








Blood pressure monitoring: A complete clinical guide
A clinical guide to blood pressure monitoring: home technique, reading categorie...
July 23, 2026
Medical practice operations covers every non-clinical function: scheduling, billing, staffing, compliance, and technology.
Claim denial rates average 5-10% of submitted revenue when front-office and billing workflows are misaligned, according to MGMA benchmarking data.
No-show rates above 8% are a leading indicator of scheduling system failure, not just patient behavior.
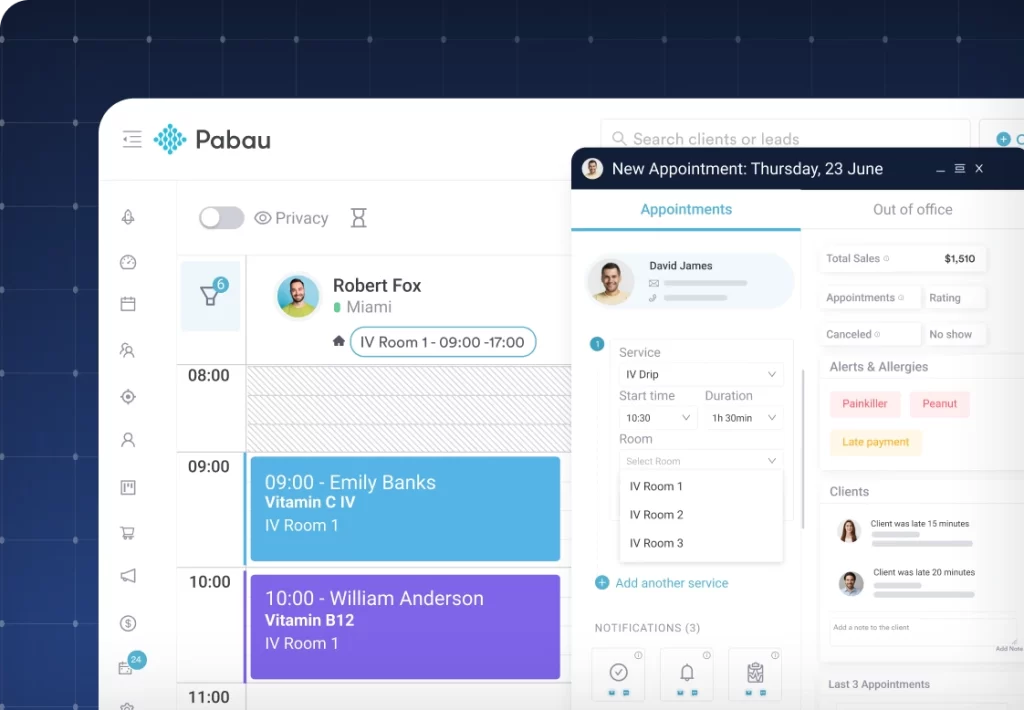
Pabau’s automated workflows and integrated scheduling reduce administrative overhead across all five core operational functions.
Most clinics lose revenue before a single claim is filed. The appointment gets booked, the patient arrives, the clinician delivers care, and then the system breaks down: a missing insurance verification, an unsigned consent form, a superbill entered three days late. According to the Medical Group Management Association (MGMA), practices that actively benchmark their medical practice operations recover measurably more revenue and sustain lower staff turnover than those running on reactive management alone. This guide covers the five functional pillars of medical practice operations, how each one drives financial performance, and where the highest-leverage improvements typically sit.
This guide is written for clinic owners, practice managers, and administrators who already understand healthcare delivery. The focus is on operational mechanics: what breaks, why it breaks, and how structured workflows prevent it. Whether you manage a solo physician practice or a multi-site group, the same five functions determine whether your operations scale or stall.
Physician practice operations form the backbone of how medical practices function, balancing patient care with administrative and financial responsibilities. Strip away the clinical work, and what remains are five interconnected systems: scheduling, front-office intake, revenue cycle, staffing, and compliance. Each one affects the others. A scheduling gap creates a revenue gap. A credentialing delay creates a compliance risk. Treating these as separate departments rather than a unified operational system is the most common structural mistake in practice management.
Patient flow starts long before the patient walks through the door. Appointment type, slot duration, provider availability, room turnover time, and insurance eligibility checks all feed into whether a scheduled visit actually generates revenue. A solo GP running 20-minute appointments needs different scheduling logic than a multi-practitioner dermatology clinic managing procedure rooms, consultation slots, and follow-up calls simultaneously.
No-show rate is the clearest signal of scheduling system health. MGMA data consistently shows that practices operating above an 8% no-show rate are losing two to three appointment slots per provider per day to preventable gaps. Automated appointment reminders, paired with a clear cancellation and deposit policy, cut that rate significantly. Pabau’s automated workflows handle reminder sequences, follow-up messages, and rebooking prompts without manual intervention from front-desk staff.
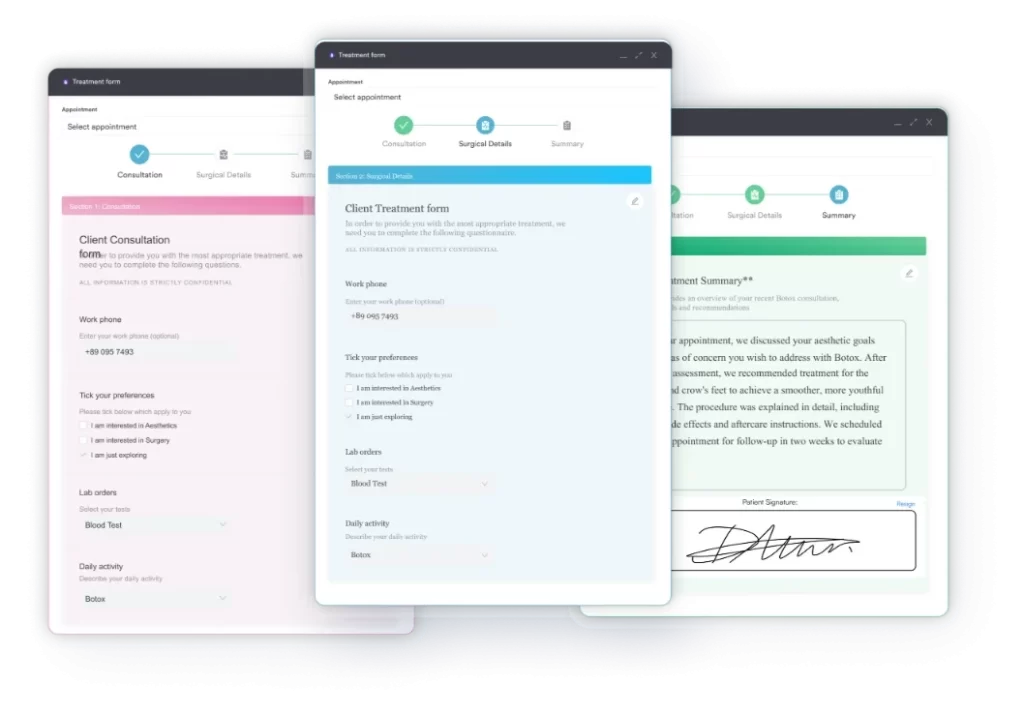
The front office is where medical practice operations either gain or lose momentum. Patient intake includes insurance verification, consent form collection, medical history capture, and identification of any pre-authorization requirements before the appointment begins. When any step is missing, the clinical team compensates by doing administrative work during appointment time, which compresses the schedule and degrades both care quality and throughput.
Digital intake workflows solve the most common bottleneck here. Digital forms sent to patients before their appointment collect history, consent, and insurance data in structured formats that feed directly into the patient record. This removes the front-desk data-entry step and reduces the rate of incomplete records reaching the clinician. A practice running 80 appointments per week can recover 4-6 staff hours per day by moving intake online.
| Operational Function | Primary Risk When Neglected | Key Performance Indicator |
|---|---|---|
| Scheduling | No-shows, revenue gaps, provider underutilization | No-show rate (target: under 8%) |
| Front-Office Intake | Incomplete records, delayed billing, compliance gaps | Intake completion rate pre-visit |
| Revenue Cycle Management | Claim denials, slow collections, cash flow strain | Days in AR, denial rate (target: under 5%) |
| Staffing and HR | Burnout, turnover, credentialing lapses | Staff retention rate, credential expiry tracking |
| Compliance | HIPAA violations, audit exposure, payer contract breaches | Policy review cadence, training completion rate |
Revenue cycle management (RCM) is the financial engine of every practice. It runs from insurance eligibility verification at the point of scheduling through claim submission, payment posting, denial management, and patient collections. Most practices treat RCM as a billing function. High-performing practices treat it as an operational discipline that touches every team member who interacts with a patient record.
Claim denials are the most expensive symptom of poor medical practice operations. The American Medical Association (AMA) reports that practices spend an average of $25 to rework each denied claim, and the administrative burden compounds when denial rates exceed 5% of submitted volume. The most common denial triggers are eligibility mismatches, missing modifiers, and late submission past payer windows, all of which are preventable with the right workflow controls upstream.
Claims management software integrates coding, submission, and denial tracking into a single view. Pabau’s claims management software connects clinical documentation to billing codes, reducing the manual coding step that introduces most submission errors. When a clinician completes a note, the billing-relevant data is already structured, not transcribed from handwritten notes after the fact.
Days in accounts receivable (AR) measures how long, on average, it takes a practice to collect payment after service delivery. MGMA benchmarks suggest that practices with efficient medical practice operations maintain days in AR below 35 for commercial payers. Practices above 50 days are typically experiencing one of three problems: slow claim submission, high denial rates requiring rework, or inadequate patient balance follow-up processes.
Each of these has a workflow fix. Slow submission is solved by same-day or next-day coding. High denial rates are solved by eligibility verification before the appointment, not after. Patient balance issues are solved by collecting copays and known patient responsibilities at check-in, supported by a clear payment policy that patients receive and acknowledge during intake.
From automated intake and digital consent forms to integrated billing workflows and recall automation, Pabau connects every operational function in one platform. Book a demo to see it in your workflow context.

Staff structure is the operational variable most practices underestimate when planning capacity. A practice with 2 physicians, 1 nurse, and 2 front-desk staff has a fundamentally different operational ceiling than a practice with the same physician count and 4 support staff. The ratio determines scheduling throughput, documentation speed, patient communication capacity, and the time available for billing follow-up.
Staff credentialing is one of the highest-risk areas in medical practice operations. A lapsed license, an expired DEA registration, or a missed payer credentialing renewal can suspend billing for an individual provider, cutting revenue from that provider’s patient panel until the credential is reinstated. The MGMA recommends tracking all expiry dates in a centralized system with automated alerts at 90 and 30 days before expiration.
Beyond credentialing, role clarity reduces the administrative burden that leads to staff burnout. Ambiguity about who handles prior authorizations, who manages patient callbacks, and who owns the billing queue creates duplication and gaps. Pabau’s team management software lets practice managers assign tasks, track completion, and set role-based access so each staff member sees exactly what they need and nothing they don’t.
Compliance in medical practice operations goes beyond annual training checkboxes. Under HIPAA (the Health Insurance Portability and Accountability Act), practices are required to maintain documented policies for patient data access, transmission, and breach response. CMS (Centers for Medicare and Medicaid Services) adds billing compliance requirements that include medical necessity documentation and proper use of modifiers. Failing either set of requirements carries financial and operational penalties that can destabilize a practice far more than a bad revenue month.
The practical compliance framework for most practices includes three layers: written policies, staff training with documented completion, and technology controls that enforce the policies automatically. The third layer is where most practices are weakest. A compliance management system that enforces access controls, audit logs, and consent workflows removes the dependency on staff remembering to follow procedures manually.
Audit your practice’s credentialing expiry dates quarterly, not annually. Create a spreadsheet or use your practice management platform to track license renewals, DEA registrations, and payer credentialing windows for every provider. One lapsed credential can freeze billing for a full patient panel until reinstatement is processed.
Practice management software has moved from optional infrastructure to operational necessity. The question is no longer whether to use it, but which functions it needs to unify. Fragmented systems, where scheduling lives in one platform, billing in another, and clinical notes in a third, create the same information gaps that manual workflows do. Every handoff between systems is a point where data can be lost, duplicated, or delayed.
Electronic Health Records (EHR) and Electronic Medical Records (EMR) are the documentation layer that connects clinical care to operational outcomes. A well-configured EHR reduces documentation time per visit, structures data in ways that support accurate coding, and creates an auditable record of every clinical decision. The ONC (Office of the National Coordinator for Health Information Technology) tracks EHR adoption and usability as part of broader interoperability initiatives that affect how practices share data with hospitals, labs, and payers.
AI-assisted documentation is reducing the time clinicians spend on notes after appointments. Pabau’s Pabau Scribe generates structured clinical notes from consultation dictation, cutting post-appointment documentation time and reducing the risk of incomplete records that trigger billing denials or compliance gaps. For practices where provider time is the primary bottleneck, documentation automation directly increases daily patient capacity. The mechanics behind that gain are covered in our guide to AI clinical documentation software, from speaker separation to EHR integration.
You cannot improve medical practice operations you cannot measure. The core operational KPIs every practice should track are: appointment utilization rate, no-show rate, days in AR, denial rate by payer, patient satisfaction scores, and staff productivity ratios. MGMA’s benchmarking tools let practices compare their metrics against peer groups by specialty, size, and geography, which is far more actionable than tracking absolute numbers in isolation.
Integrated reporting connects scheduling data, financial data, and clinical data in a single dashboard. Pabau’s reporting and analytics tools surface operational metrics across all locations, showing which providers have the highest utilization, which appointment types generate the most revenue per slot, and where no-show patterns cluster by day, time, or patient demographic. Decisions made from this data replace the guesswork that often drives operational changes in under-resourced practices.
Telehealth has added a new operational layer that many practices are still integrating. The CMS telehealth coverage guidelines govern reimbursement eligibility for virtual visits under Medicare, and the requirements vary by service type, patient location, and originating site. Practices that added telehealth during the pandemic without building proper billing workflows for it are often discovering retroactive reimbursement gaps when they conduct AR reviews. Telehealth needs the same intake, consent, and billing discipline as in-person care, delivered through a platform that supports telehealth workflows natively.
Need a structured framework for practice management software selection? Best Medical Practice Management Software evaluates the leading platforms by operational function coverage, pricing, and specialty fit.
Want to benchmark your revenue cycle performance? Practice Management Software Guide covers RCM workflows, claim management features, and integration requirements for high-volume practices.
Looking to reduce no-shows and improve scheduling efficiency? How to Improve Patient No-Show Rate provides a step-by-step breakdown of reminder workflows, deposit policies, and waitlist strategies.
Running a multi-site practice and need operational consistency across locations? Pabau Multi-Location Management centralizes scheduling, billing, and reporting across all sites with role-based access per location.
The gap between a practice that runs smoothly and one that doesn’t is rarely clinical. It’s operational: misaligned scheduling, reactive billing, manual compliance tracking, and fragmented technology. Fixing medical practice operations means building systems where each function supports the next, rather than compensating for gaps elsewhere.
Pabau’s all-in-one practice management platform unifies every operational layer, from digital intake and automated recall to claims management and AI-assisted documentation, into a single workflow system. The same logic explains the reasons clinics choose Pabau instead of stitching together separate tools. Book a demo to see how Pabau handles the operational functions your team currently manages manually.
Physician practice management covers five core functions: scheduling and patient flow, front-office intake, revenue cycle management, staffing and credentialing, and compliance. Each function has measurable KPIs, and MGMA publishes annual benchmarks that let practices compare performance against specialty-specific peer groups.
A practice operations manager oversees day-to-day functions from the front desk through the revenue cycle, including staff scheduling, billing oversight, compliance monitoring, and vendor management. In larger group practices, the role often splits into front-office and back-office tracks with separate team leads reporting to a central operations director.
Start by measuring the five core KPIs: no-show rate, days in AR, denial rate, intake completion rate, and staff-to-provider ratio. Most practices find their biggest inefficiency in one of two places: pre-visit intake (missing information that delays billing) or post-visit documentation (slow coding that delays claims). Automating both with practice management software typically recovers 3-6 hours of staff time per day in a 3-provider practice.
Clinical operations covers everything delivered by licensed practitioners: diagnosis, treatment, prescribing, and care planning. Non-clinical operations covers everything that supports care delivery: scheduling, billing, compliance, facilities, staffing, and technology. Both are required for a practice to function, but only non-clinical operations can be fully systematized and automated without clinical judgment.



