CPT code 00103: Anesthesia for eyelid reconstruction billing guide
CPT code 00103 is the anesthesia code for reconstructive procedures on the eyeli...
July 23, 2026
CPT code 99223 describes high-complexity initial hospital inpatient or observation care, reported once per day by the admitting physician.
Since January 1, 2023, CPT code 99223 covers both inpatient AND observation care, eliminating separate observation-only codes.
Qualifying for 99223 requires either high-complexity MDM or a minimum of 75 minutes of total time on the date of the encounter.
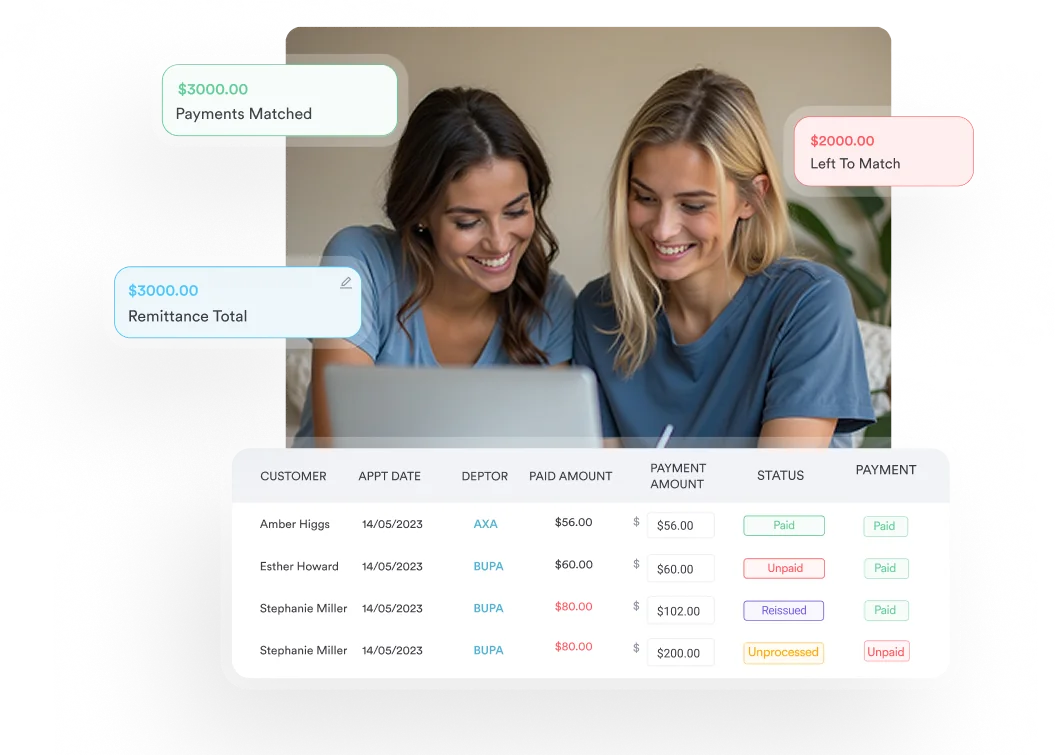
Pabau’s claims management software helps hospital-based practices document 99223 encounters accurately and reduce claim denials.
CPT code 99223 is the highest-complexity initial hospital inpatient or observation care code, reported once per day by the admitting physician for a patient requiring high-complexity medical decision making or at least 75 minutes of total time on the date of the encounter.
This reference covers CPT code 99223’s official description, the 2023 guideline changes that expanded its scope to include observation care, medical decision making (MDM) criteria, time thresholds, RVU values, reimbursement benchmarks, valid modifiers, and the compliance risks that lead to denials and audits.
CPT code 99223 describes initial hospital inpatient or observation care, per day, for the evaluation and management of a new or established patient, requiring high-complexity medical decision making or a minimum of 75 minutes of total time on the date of the encounter. According to the American Medical Association (AMA), which maintains the CPT code set, this code sits at the top of the initial hospital care family (99221-99223).
CPT code 99223 is used by the admitting physician for the first encounter with the patient during a hospital stay. Other physicians seeing the patient on the same day for the first time use different codes depending on their role and the payer.
| Code | Complexity | MDM Level | Minimum Time (total, date of encounter) |
|---|---|---|---|
| 99221 | Low | Straightforward or low | 40 minutes |
| 99222 | Moderate | Moderate | 55 minutes |
| 99223 | High | High | 75 minutes |
These are per diem codes. The Centers for Medicare and Medicaid Services (CMS) confirms that CPT codes 99221-99223 may be reported only once per day by the same physician or physicians of the same specialty from the same group practice.
Effective January 1, 2023, the AMA and CMS consolidated observation care and inpatient hospital care into a single code family. CPT code 99223 now covers both hospital inpatient and observation care for an initial encounter. This eliminated the previously separate initial observation codes (99218-99220), subsequent observation codes (99224-99226), and the observation discharge code (99217).
The practical impact is significant. A patient placed in observation status and a patient admitted as inpatient are now coded identically for the initial encounter. Transition from observation to inpatient status within the same stay does not constitute a new stay. According to the Medicare Claims Processing Manual (IOM 100-04, Chapter 12, Section 30.6.8.D), when a practitioner places a patient in observation and later converts to inpatient during the same stay, the practitioner does not report a second initial hospital visit code.
For practices managing hospital-based billing, staying current with these changes is part of routine HIPAA compliance for medical offices. Coding an encounter to the wrong code family after the 2023 changes is a common audit trigger.
High-complexity MDM is the clinical pathway most physicians use to qualify for CPT code 99223. The AMA defines high-complexity MDM across three elements, and the encounter must meet or exceed two of the three.
High complexity requires one or more of: a chronic illness with severe exacerbation or progression, a life-threatening condition requiring hospital-level management, or an acute illness or injury that poses a threat to life or bodily function.
Examples that commonly meet this threshold include sepsis, acute MI, stroke with new neurological deficits, severe CHF exacerbation, or multi-system trauma. A routine pneumonia admission in an otherwise healthy patient is unlikely to meet high-complexity criteria on problem complexity alone.
High complexity requires extensive data review. This means meeting three or more of the following within a single category, or meeting requirements across two of three data categories:
Documentation must be explicit. Writing “labs reviewed” does not meet the standard. The note must identify which labs were reviewed, what the results showed, and how they influenced the management decision.
High risk means one or more of: drug therapy requiring intensive monitoring for toxicity, decision for elective major surgery with identified patient or procedure risk factors, decision for emergency major surgery, diagnosis or treatment significantly limited by social determinants of health, or parenteral controlled substances.
A patient starting IV heparin for acute PE, or a patient requiring emergent surgical consultation for bowel obstruction, typically clears the high-risk threshold. Anticoagulation with close monitoring is a common documented risk element in initial hospital encounters billed with CPT code 99223.
Total time on the date of the encounter is an alternative pathway to the MDM route. For CPT code 99223, the minimum total time is 75 minutes. This includes all physician time on the date of the encounter, not just face-to-face time with the patient.
Activities that count toward total time include: preparing to see the patient, reviewing records and test results, obtaining and reviewing a history, performing the physical exam, ordering and reviewing tests, discussing the encounter with other providers, documenting the encounter in the medical record, and counseling and educating the patient or family.
Time that does NOT count: travel time, teaching unrelated to the encounter, time spent with other patients, and administrative work unrelated to this specific encounter.
When billing by time, the note must document the total time spent and confirm it occurred on the date of the encounter. A statement such as “Total time spent today on this encounter: 82 minutes” satisfies the documentation requirement. Practices using claims management software can flag encounters where time documentation is missing before submission, reducing the downstream denial rate.
Document total time as a discrete statement in the note, not buried in the narrative. Auditors look for an explicit time notation. A note that runs four pages but never states total time does not satisfy time-based billing criteria for CPT code 99223, even if the actual time clearly exceeded 75 minutes.
Relative Value Units (RVUs) are the foundation of Medicare reimbursement under the Resource-Based Relative Value Scale (RBRVS). CPT code 99223 carries one of the highest RVU totals in the initial hospital care family. The CMS Physician Fee Schedule publishes updated RVU values annually, and exact figures vary by geographic locality through the Geographic Practice Cost Index (GPCI) adjustment.
| RVU Component | Description | Relative Weight |
|---|---|---|
| Work RVU (wRVU) | Physician time, skill, and intensity | Highest component for 99223 |
| Practice Expense RVU (PE RVU) | Office overhead, staff, supplies | Facility vs. non-facility rates differ |
| Malpractice RVU (MP RVU) | Professional liability insurance cost | Smallest component |
For 2026, CPT code 99223 carries a work RVU of 3.86 and a total facility RVU of 4.68. At the 2026 Medicare conversion factor, that comes to a national payment of roughly $156 before geographic adjustment. Commercial payers often pay more, with reported rates ranging from about $260 to $390 depending on the state and contract.
A change specific to 2026 affects that math directly. CMS now publishes two conversion factors, so the same 4.68 total RVU pays slightly differently depending on the billing clinician:
Multiply the total RVU by your locality’s geographic adjustment and the applicable conversion factor to get the exact allowed amount for your MAC region.
For hospital inpatient services, the facility rate (Place of Service Code 21) applies, which uses the lower PE RVU compared to the non-facility rate. Commercial payers may reimburse above or below Medicare rates depending on contract terms. Practices managing both inpatient and outpatient billing benefit from keeping coding workflows organized through practice management software that separates facility and non-facility encounters automatically.
Pabau's claims management software helps hospital-based and inpatient billing teams document E/M encounters correctly, flag missing time notation, and track denial patterns before they become audit risks.

Place of service (POS) codes affect which RVU rate applies and whether the claim routes correctly. CPT code 99223 is reported under two POS codes depending on where the patient resides at the time of the encounter.
Modifier usage with CPT code 99223 is relatively limited but important in specific circumstances.
For practices with complex modifier workflows across multiple specialties, reviewing NCCI (National Correct Coding Initiative) edits before submission prevents bundling errors. Physicians who regularly admit patients from other care settings such as an IV therapy practice or outpatient setting should ensure their billing team understands when modifier AI applies. Practices managing those workflows can explore how IV therapy EMR software handles the transition documentation between sites of care.
Modifier AI (Principal Physician of Record) is a Medicare requirement, not optional documentation. Forgetting to append AI when the admitting physician bills 99223 can result in claim rejection or a request for refund if caught on audit. Build it into your billing team’s checklist for every initial inpatient claim.
Medicare eliminated consultation codes (99241-99255) in 2010. Consulting physicians seeing a Medicare patient in the hospital for the first time report the initial hospital care codes (99221-99223) based on the complexity of their encounter, not inpatient consult codes. The same MDM or time criteria apply.
According to Palmetto GBA MAC guidance, consulting physicians billing 99221-99223 for Medicare patients do not append modifier AI. Only the admitting physician appends AI. A cardiologist called for a consult on a patient admitted by a hospitalist bills 99221-99223 without AI, while the hospitalist who admitted the patient bills with AI.
Non-Medicare commercial payers may still use consultation codes. Verify each payer’s current policy before defaulting to the Medicare approach. Practices managing multi-specialty hospital billing can reduce coding errors with structured documentation workflows. The same principles apply whether billing for initial inpatient encounters or managing coaching CPT codes in outpatient settings: the code must match the documented complexity level.
CPT code 99223 carries higher financial value than 99221 or 99222, making it a frequent target for payer review and RAC audits. CMS has designated initial hospital care codes (99221-99223) as a projected high-improper-payment area, per WPS Government Health Administrators guidance.
The most common audit findings break into three categories: upcoding, missing documentation elements, and per-diem violations.
Billing 99223 when the documented encounter supports only moderate complexity (99222) is the most cited error. Auditors look for whether the documented problems, data reviewed, and risk elements actually meet the high-complexity threshold. A note that describes “stable chronic conditions” without documenting a severe exacerbation, extensive data review, or high-risk treatment does not support 99223.
Notes that describe clinical activity but don’t explicitly articulate MDM elements fail on audit. For time-based billing, the note must state total time numerically. “Spent significant time with patient” does not satisfy the requirement. Practices managing HIPAA-aligned documentation workflows should review their note templates against MDM criteria. A HIPAA compliance checklist for primary care can help identify documentation gaps that create audit exposure.
Reporting CPT code 99223 more than once per day, or reporting it after the initial encounter and then billing a second initial hospital code when the patient’s status changed from observation to inpatient, both constitute per-diem billing errors. The CMS RAC approved topic 0037 explicitly flags excessive units of initial hospital care codes as a monitored improper payment pattern.
Understanding where CPT code 99223 fits within adjacent code families prevents crosswalk errors and ensures correct code selection across the full hospital stay.
| Code(s) | Description | When to Use Instead |
|---|---|---|
| 99221-99222 | Initial hospital care, low/moderate complexity | When MDM or time does not meet high-complexity threshold |
| 99231-99233 | Subsequent hospital care | Days 2+ of the hospital stay (not the initial encounter) |
| 99234-99236 | Same-day hospital admit and discharge | Patient admitted and discharged on the same date of service |
| 99291-99292 | Critical care services | Patient requires critical care with constant physician attendance |
Selecting between 99223 and 99291 (critical care) depends on whether the patient’s condition requires constant attendance and whether the physician provided critical care as defined by CMS. A severely ill patient who requires high-complexity management but not constant attendance is appropriately billed with CPT code 99223, not critical care codes. The AAPC Codify CPT lookup provides official code descriptors and crosswalk data for the full E/M family.
Practices that manage both inpatient and outpatient workflows face documentation consistency problems across care settings. Pabau’s claims management software centralizes billing workflows, flags incomplete documentation before submission, and tracks denial patterns by code.
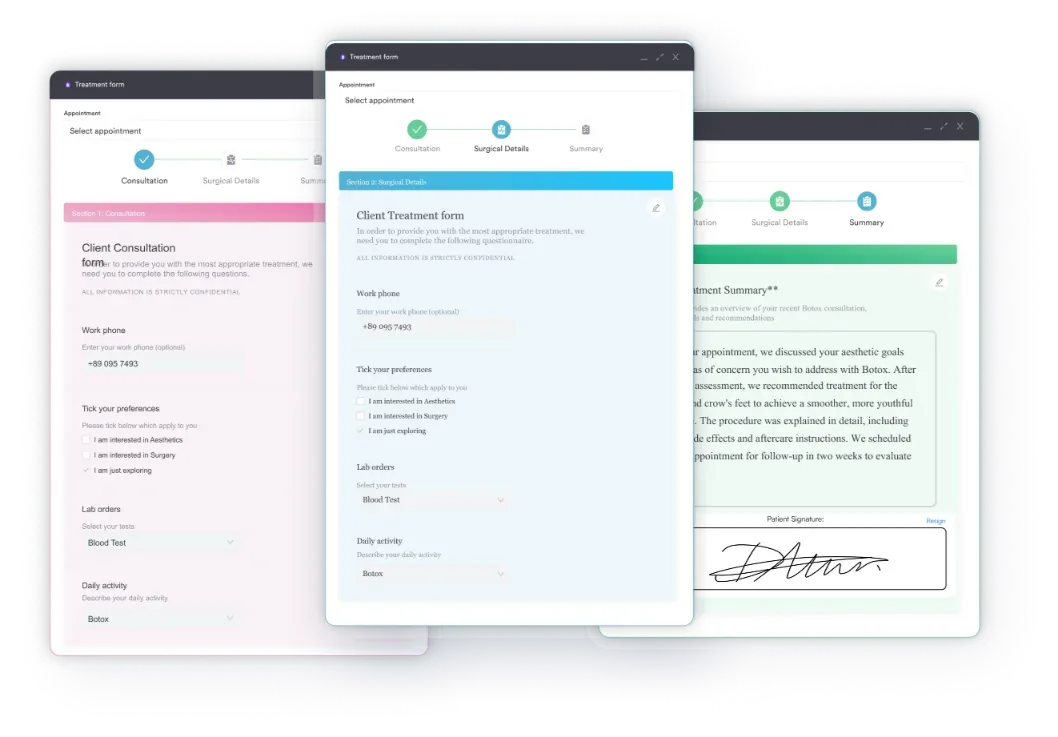
For practices managing initial hospital encounters alongside outpatient care, Pabau’s digital forms ensure that intake documentation captures the clinical complexity elements required for E/M code selection, reducing reliance on retrospective chart reviews during audits. Practices that see patients across multiple care settings can also leverage Pabau’s direct primary care EHR capabilities for non-facility encounters.
Consistent, structured documentation is the single most effective defense against 99223 claim denials. Good medical practice scheduling software connects appointment data to billing workflows, so the right POS code and modifier attach to the right encounter automatically.
CPT code 99223 is the most complex initial hospital care code, and the documentation requirements match its financial value. High-complexity MDM or 75 minutes of total time, clearly documented, is what separates a clean claim from a denial or audit finding.
Pabau’s claims management software helps practices build the documentation workflows that support correct E/M code selection from the point of encounter, not after a denial lands. To see how Pabau handles hospital-based billing documentation, book a demo with the team.
Need documentation templates for complex inpatient encounters? Safer clinical notes provides a practical framework for structuring hospital encounter notes that hold up to audit review.
Managing compliance across billing and care workflows? Med spa compliance outlines the documentation and billing compliance principles that apply across clinical settings.
Want to understand how AI tools support clinical documentation? Pabau’s AI medical scribe automates clinical note generation, reducing the documentation burden on physicians managing high-complexity inpatient encounters.
CPT code 99223 is used to bill for high-complexity initial hospital inpatient or observation care on the first day of a patient’s hospital encounter. It requires either high-complexity medical decision making or a minimum of 75 minutes of total physician time on the date of service. It is reported by the admitting physician or, for Medicare, by consulting physicians seeing the patient for the first time during the stay.
Yes. Since January 1, 2023, CPT code 99223 covers both hospital inpatient and observation care for the initial encounter. The 2023 E/M guideline changes eliminated separate observation-only codes, so a high-complexity initial observation encounter is now billed with 99223 under Place of Service 22.
The minimum total time for CPT code 99223 is 75 minutes on the date of the encounter. This includes all physician time associated with the encounter, not just face-to-face time. The note must explicitly state total time to support time-based billing.
All three describe initial hospital inpatient or observation care, but differ by complexity: 99221 requires straightforward or low-complexity MDM (or 40+ minutes total time), 99222 requires moderate-complexity MDM (or 55+ minutes), and CPT code 99223 requires high-complexity MDM (or 75+ minutes). Select the code that matches what is documented, not the clinical perception of how ill the patient appeared.
Modifier AI (Principal Physician of Record) is required by Medicare when the admitting physician bills CPT code 99223. Modifier 57 (Decision for Surgery) is appended when the encounter on the day of or day before a major surgery was when the surgical decision was made, protecting the E/M charge from bundling into the global surgical period.
CPT code 99223 is reported under Place of Service 21 (Inpatient Hospital) when the patient is formally admitted, and under Place of Service 22 (Outpatient Hospital/On Campus Observation) when the patient is in observation status. The facility PE RVU applies in both cases, which is lower than the non-facility rate.
For 2026, CPT code 99223 has a total facility RVU of 4.68, which comes to a national Medicare payment of approximately $156 before geographic adjustment, using the 2026 conversion factor of $33.40. The exact allowed amount varies by locality through the GPCI, and commercial payers often reimburse more.