








CPT Code 10080: Pilonidal cyst I&D billing guide
CPT Code 10080 is the CPT code for incision and drainage of a pilonidal cyst, si...
July 24, 2026
CPT code 55700 (Biopsy, prostate; needle or punch, single or multiple, any approach) was deleted effective January 1, 2026, and must not be used for any date of service in 2026 or later.
Nine replacement codes (55707-55715) now differentiate prostate biopsy by approach, imaging guidance method, and whether the biopsy is systematic, targeted, or in-bore MRI/CT-guided.
Imaging guidance codes 76872 and 76942 can no longer be separately billed alongside any prostate biopsy code, as imaging is now bundled into the new code set.
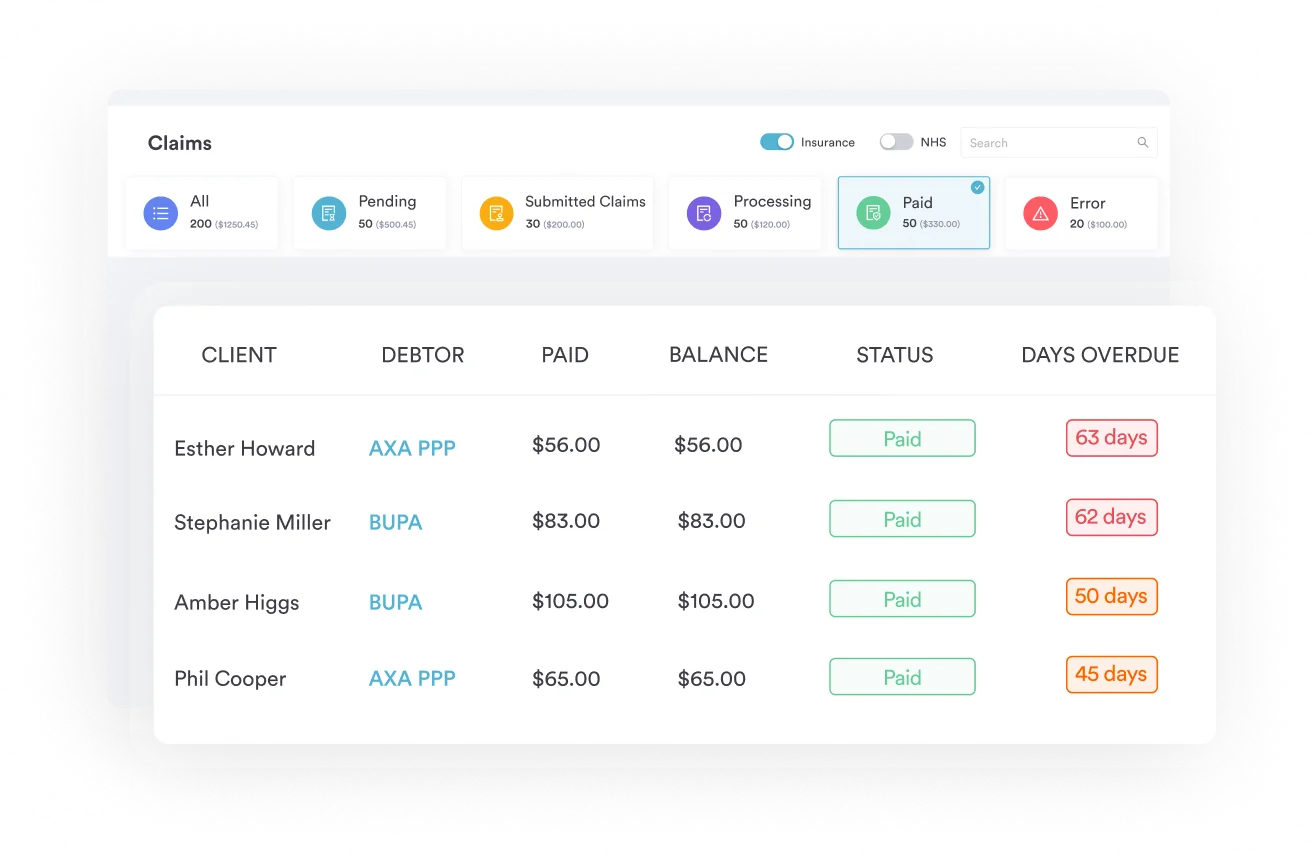
Pabau’s claims management software helps urology practices update code sets, manage payer crosswalks, and reduce denials during major CPT transitions like this one.
CPT code 55700 (Biopsy, prostate; needle or punch, single or multiple, any approach) was a prostate biopsy code deleted effective January 1, 2026. The American Medical Association replaced it with an expanded family of eleven codes (55705-55715) that sort prostate biopsy claims by approach, imaging guidance, and lesion targeting.
This guide covers the historical 55700 descriptor, the reason for its deletion, the full replacement family, and how to select the correct new code for each clinical scenario.
This reference is written for urologists, urology coders, and billing staff navigating the 2026 prostate biopsy code overhaul. It covers everything from the deleted 55700 descriptor to modifier guidance, imaging bundling rules, and denial prevention during the payer transition period.
CPT code 55700 carried a deceptively simple descriptor for decades: Biopsy, prostate; needle or punch, single or multiple, any approach. That “any approach” language was intentional. Transrectal, transperineal, ultrasound-guided, saturation, or fusion, a single code covered them all.
For high-volume urology practices, this was efficient. For payers trying to distinguish between a basic systematic biopsy and a precision in-bore MRI-targeted lesion biopsy, it was inadequate. The men’s health sector saw this change coming as MRI-guided fusion biopsy adoption accelerated throughout the early 2020s.
The AMA CPT Editorial Panel responded by expanding the prostate biopsy code family from three codes to eleven. The deletion of 55700 is, as the AAPC noted, the most impactful coding change in urology for 2026.
Under the old system, CPT code 55700 was used regardless of whether a urologist performed a 12-core transrectal ultrasound-guided systematic biopsy or a single-core in-bore MRI-targeted procedure, and regardless of whether the indication was an elevated PSA or suspected prostate cancer. Both were reported the same way. Imaging guidance, if used, was billed separately under CPT 76872 (transrectal ultrasound) or 76942 (ultrasound needle guidance). The approach was not documented in the code itself.
This limited the detail coders could capture. As prostate cancer diagnosis evolved toward multiparametric MRI (mpMRI) and fusion-guided targeted biopsy, coders had no mechanism to signal the complexity or resource intensity of the procedure at the claim level. The 55700 descriptor simply could not carry that information.
The AMA deleted CPT code 55700 to reflect two realities: the clinical landscape had changed, and reimbursement policy needed to catch up. MRI-guided fusion biopsy and in-bore MRI-targeted biopsy require different equipment, skill sets, and workflows than a standard transrectal ultrasound-guided biopsy. A single undifferentiated code could not support appropriate resource-based relative value.
The deletion also resolved the long-standing question of separately billing imaging guidance. By bundling ultrasound guidance and MRI guidance into the new codes, the AMA eliminated the separate reporting of 76872 and 76942 with any prostate biopsy service. This is a hard bundling rule: those two codes are not separately payable with any code in the 55705-55715 family, effective January 1, 2026.
Nine new codes (55707-55715) join the revised 55705 and the retained 55706 to replace CPT code 55700. Selection runs along three axes: approach (transrectal, transperineal, or in-bore), imaging method (none, ultrasound, MRI-ultrasound fusion, or in-bore CT/MRI), and biopsy type (systematic, targeted, or combined). Understanding all three is required before updating a charge master or order entry template. For reference on how other urology-adjacent code families are structured, our guide on IVF CPT codes illustrates a similar approach-based coding logic.
Retained and revised: CPT 55705 (non-image-guided biopsy, any approach) and CPT 55706 (saturation biopsy) are retained, with 55705 receiving a descriptor revision. The deletion of 55700 does not eliminate the entire pre-existing family. Verify current descriptors for 55705 and 55706 against your 2026 AAPC Codify CPT lookup before using them.
Selecting the right code from the 55705-55715 family requires three questions answered in sequence before billing any prostate biopsy in 2026. Urology coders who previously selected CPT code 55700 without documenting approach or imaging method now need that clinical detail captured in the operative report. Coding staff handling ADHD screening CPT codes or other procedure families face similar specificity upgrades when the AMA restructures a code family around clinical differentiation.
The per-lesion reporting rule for targeted biopsies is a significant billing change. Under the old CPT code 55700 system, a procedure targeting three suspicious MRI lesions was still one code. Under the new system, a transrectal MRI-fusion targeted biopsy of three lesions reports 55711 (first lesion) plus 55715 x2 (each additional lesion).
Document the approach, imaging modality, number of targeted lesions, and whether systematic cores were also taken in every prostate biopsy operative report. The new code set rewards documentation specificity. A report that says ‘TRUS-guided biopsy performed’ without naming the approach or whether fusion targeting was used will generate a coding query every time, delaying billing by days.
The biggest near-term risk is claim submission. Any claim for a prostate biopsy performed on or after January 1, 2026 that still uses CPT code 55700 will be denied. The code is invalid. Payers will not crosswalk it automatically. This is a hard edit, not a soft flag.
Use Pabau’s claims management software to audit any open claims from January 2026 onward for 55700 usage before they age into denials. The same workflow applies to any claim submitted in late 2025 for a date of service straddling the transition.
CPT 76872 (transrectal ultrasound) and CPT 76942 (ultrasound needle guidance) are now bundled into all prostate biopsy codes in the 55705-55715 family. Billing either code separately with any prostate biopsy will generate an NCCI edit denial. This applies to all payers following CMS National Correct Coding Initiative (NCCI) edits, which most commercial payers mirror with a short lag. Remove 76872 and 76942 from prostate biopsy order sets and charge capture templates immediately if you have not already done so.
Commercial payers do not always update their systems on January 1. Some may have interim crosswalk policies that map 55700 to a new code for a short period, while others may simply deny. Check each payer’s provider bulletin for prostate biopsy coding guidance. Review the CMS Physician Fee Schedule lookup for RVU values assigned to each new code in the 55707-55715 family, as reimbursement rates will vary by code and geographic region.
For practices using electronic health records, update order entry templates, diagnosis-to-procedure crosswalks, and superbill dropdowns before submitting any 2026 prostate biopsy claims. A charge master audit checklist helps confirm all retired codes have been replaced. Crosswalks should map indications such as a prostate cancer screening encounter to the correct new biopsy code so claims pass edits on the first submission.
Pabau's claims management and automated billing workflows help urology practices stay ahead of CPT code changes, reduce denials, and keep documentation audit-ready. See how it works for men's health and urology practices.

Several adjacent codes affect how prostate biopsy procedures are reported in 2026. Knowing which codes remain billable and which modifiers apply prevents additional denials beyond the 55700 deletion itself. For reference on how other procedure-specific code families use modifiers, our article on coaching CPT codes covers modifier logic in a different specialty context.
Modifier 50 (bilateral procedure) does not apply to prostate biopsy codes. Modifier 59 or XS may apply when distinct services are performed in the same session, but only when documentation clearly supports separate, distinct procedures. Use modifier 76 or 77 if a repeat procedure is required in the same session due to inadequate sampling, provided the operative report documents the clinical rationale. Add-on code 55715 is reported without a modifier; it is inherently a per-additional-lesion descriptor. Confirm current work, practice expense, and malpractice RVU values for each new code against the CMS Physician Fee Schedule before setting internal fee schedules.
Each new code has implicit documentation requirements that the old CPT code 55700 did not demand. At minimum, the operative report should capture:
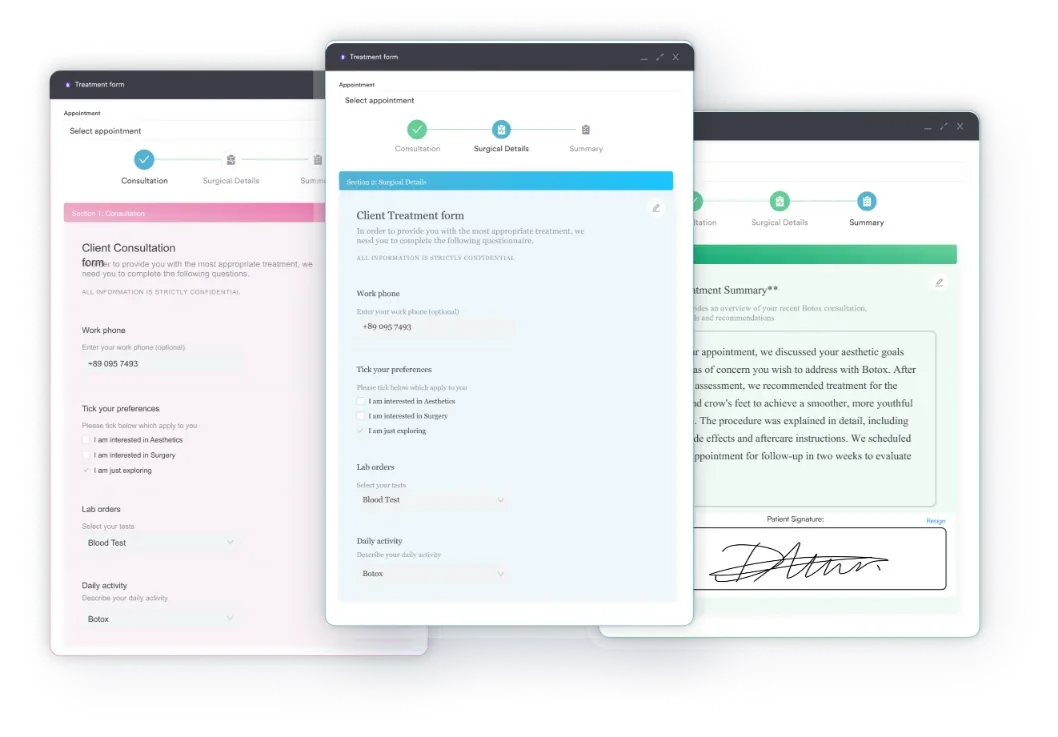
Practices using digital intake forms and structured clinical documentation can build these fields directly into procedure note templates, reducing coder queries at the point of billing rather than after the claim is filed.
Run a retroactive audit of all prostate biopsy claims submitted for January and February 2026 dates of service. Any claim that still carries CPT code 55700 should be corrected and resubmitted with the appropriate new code before the payer’s timely filing deadline. Do not wait for a denial letter.
CMS assigned new RVU values to the 55707-55715 code family for the 2026 Medicare Physician Fee Schedule. The values differ by code, reflecting the resource intensity of each approach and imaging method.
In-bore MRI-guided targeted biopsy (55714) carries higher RVUs than a standard TRUS-guided systematic biopsy (55707), consistent with the greater clinical complexity, suite time, and imaging infrastructure required. Verify exact dollar amounts using the CMS fee schedule tool, as payment rates vary by geographic practice cost index (GPCI) and are subject to annual adjustment.
Practices that routinely performed fusion-guided targeted biopsies under the old CPT code 55700 and billed 76872 or 76942 separately should model the net reimbursement impact carefully. The bundling of imaging guidance into the new codes means practices lose the separate payment for 76872 and 76942, but gain higher base RVUs for codes like 55708, 55711, and 55714.
Whether the net effect is revenue-neutral, positive, or negative depends on payer mix, payer-specific fee schedules, and the volume of targeted versus systematic procedures.
The deletion of CPT code 55700 marks the most significant urology coding change in more than a decade. The new 55707-55715 code family brings reimbursement policy in line with how prostate biopsy is actually performed: differentiated by approach, imaging guidance, and lesion-level targeting. For practices still submitting 55700 on 2026 claims, immediate correction is required.
Pabau’s automated billing workflows and claims management tools help urology practices update code templates, flag outdated CPT codes before submission, and stay audit-ready through major transitions. For guidance on broader HIPAA compliance for medical offices, Pabau also supports urology documentation workflows from intake through claim. Book a demo to see how Pabau handles prostate biopsy billing transitions and urology practice management end to end.
Need to review other urology-adjacent procedure codes? IVF CPT codes covers approach-based coding logic for reproductive procedures with similar documentation requirements.
Looking for a claims management tool built for specialty clinics? Pabau’s claims management software supports urology billing workflows, code template updates, and denial tracking.
Managing compliance documentation across your clinic? Safer clinical notes outlines documentation best practices that reduce audit risk across all procedure types.
CPT code 55700 was a prostate biopsy code described as “Biopsy, prostate; needle or punch, single or multiple, any approach.” It was used for all prostate needle biopsies regardless of whether the approach was transrectal or transperineal, and regardless of whether imaging guidance was used. The code was deleted effective January 1, 2026, and replaced by nine new codes (55707-55715) that differentiate by approach, imaging method, and lesion targeting.
CPT codes 55707 through 55715 replaced CPT code 55700 prostate biopsy effective January 1, 2026. The replacement codes separate prostate biopsy claims by approach (transrectal vs. transperineal), imaging guidance type (TRUS, MRI-fusion, in-bore MRI/CT), and biopsy category (systematic, targeted first lesion, or targeted additional lesion). The non-image-guided code 55705 was retained and revised, and 55706 (transperineal saturation biopsy) remains active.
No. CPT code 55700 was deleted effective January 1, 2026, and cannot be used for any date of service on or after that date. Claims submitted with 55700 for 2026 dates of service will be denied. Practices must use one of the new codes (55707-55715, or revised 55705) depending on the approach, imaging guidance, and biopsy type documented in the operative report.
No. CPT 76872 (transrectal ultrasound) and CPT 76942 (ultrasound needle guidance) are bundled into all new prostate biopsy codes in the 55705-55715 family and cannot be separately reported. Billing either code alongside any prostate biopsy code will generate an NCCI edit denial. Remove both codes from prostate biopsy charge capture templates immediately.
CPT 55707 is a transrectal, ultrasound-guided systematic biopsy: standard sextant sampling, with any ultrasound-visible lesion included, and no MRI fusion. CPT 55708 is a transrectal biopsy that combines systematic ultrasound-guided sampling with MRI-ultrasound fusion targeting of a suspicious lesion in the same session. If only a fusion-targeted lesion is sampled transrectally, with no systematic cores, report 55711 instead, and add 55715 for each additional targeted lesion.
CMS assigned distinct RVU values to each new code in the 55707-55715 family, with in-bore MRI-guided targeted biopsy (55714) carrying higher RVUs than standard TRUS-guided systematic biopsy (55707). Practices that previously billed 76872 or 76942 separately will lose that separate reimbursement, as imaging is now bundled. Net revenue impact varies by payer mix and procedure volume; verify current fee schedule amounts using the CMS Physician Fee Schedule lookup tool.



