








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT Code 95911 describes nerve conduction studies involving 9-10 individual motor or sensory nerves tested in a single session.
Each named nerve counts as one study regardless of how many sites are tested along that nerve, per CMS Article A56619.
Billing 95911 with EMG codes (95885, 95886) on the same day is generally permitted but may require Modifier 59 or XU depending on current NCCI edits.
Pabau’s claims management software and digital documentation tools help neurology practices capture the nerve-by-nerve detail needed for clean NCS claims.
CPT Code 95911 is the billing descriptor for nerve conduction studies (NCS) covering exactly 9-10 individual nerve studies performed in a single encounter. Electrodiagnostic testing at this scale is common in comprehensive neuromuscular evaluations where carpal tunnel syndrome, peripheral neuropathy, or radiculopathy is under investigation.
The American Medical Association (AMA) publishes CPT Code 95911 under the Neurology and Neuromuscular Procedures section. It sits within the NCS code ladder that runs from CPT 95907 (1-2 studies) through CPT 95913 (13 or more studies). Selecting the right code depends entirely on how many individual nerves were evaluated during the session.
The NCS code series uses a nerve-count threshold to determine which code applies. Each motor or sensory nerve tested counts as one study. The table below shows the full ladder relevant to most neurology billing workflows, from CPT 95907 at the low end up to CPT 95913 for studies of 13 or more nerves.
Work RVUs are approximate and based on published Medicare Physician Fee Schedule values, which CMS revalues periodically. Estimated Medicare payments also vary by geographic locality and the annual conversion factor. Confirm current rates with the CMS Physician Fee Schedule Look-Up Tool for your MAC jurisdiction.
The most costly billing mistake in NCS coding is miscounting studies. CMS Medicare Coverage Database Article A56619 is explicit: each code in the 95907-95913 series can be reimbursed only once per nerve, or named branch of a nerve, regardless of how many sites are tested along that nerve.
Testing the ulnar nerve at the wrist, forearm, below-elbow, above-elbow, axilla, and supraclavicular sites all counts as a single study. The nerve name determines the count, not the electrode placement count.
For a 9-10 nerve study justifying CPT Code 95911, document each nerve by name in the procedure report. Coders cannot reliably select the correct ladder code if the report lists “bilateral upper and lower extremity NCS” without naming the individual nerves tested.
Clean NCS claims start with the procedure report. Payers and Medicare audit contractors review this document when adjudicating CPT Code 95911. Missing or vague documentation is the primary driver of claim denials in electrodiagnostic billing. Practices using digital intake and documentation forms can build structured NCS report templates that capture the required fields at the point of care.
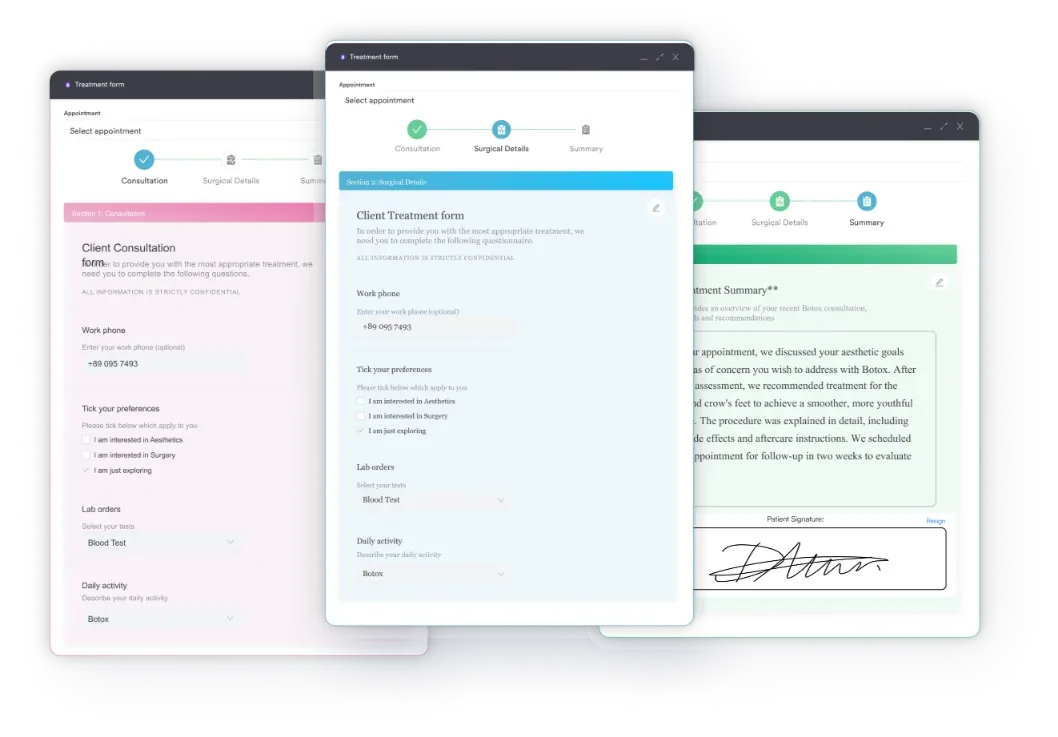
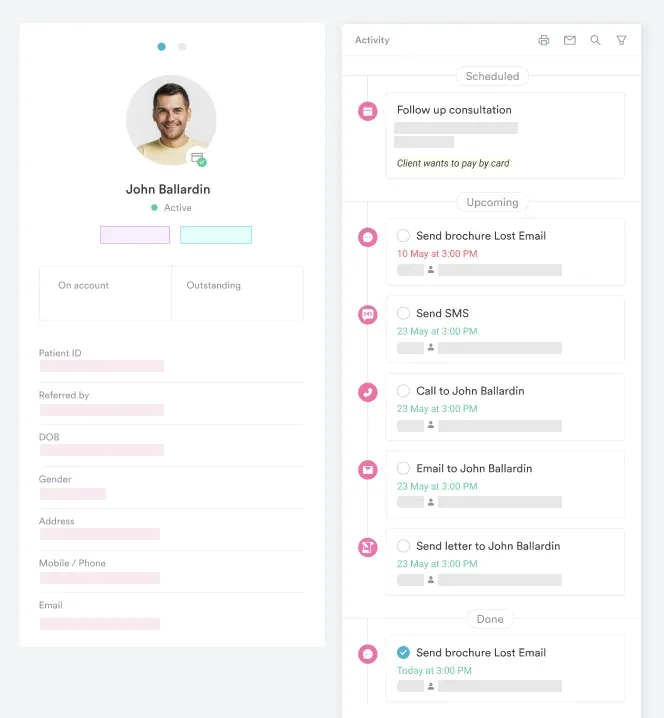
Maintaining structured patient records tied to each encounter makes retrospective audits far easier to defend. A single-page NCS summary that names all tested nerves, their parameters, and the interpreting clinician’s signature satisfies most payer and Medicare documentation standards. For the neurologic exam that supports the order, a cranial nerve examination checklist provides a ready-made structure.
Build a nerve-by-nerve NCS report template that forces staff to list each nerve separately before signing off. Auditors count named nerves to verify the CPT ladder code selected. A report that says ‘9 nerves tested’ without naming them creates unnecessary claim risk.
Medicare covers CPT Code 95911 when medical necessity is established through a supported ICD-10 diagnosis and the NCS is performed or directly supervised by the treating physician. Coverage is governed by Local Coverage Determinations (LCDs) issued by each Medicare Administrative Contractor (MAC). LCDs vary by jurisdiction, so always confirm coverage criteria with your specific MAC before relying on national estimates.
The work RVU for 95911 is 2.44, with a total RVU of approximately 6.59. Estimated Medicare payment falls around $220 per session, though this figure shifts with each year’s conversion factor and geographic locality adjustment. Verify current rates through the CMS Physician Fee Schedule search tool for your specific MAC region.
Medicare and commercial payers do not set a universal frequency limit for NCS in all clinical scenarios. Aetna, however, follows the American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM) maximum-study recommendations for electrodiagnostic (EDX) coverage determinations.
According to Aetna’s Clinical Policy Bulletin 0502, the number of NCS studies considered necessary is benchmarked against AANEM’s diagnostic-category guidelines.
State Medicaid programs can also impose their own frequency and documentation rules that differ from Medicare. Medi-Cal (California Medicaid), for example, applies coverage and provider conditions specific to electrodiagnostic testing that a national Medicare estimate won’t capture.
Always verify your state Medicaid program’s limits separately from Medicare LCDs. Practices with strong HIPAA-compliant documentation practices are better positioned to defend frequency-related audits.
Pabau helps neurology practices build structured NCS report templates, capture nerve-by-nerve documentation at the point of care, and manage claims workflows, so your team spends less time on rework and more time with patients.

Commercial payer rules for NCS billing diverge in ways that matter to neurology billing teams. Understanding three major payers illustrates the key differences to watch.
Aetna ties EDX coverage to AANEM’s maximum recommended study counts by diagnostic category. Submitting more studies than AANEM recommends for a given diagnosis increases denial risk, so the interpreting physician’s report must document which diagnostic category applies and why the study count is medically justified.
For CPT Code 95911, 9-10 studies is within the range Aetna considers appropriate for polyneuropathy evaluations, but it may exceed their threshold for isolated mononeuropathy workups.
Anthem’s Medical Policy CG-MED-24 addresses electromyography and nerve conduction studies. Anthem requires that NCS be medically necessary, performed by or under the direct supervision of a qualified physician, and supported by documented clinical indications.
The policy lists covered diagnoses and study types, so review the current version of CG-MED-24 through Anthem’s provider portal before submitting 95911 claims. Pairing NCS with the right diagnosis code, such as the ICD-10 code for lumbar disc disorder with radiculopathy, helps establish medical necessity.
Medi-Cal restricts billing of CPT codes 95907-95913 to credentialed providers only. The Medi-Cal Provider Manual specifies that these codes, along with 95924, 95940, 95941, and 95943, are reimbursable only to providers who have completed a neurology or physical medicine and rehabilitation (PM&R) residency, with a certification attestation attached to the claim.
Practices treating Medi-Cal patients should verify their credentialing status before billing the NCS ladder. Pairing each claim with a well-documented diagnosis, such as the ICD-10 code for type 2 diabetes with diabetic neuropathy, supports medical necessity and helps prevent avoidable denials.
NCS and EMG studies are frequently performed in the same session. Whether they can be billed together on the same date of service depends on current National Correct Coding Initiative (NCCI) edits, which CMS updates quarterly.
As of available guidance, CPT Code 95911 can generally be billed with EMG codes 95885 (limited EMG) and 95886 (complete EMG) on the same date, but Modifier 59 or XU may be required to indicate that the procedures are distinct services. Verify the current NCCI edit table before billing both codes together, as edit status changes.
The key distinction for bundling purposes is that NCS measures nerve signal transmission velocity and amplitude electrically, while EMG assesses muscle electrical activity with needle insertion. The two evaluate different physiological systems and are clinically complementary for a full electrodiagnostic workup.
Payers generally recognize this distinction, but documentation must clearly reflect that both services were separately indicated and performed. Coders can cross-reference the CCSD code for EMG and nerve conduction studies when mapping these services, and the same distinct-service scrutiny applies to other screenings, such as the ADHD screening CPT code.
Check the current NCCI edit table at CMS.gov each January when the annual update releases. Bundling rules for 95885, 95886, and the 95907-95913 NCS ladder can shift year to year. Using an outdated edit table is one of the easiest compliance errors to avoid.
Two modifiers come up consistently in NCS billing: Modifier 25 and Modifier 59.
When a physician performs both an evaluation and management (E/M) service (such as CPT 99205) and NCS on the same date, Modifier 25 should be appended to the E/M code to indicate a significant, separately identifiable service.
A Texas Department of Insurance medical fee dispute case (Case M4241188, January 2024) involved exactly this scenario: the billing of CPT 99205-25 alongside NCS codes including 95911. The requirement is generally accepted across payers, though some may deny or retract the E/M if Modifier 25 is missing.
Always append Modifier 25 to the E/M when a diagnostic procedure like NCS is billed on the same day. Use claims management software that supports modifier tracking at the claim level to reduce this type of denial.
Modifier 59 (or its more specific X-modifiers: XE, XS, XP, XU) is used when billing NCS and EMG together to indicate they are distinct services not typically reported together. When NCCI edits pair 95911 with an EMG code as a bundled edit, Modifier 59 or XU signals to the payer that the procedures qualify for separate payment under that encounter.
Use it only when clinically appropriate and when documentation supports two distinct, separately indicated services.
Denial patterns in NCS billing tend to cluster around the same root causes, and recognizing them before submission is more efficient than working denials after the fact. The AAPC Codify platform provides code-level guidance and crosswalk tools that neurology billing teams use to cross-check their coding decisions.
Practices that invest in neurology practice management software with built-in billing workflows can catch many of these errors before claims go out.
Most NCS billing denials trace back to two recurring issues: unclear procedure reports and nerve-counting errors. When the documentation names every nerve tested and the coder applies CMS Article A56619’s one-nerve-one-study rule, CPT Code 95911 claims go through cleanly.
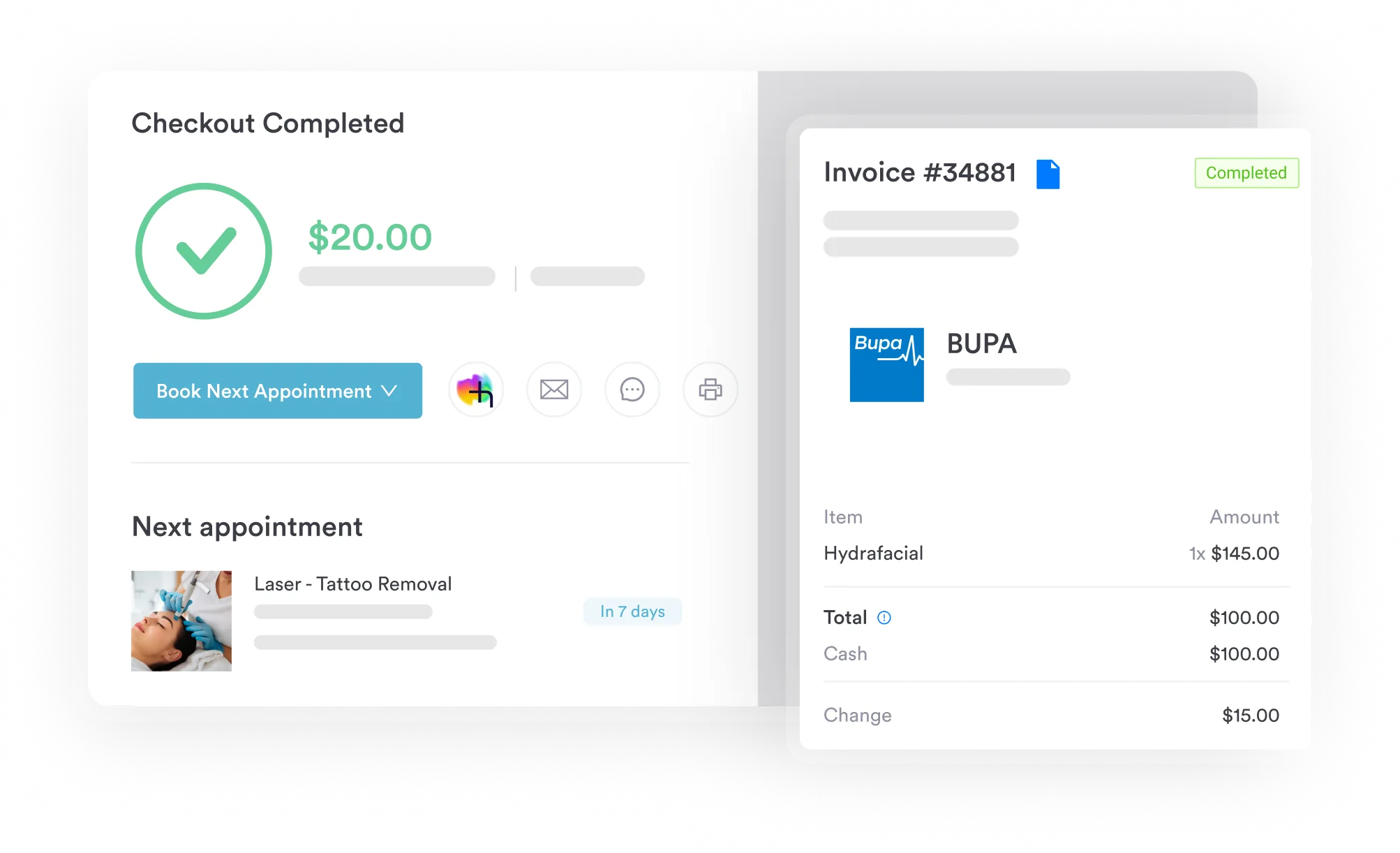
Pabau’s claims management tools give neurology practices structured workflows to attach procedure notes, track modifier requirements, and manage claim-level compliance before submission. Book a demo to see how Pabau handles neurology billing documentation end to end.
Testing more than 10 nerves? CPT Code 95913: nerve conduction studies, 13 or more covers the top rung of the NCS ladder and when to move up from 95911.
CPT Code 95911 is a nerve conduction studies descriptor covering exactly 9-10 individual motor or sensory nerve studies performed in a single session. It sits within the NCS code ladder (CPT 95907-95913), which scales by nerve count. Each named nerve tested counts as one study, regardless of how many recording sites are used on that nerve.
CPT 95911 covers 9-10 individual nerves. Per CMS Article A56619, a “nerve” means a named nerve or named branch of a nerve, not an electrode placement site. Testing the ulnar nerve at six different sites still counts as one nerve study.
CPT 95910 covers 7-8 nerve studies; CPT 95911 covers 9-10. The distinction is the nerve count documented in the procedure report. The work RVU increases from 1.95 (95910) to 2.44 (95911), so accurate counting directly affects reimbursement. Always select the code that matches the documented nerve count, not the estimate made before the study.
Generally yes, CPT 95911 can be billed with EMG codes (95885, 95886) on the same date of service, since NCS and EMG evaluate different physiological systems. However, current NCCI edits may require Modifier 59 or XU. Verify the active NCCI edit table from CMS before submitting both codes together, as bundling rules are updated quarterly.
The two most common modifiers are Modifier 25 (appended to a same-day E/M code to indicate a separately identifiable service) and Modifier 59 or XU (appended to 95911 or an EMG code when NCCI edits require separate identification). Modifier 25 goes on the E/M code, not on 95911 itself.
Count each named motor or sensory nerve as one study. Bilateral testing of the same nerve counts as two studies (one per side). F-waves and H-reflexes captured during the motor nerve study do not typically add to the count. Document each nerve by name in the procedure report before selecting the CPT ladder code.



