








HCPCS Code J3360: Diazepam injection billing guide
HCPCS Code J3360: Definition, description, and code details HCPCS Code J3360 is ...
Last Updated: July 28, 2026
CPT code 92551 describes a screening test, pure tone, air only – it detects possible hearing loss but does not determine hearing thresholds.
Medicare does not cover CPT 92551 for routine hearing screening; Medicaid EPSDT programs and commercial insurers may cover it with appropriate diagnosis codes.
Never use 92551 for newborns or infants – OAE or ABR codes apply; calibrated electronic equipment is required for any 92551 claim.
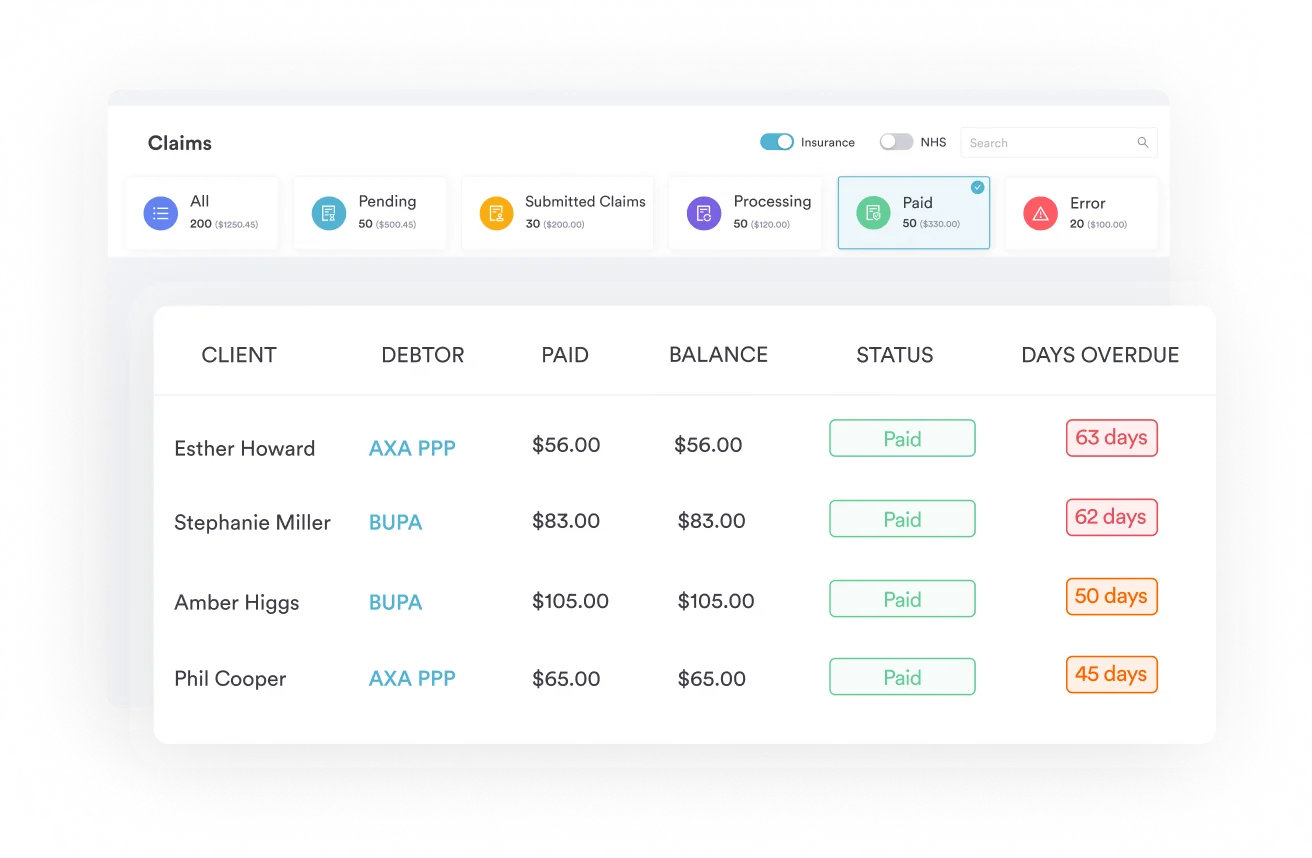
Pabau’s claims management software supports audiology billing workflows, reducing claim errors and speeding reimbursement.
CPT code 92551 is a screening test for pure tone, air conduction hearing only. It presents tones at a fixed intensity (typically 20-25 dB HL) across several frequencies to flag possible hearing loss on a pass/fail basis. It does not measure exact hearing thresholds, which requires diagnostic code 92552.
Practices billing audiology services get 92551 wrong more often than almost any other hearing code. The most common error: Using it when a diagnostic threshold test was actually performed, or billing it for newborns it was never designed to cover. According to the American Medical Association’s CPT code set, CPT code 92551 has a precise descriptor: “Screening test, pure tone, air only.” That precision matters for every claim you submit.
Pure tone audiometry uses calibrated electronic equipment to transmit tones of varying pitches and intensities through headphones placed on the patient. The patient signals each time they hear a tone. CPT code 92551 covers only the air conduction portion of that test. It does not include bone conduction testing, and it does not determine the faintest sound a patient can reliably detect (hearing threshold). If the patient fails the screen, further evaluation is needed using a separate code.
This distinction between screening and threshold testing is the most important concept in this article. Getting it wrong exposes a practice to claim denials, downcoding, and in audit scenarios, potential fraud allegations. The sections below cover everything coders, audiologists, ENTs, and primary care practices need to bill 92551 correctly, including documentation requirements for medical forms at your practice, modifiers, Medicare coverage rules, and the adjacent codes you will reach for when 92551 does not apply.
CPT 92551 covers a pass/fail hearing screen using pure tone air conduction. A technician or clinician places headphones on the patient and presents tones at a fixed intensity (typically 20-25 dB HL) across a range of frequencies. The patient either responds or does not. That is the entire scope of the test.
Three things are explicitly not included:
The American Academy of Pediatrics coding resources confirm that 92551 is reported when earphones are placed on the patient and the patient is asked to respond to tones of different pitches and intensities. If the patient fails to respond during this limited study, additional diagnostic testing is required. That failed-screen-to-referral pathway is exactly where many practices make their second biggest error: Billing 92552 (diagnostic) without actually performing the threshold determination protocol.
According to the AAPC CPT coding guidelines, none of the audiologic function test codes 92551-92598 may be billed unless the clinician is using calibrated electronic equipment. That requirement applies to 92551 even though it is the simplest test in the series. A handheld device that has not been calibrated per manufacturer standards does not meet this threshold. Document the calibration status of your audiometer in your compliance records.
The 92551 vs 92552 question is the most frequent coding question audiologists and primary care coders face. The answer comes down to a single concept: Did the clinician determine a hearing threshold?
The American Academy of Family Physicians describes the distinction clearly: 92551 uses a device that produces a series of tones; if the patient does not hear a certain number of tones, further testing is warranted. At that point, 92552 becomes the appropriate code for an audiologist to use when determining the exact threshold across frequencies. Billing 92552 when only a screen was performed is upcoding. Billing 92551 when a full threshold determination was documented is downcoding. Both create compliance risk.
For practices that also handle other specialty coaching CPT codes or ADHD screening CPT codes, this screening-vs-diagnostic distinction appears across many code families, from audiology to preventive screens billed under HCPCS code G0121 for screening colonoscopy. The logic is consistent: Screen identifies who needs more; diagnostic measures precisely how much.
Payers expect specific documentation elements for every 92551 claim. Missing even one can trigger a denial or a request for additional information during post-payment review.
Practices using digital intake forms can build structured audiology screening templates that capture all required elements automatically. That removes the reliance on paper forms where fields are routinely left blank.
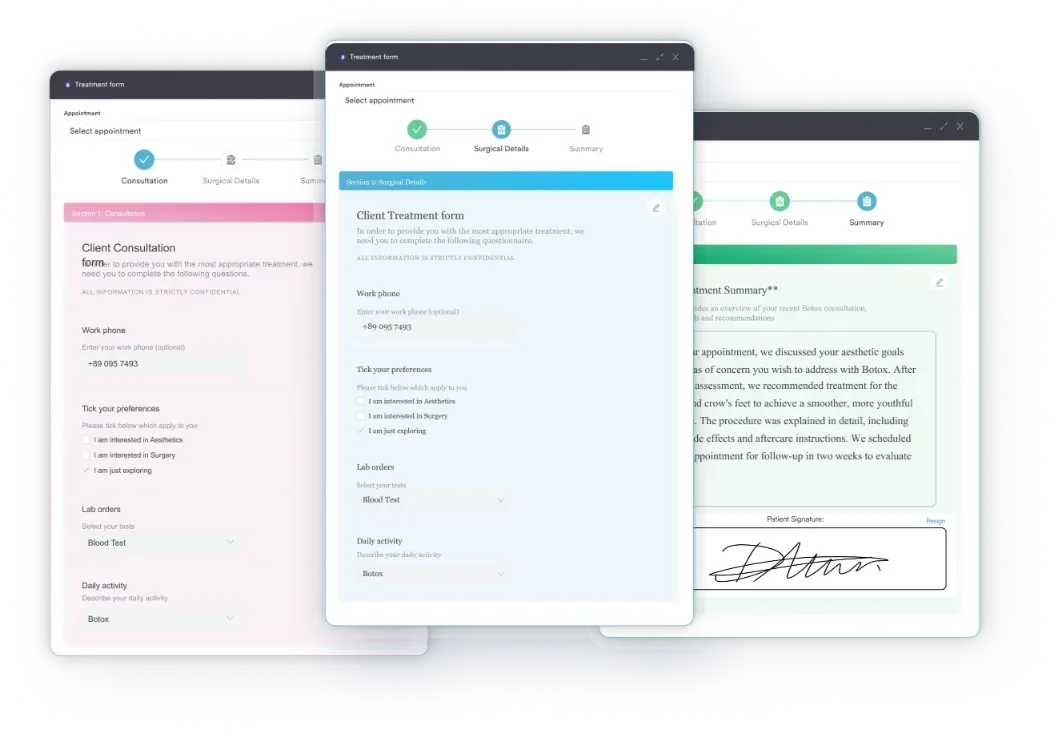
Some practices use automated audiometry devices that present tones without a live technician monitoring the process. The documentation requirements are the same regardless of automation level. What matters to payers is whether calibrated electronic equipment was used, whether air conduction was the testing modality, and whether the result was pass/fail. CPT 92551 applies to both manual and automated pure tone air conduction screens as long as those conditions are met.
Audit your current audiology documentation templates against the eight elements listed above. Practices that add checkboxes for each required field see measurably fewer documentation-related denials on 92551 claims. A single missing element – most commonly the calibration date or the frequencies tested – accounts for the majority of preventable rejections.
Medicare does not cover CPT code 92551 for routine hearing screening. The American Academy of Family Physicians confirms that Medicare Part B excludes pure tone audiometry screening from coverage because hearing examinations are considered routine services under the statute that governs Medicare benefits. This is not a local coverage determination issue; it is a national statutory exclusion.
This means that when you perform CPT 92551 on a Medicare beneficiary, the claim will be denied. You have two compliant options. First, issue an Advance Beneficiary Notice (ABN) before the service, informing the patient that Medicare will not cover this test and that they are responsible for payment. Second, if the screen is being ordered as a diagnostic service (not a routine screen) with a supporting clinical indication, the correct path may be to perform a diagnostic test instead and bill 92552, which can be covered by Medicare when medically necessary.
Modifier -GY (item or service statutorily excluded or does not meet the definition of any Medicare benefit) can be appended to 92551 on a Medicare claim to signal that the service is excluded. Modifier -GZ (item or service expected to be denied as not reasonable and necessary) is used when you believe Medicare will deny coverage and you did not issue an ABN. Use -GZ only when no ABN was obtained; it signals non-compliant practice if used routinely without attempting the ABN process.
Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) program covers CPT 92551 for eligible pediatric patients as part of well-child screenings. Coverage details vary by state Medicaid plan; verify with your specific state’s fee schedule and prior authorization rules. Highmark’s payer policy, for example, confirms CPT 92551 for audio screen as the appropriate code when pure tone air conduction screening is part of an EPSDT visit. If the patient fails, the threshold test (92552) is the next step, and most state EPSDT programs will cover that follow-up as well.
Commercial insurers generally cover 92551 when it is medically necessary and supported by an appropriate diagnosis code. Review each payer’s coverage policies using the CMS Physician Fee Schedule lookup tool for Medicare rates, and check individual commercial payer portals for contracted rates and coverage criteria.
Pabau's claims management tools help audiology practices and primary care teams document, code, and submit hearing screening claims accurately. See how it works for your team.

Modifier selection for CPT 92551 is straightforward in most scenarios. Four modifiers deserve attention:
The modifier -25 point deserves emphasis. It is appended to the E/M code, not to 92551 itself. A common billing error is placing -25 on 92551, which is incorrect. The 92551 claim is submitted without a modifier in most cases. The E/M code carries the -25 to explain why a separate procedure is also being billed on the same date.
For practices handling other specialty procedures, the same modifier-25 logic applies across audiology codes 92551-92557 and extends to other diagnostic procedures performed on the same day as an E/M. Clinics managing multi-specialty billing, including IVF CPT codes, anesthesia services governed by their own rules such as CPT Code 00140 anesthesia guidelines, and comparable procedure-plus-evaluation scenarios, encounter this pattern regularly.
CPT code 92551 has no universal upper age limit for eligible patients. It can be billed for children, adolescents, and adults across all practice settings. However, there is a hard lower age boundary that coders must respect: 92551 is not appropriate for newborns or infants.
Newborn hearing screening uses otoacoustic emissions (OAE) testing or auditory brainstem response (ABR) testing because infants cannot behaviorally respond to pure tone stimuli in a meaningful way. The codes for those services are 92587 (OAE, limited) and 92558 (OAE, screening), among others. Billing 92551 for a newborn in the hospital nursery or NICU is incorrect and will be denied by most payers. This distinction is confirmed by standard audiology coding guidance cited by the American Speech-Language-Hearing Association.
For older pediatric patients, the EPSDT context is the primary consideration. Practices serving pediatric populations should review Children’s Minnesota’s coding-by-age charts and state Medicaid payer policies to confirm age-specific coverage tiers. The HIPAA compliance checklist for primary care is also worth reviewing when setting up pediatric audiology screening workflows, particularly regarding consent documentation for minors and records handling requirements.
Primary care pediatric offices performing routine hearing screens at well-child visits represent one of the highest-volume 92551 billing environments. The HIPAA-compliant documentation workflows within your practice management system need to capture the same calibration and screening protocol data that audiology specialists document, even if the test takes only two minutes at a well visit.
For pediatric practices billing 92551 at well-child visits, create a standing order protocol that specifies the ages at which hearing screening is performed, the equipment used, and the pass/fail criteria. This standing order, combined with your calibration log, becomes your first line of defense in a payer audit.
CPT 92551 sits within the audiologic function tests code range (92550-92598). Understanding how it interacts with adjacent codes prevents unbundling errors and missed revenue.
The most common bundling violation is billing 92551 and 92552 on the same date for the same patient. These two codes describe mutually exclusive tests. A test is either a screening (92551) or a diagnostic threshold determination (92552). It cannot be both. Most payers will deny one automatically via their claims editing software when they appear together. Practices encountering this denial pattern should review their superbill design to ensure the two codes are not accidentally checkmarked together.
Another frequent error: Billing 92551 when 92557 (comprehensive audiometry) was actually performed. Code 92557 is a package code that already includes pure tone air conduction threshold testing. Billing 92551 alongside it is unbundling and will be caught by claims edits at virtually every payer.
Practices also frequently miss the opportunity to bill 92550 (tympanometry) separately when it is performed at the same visit as a pure tone screen. These two codes are not bundled against each other. When both tests are genuinely performed and documented, both should be billed. That is appropriate coding and maximizes compliant revenue. For practices exploring related procedural billing resources, the Bupa procedure code fee schedule illustrates how fee schedules across payers structure audiology-adjacent codes.
Reimbursement for CPT code 92551 varies by payer, geographic location, and contract terms. The Medicare Physician Fee Schedule does not cover 92551 for routine screening, so there is no standard Medicare reimbursement rate for this code in most scenarios. For non-Medicare payers, rates are determined by individual contract terms or state Medicaid fee schedules.
For Medicaid EPSDT programs, state fee schedules typically set a low reimbursement for 92551 reflecting the brief nature of the test (the screen itself may take under five minutes in many settings). Commercial payer rates tend to track above Medicaid rates. Use the AAPC Codify CPT lookup to view national average fee data and benchmark your contracted rates.
Revenue from 92551 in a primary care setting comes largely from volume (EPSDT well-child visits) rather than high per-claim rates. The more significant financial consideration is avoiding the downstream cost of claim denials and resubmissions. A single denied claim that requires staff time to appeal, correct, and resubmit often costs more in labor than the claim is worth. Practices using claims management software with pre-submission claim scrubbing reduce that friction significantly.
For audiology practices also billing bone conduction or comprehensive tests, the combined revenue from 92552 or 92557 (which do carry Medicare coverage when medically indicated) is where most of the fee schedule value sits. Code 92551 is typically the entry point of a hearing care episode, not the primary revenue driver.
Billing errors on CPT code 92551 almost always trace back to two root causes: Confusing the screening code with the diagnostic threshold code (92552), and failing to document the calibrated equipment requirement. Both are entirely preventable with clear protocols and structured documentation templates.
Pabau’s claims management software helps audiology practices, ENT clinics, and primary care teams build audiology-specific documentation workflows that capture every required element before claims go out. Fewer errors at submission means fewer denials, fewer appeals, and faster payment cycles. To see how Pabau handles audiology billing workflows for your team, book a demo.
Need a complete audiology code reference? ADHD screening CPT code covers the screening-versus-diagnostic distinction across neurodevelopmental assessments, useful context for multi-specialty practices.
Billing multiple procedure types? IVF CPT codes demonstrates how procedure bundling rules and modifier requirements apply across specialty billing scenarios.
Looking to improve your practice’s claims accuracy? Practice management software explains how integrated billing and documentation tools reduce claim errors across specialties.
CPT code 92551 is a screening test, pure tone, air only. It tests whether a patient can detect tones at a fixed intensity through air conduction headphones but does not determine precise hearing thresholds. It is used in primary care, pediatric, and EPSDT settings to identify patients who need further audiological evaluation.
CPT 92551 is a pass/fail screening test that does not determine hearing thresholds. CPT 92552 is a diagnostic pure tone audiometry test that does determine the exact threshold (in dB HL) at which a patient can hear each frequency. Never bill both codes for the same patient on the same date; they describe mutually exclusive tests.
No. Medicare does not cover CPT 92551 for routine hearing screening. This is a national statutory exclusion under Medicare Part B. If you perform this test on a Medicare patient, issue an Advance Beneficiary Notice (ABN) beforehand and append modifier -GY to the claim to indicate the service is statutorily excluded.
Yes. When a significant and separately identifiable E/M service is performed on the same date, bill both codes. Append modifier -25 to the E/M code (not to 92551) to indicate the E/M was distinct from the hearing screen. Document the E/M content independently in the medical record.
No. Newborns and infants cannot reliably respond to pure tone stimuli behaviorally, so 92551 does not apply. Use otoacoustic emissions (OAE) codes such as 92587 for limited OAE or 92558 for screening OAE testing when screening newborns. Using 92551 for newborn screens results in claim denials and may create compliance exposure.
Common supporting diagnosis codes include Z01.10 (encounter for examination of ears and hearing without abnormal findings), Z01.110 (encounter for hearing examination following failed hearing screening), and H91.90 (unspecified hearing loss, unspecified ear). For EPSDT well-child visits, the well-child Z-code typically serves as the primary diagnosis, with a hearing-concern code as secondary. Always verify with the specific payer’s medical necessity criteria.



