 per 100 mcg administered; a standard 1 mg IV dose equals 10 units. Always verify the ordered dose before submitting units.
Medicare covers J1626 under Part B via the buy-and-bill model; prior authorization requirements vary by payer and plan—check each payer policy before administering.
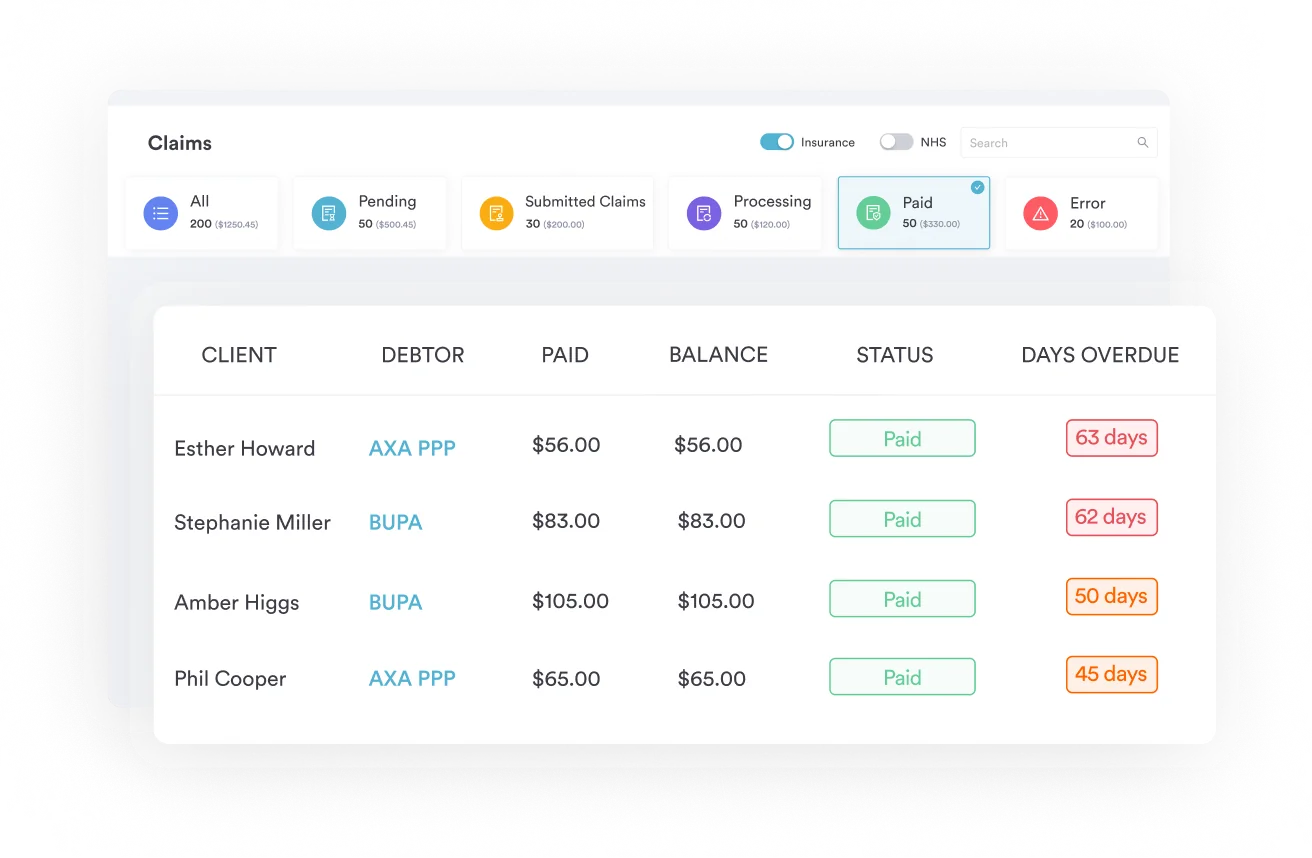
Pabau’s claims management software helps oncology and infusion practices automate J-code submission, track NDC crosswalk data, and reduce claim denials for injectable drugs like J1626.
The official descriptor for HCPCS Code J1626 is Injection, Granisetron Hydrochloride, 100 mcg. It was established by the CMS HCPCS National Panel and confirmed in CMS Transmittal R1055CP. The code falls under HCPCS Level II J-codes, the category reserved for drugs administered other than by the oral method — primarily injectable and infusible agents billed under Medicare Part B.
Granisetron hydrochloride is a 5-HT3 (serotonin) receptor antagonist. It works by blocking serotonin receptors in the gut and brain that trigger nausea and vomiting.
The NCI SEER CanMED oncology toolbox classifies J1626 under Major Drug Class: Antiemetic, Minor Drug Class: 5HT3 Receptor Antagonist, with FDA approval dating to 1993. The brand name Kytril is associated with granisetron hydrochloride injection, though generic formulations are also widely used.
J1626 covers granisetron hydrochloride given by injection in two principal clinical scenarios:
Note that granisetron also comes in a transdermal patch (Sancuso) and an extended-release injection (Sustol). These are distinct formulations with their own HCPCS codes and are not interchangeable with J1626.
Unit miscalculation is the leading source of J1626 claim errors, so confirm the count against the documented dose before every submission.
Each unit of HCPCS Code J1626 equals 100 mcg of granisetron hydrochloride. A typical adult IV dose for CINV prevention is 1 mg (1,000 mcg), which means you should bill 10 units of J1626 for that dose.
Always bill the actual dose administered, not the dose ordered or the dose in the vial. Verify the administered dose in the clinical notes before submitting.
| Dose Administered | Units to Bill (J1626) | Notes |
|---|---|---|
| 100 mcg | 1 unit | Minimum billable dose |
| 500 mcg | 5 units | Uncommon; verify order |
| 1 mg (1,000 mcg) | 10 units | Standard adult CINV prophylaxis dose |
| 2 mg (2,000 mcg) | 20 units | High-dose; ensure documentation supports medical necessity |
J1626 typically follows the buy-and-bill model under Medicare Part B. The practice purchases the drug directly from a wholesaler or specialty pharmacy, administers it to the patient, and then bills Medicare for the drug and the associated administration code (such as CPT 96374 for IV push).
Medicare reimburses the drug at ASP (average sales price) plus a percentage add-on. The statutory rate is ASP + 6%, though the effective rate is approximately ASP + 4.3% for most Part B claims because of sequestration. Rates depend on the quarterly ASP pricing file published by CMS.
Because ASP rates update quarterly, always check the current CMS ASP pricing file before finalizing your fee schedule. Reimbursement for J1626 is modest compared to newer antiemetics, but it remains widely covered and predictable. Practices using claims management software can track quarterly rate changes and update charge masters automatically rather than relying on manual lookups.
Coverage for J1626 is generally consistent, but it differs enough between payers to warrant checking each policy before administering.
Medicare Part B covers injectable antiemetic drugs, including J1626, when used in conjunction with cancer chemotherapy. The coverage determination rests on medical necessity: the drug must be administered to prevent nausea and vomiting associated with emetogenic chemotherapy. CINV prevention meets this bar routinely. PONV use may require stronger documentation, particularly if the patient is not a Medicare oncology beneficiary.
Medicaid coverage varies by state. Massachusetts MassHealth lists J1626 as payable without prior authorization at standard quantities in its Physician Provider Manual Subchapter 6. Note that the related code J1627 (granisetron extended-release injection) requires prior authorization above 200 units per 28 days under MassHealth, a separate rule from the one that applies to J1626.
State Medicaid fee schedules set their own allowable amounts, which may differ significantly from Medicare ASP rates. The Washington State Department of Corrections fee schedule, for example, lists J1626 with its own allowed amount distinct from federal Medicare rates. Always verify the applicable state Medicaid fee schedule rather than assuming Medicare rates apply.
Commercial payer requirements are inconsistent. Some payers require prior authorization for J1626, especially when it is administered in settings other than active chemotherapy. Harvard Pilgrim Health Care (HPHC), for example, lists J1626 on its chemotherapy prior authorization list per the OncoHealth HPHC Chemotherapy HCPCS J-Codes list.
Prior authorization policies change annually, so verify current requirements with each payer before the encounter. A documented pre-authorization workflow prevents most commercial coverage denials. See also the HCPCS Code S9379 and HCPCS Code S9542 home infusion therapy billing guides for infusion-specific payer requirements.
Check prior authorization requirements for every commercial payer at least once per quarter. Set a calendar reminder tied to your payer contract renewal dates. A denied claim for J1626 often traces back to a PA that expired or was never initiated for a new payer policy.
Documentation failures are the second leading cause of J1626 denials after unit errors. The clinical record must support both the medical necessity of the drug and the dose billed.
Per CMS HCPCS guidelines, every injectable drug claim must be supported by documentation that includes the drug name and dose, the route of administration, the date and time of administration, and the clinical indication.
For J1626 specifically, the chart must show that granisetron hydrochloride was ordered, prepared, and administered, not merely that an antiemetic was given. Vague documentation such as “antiemetic given pre-chemo” will not survive audit scrutiny.
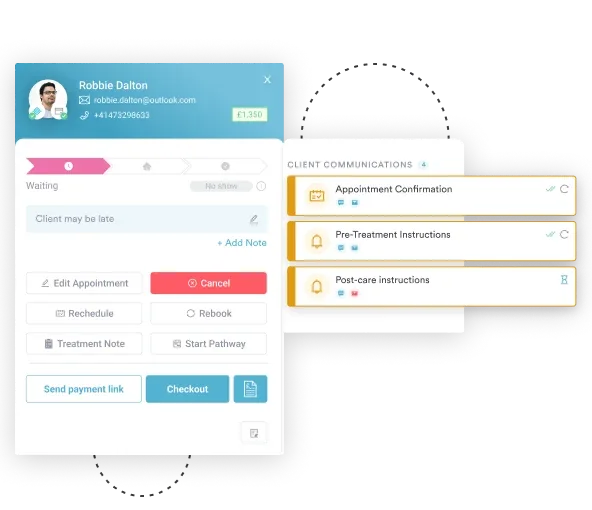
Maintaining HIPAA-compliant documentation practices means storing all drug administration records securely and ensuring audit trails are intact. Paper-based records are prone to missing entries — digital intake and consent forms combined with integrated clinical notes reduce the risk of missing documentation at claim submission.

Most Medicare and commercial payers require the National Drug Code (NDC) on J1626 claims. The NDC identifies the specific manufacturer, product, and package size of the granisetron hydrochloride vial used, appears on the drug label, and must be transcribed accurately onto the claim.
The HIPAA Space HCPCS-to-NDC crosswalk database is a commonly referenced tool for verifying NDC-to-J1626 mappings. Always confirm the NDC matches the vial used on the date of service.
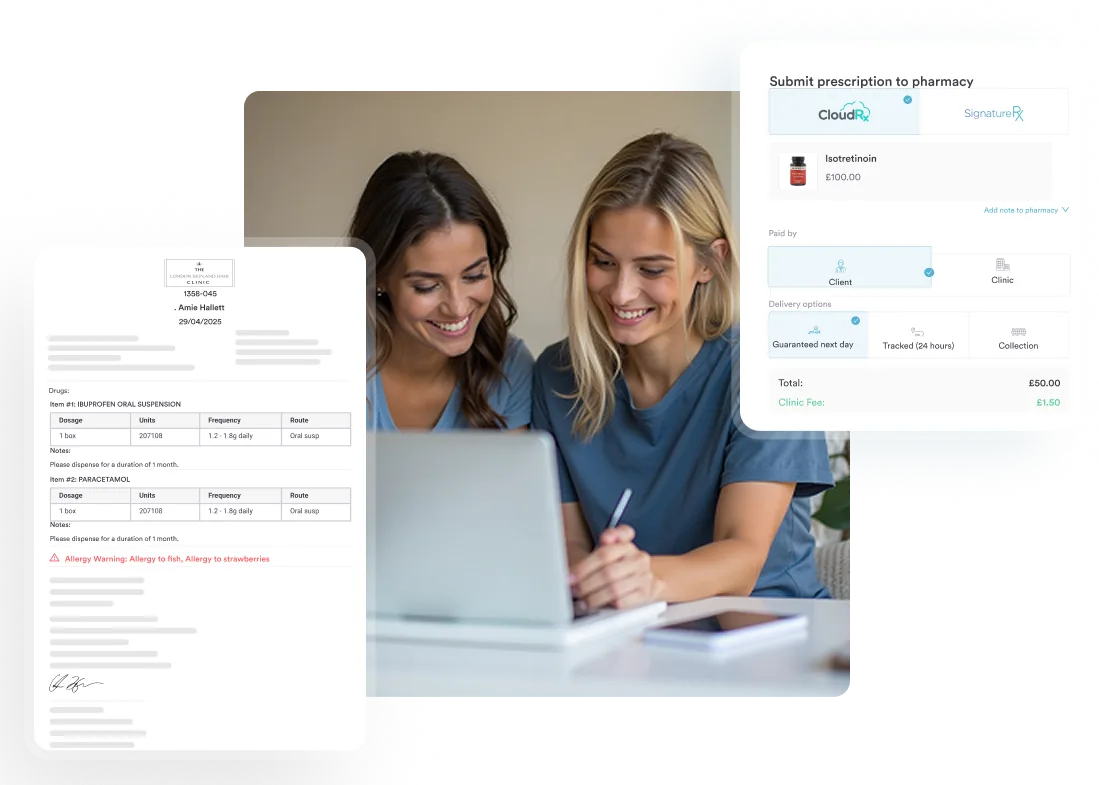
NDC formatting on claims typically follows the 11-digit format separated as 5-4-2. Incorrect NDC formatting (including wrong separator format) causes claim rejections at the clearinghouse level before the payer even reviews the claim. Using prescription management software with built-in NDC validation catches these formatting errors before submission.
Pabau's claims management tools help infusion and oncology practices automate J1626 billing, track NDC crosswalk data, apply correct modifiers, and catch unit errors before claims go out. Fewer denials. Faster reimbursement.

Modifier selection for J1626 depends on the drug’s source and the payer’s billing requirements. Using the wrong modifier—or omitting one when required—triggers immediate rejection or downcoding.
| Modifier | When to Use | Impact |
|---|---|---|
| JA | Drug administered intravenously (IV) | Required by many payers to indicate IV route; affects pricing under some fee schedules |
| JB | Drug administered subcutaneously (SQ) | Less common for granisetron; use only when route is SQ per physician order |
| GY | Item or service statutorily excluded or does not meet the definition of any Medicare benefit | Used when billing a non-covered indication to facilitate secondary payer billing |
| GX | Notice of liability issued—voluntary to the beneficiary | Paired with GY when patient has been notified of non-coverage; protects the practice |
The JA modifier is the most commonly required for J1626 given that granisetron hydrochloride injection is administered intravenously in CINV prevention protocols. Confirm your Medicare Administrative Contractor (MAC) requirements—some MACs require JA routinely on all injectable drug claims, while others require it only for specific drug categories.
Automated billing workflows can apply modifier rules by payer automatically, reducing manual assignment errors.
Build a modifier rule into your billing system for J1626 that prompts staff to confirm route of administration before claim submission. A claim submitted with JB (subcutaneous) when the drug was given IV creates a discrepancy between the clinical record and the claim—an audit red flag that is entirely preventable.
Oncology and infusion billing teams encounter predictable denial patterns with J1626. The fixes below address each at the source.
Proactive denial management starts with the charge capture workflow. Practices that review J1626 denial patterns monthly and correct root causes see materially lower denial rates within two to three billing cycles.
The HCPCS Code Q5121 infliximab-axxq billing guide covers comparable denial-prevention steps for other injectable biologics. A medical practice compliance checklist reviewed quarterly keeps documentation and billing processes aligned with current payer requirements.
For related injectable-drug billing workflows, see the HCPCS Code J3489 zoledronic acid injection guide and the HCPCS Code J0894 decitabine injection billing guide.
Understanding where J1626 sits within the antiemetic J-code landscape prevents miscoding and supports accurate crosswalk documentation. Refer to the CMS HCPCS code lookup to verify codes adjacent to J1626 in the J1620-J1631 range.
For other injectable oncology drug billing guides, see the HCPCS Code J9041 (bortezomib), HCPCS Code J9145 (daratumumab), and HCPCS Code J2329 (ublituximab) guides.
| HCPCS Code | Drug | Key Distinction from J1626 |
|---|---|---|
| J1626 | Granisetron hydrochloride injection, 100 mcg/unit | Standard IV/IM injectable formulation |
| J1627 | Granisetron extended-release injection, 0.1 mg/unit | Sustol formulation; different dosing interval and PA requirements under some Medicaid plans |
| J2550 | Promethazine HCl injection, up to 50 mg | Different drug class (phenothiazine); not interchangeable with 5-HT3 antagonists |
| J2405 | Ondansetron HCl injection, 1 mg/unit | Alternative 5-HT3 antagonist; more common in hospital outpatient settings |
| J1260 | Dolasetron mesylate injection, 10 mg/unit | Another 5-HT3 antagonist; less commonly used post-FDA IV restriction |
When a payer requests a crosswalk from a discontinued NDC to J1626 or between J1626 and J1627, document the crosswalk rationale in the patient record. Auditors look for internal consistency: the NDC billed must match the drug administered, and the HCPCS code must match the formulation.
Practices managing infusion drug inventories benefit from inventory management software that links drug lot numbers to patient administration records, making NDC crosswalk documentation automatic rather than manual.
Infusion and oncology practices carry a heavy medical billing burden: they administer multiple drugs per visit, each with its own J-code, unit count, NDC, and modifier requirements. Manual charge capture—often still recorded on a paper superbill—produces errors at rates that compound across hundreds of claims per month.
Pabau’s claims management software connects clinical documentation to claim creation, so the dose recorded in the patient’s drug administration record maps directly to the units billed on the claim. Modifier rules apply by payer. NDC fields pull from the inventory record.
The result is fewer unit errors and fewer missing-NDC denials without adding manual steps to the billing workflow. Practices using paperless clinical documentation report faster claim turnaround and cleaner audit trails compared to hybrid paper-and-digital processes. The HCPCS Code A9278 CGM receiver billing guide is a useful companion reference for practices billing other Part B drug-device codes.
For practices managing EMR software for infusion, integrating drug billing with patient scheduling and clinical notes in a single platform removes the hand-off points where J1626 billing errors typically originate.
HCPCS Code J1626 is a predictable code with predictable failure points: unit miscalculation, missing NDC numbers, wrong modifiers, and inadequate medical necessity documentation. Getting these four elements right on every claim eliminates the vast majority of J1626 denials before they happen.
Pabau’s integrated claims management connects drug administration records directly to claim creation, applying the correct unit counts, modifiers, and NDC data automatically. For infusion and oncology practices billing J-codes at volume, that connection can materially reduce denial rates compared to manual, disconnected processes. Book a demo to see how Pabau handles J-code billing end to end.
Running an IV therapy or infusion practice? IV therapy EMR software from Pabau covers drug administration records, billing integration, and compliance workflows for infusion practices.
Need a structured approach to injectable drug documentation? IV therapy intake form guidance walks through what pre-treatment documentation should capture for infusion encounters.
HCPCS Code J1626 represents Injection, Granisetron Hydrochloride, 100 mcg—a 5-HT3 receptor antagonist antiemetic used to prevent chemotherapy-induced and postoperative nausea and vomiting. The brand name Kytril is associated with this formulation, though generic granisetron HCl is also billed under J1626.
Bill one unit of J1626 per 100 mcg administered. A standard 1 mg (1,000 mcg) IV dose for CINV prevention equals 10 units. Always bill the actual dose administered as documented in the clinical record, not the vial size or ordered dose.
Yes, Medicare Part B covers J1626 when granisetron hydrochloride is administered as part of a cancer chemotherapy regimen. Coverage requires documentation of medical necessity linking the drug to an emetogenic chemotherapy protocol. PONV use in non-oncology patients may require stronger documentation to establish Part B eligibility.
Modifier JA (intravenous administration) is the most commonly required modifier for J1626 billing. Modifier JB applies when the drug is given subcutaneously. Modifiers GY and GX are used together when billing a non-covered indication and providing advance beneficiary notice to the patient.
Prior authorization requirements for J1626 vary by payer. Medicare Part B does not routinely require PA for antiemetics given with chemotherapy. Some commercial payers and managed care plans do require prior authorization—Harvard Pilgrim Health Care, for example, lists J1626 on its chemotherapy PA-required list. Verify the current PA policy for each payer before the encounter rather than assuming coverage.