CPT Code 15276: Skin substitute graft add-on billing guide
CPT Code 15276 is an add-on procedure code for applying a skin substitute graft ...
Last Updated: July 30, 2026
CPT code 11601 describes excision of a malignant skin lesion including margins on the trunk, arms, or legs, with an excised diameter of 0.6 to 1.0 cm.
A pathology report confirming malignancy is required for Medicare medical necessity under CMS LCD Article A57660.
The excised diameter measurement includes surgical margins, not just the visible lesion – selecting the wrong size tier is a top denial trigger.
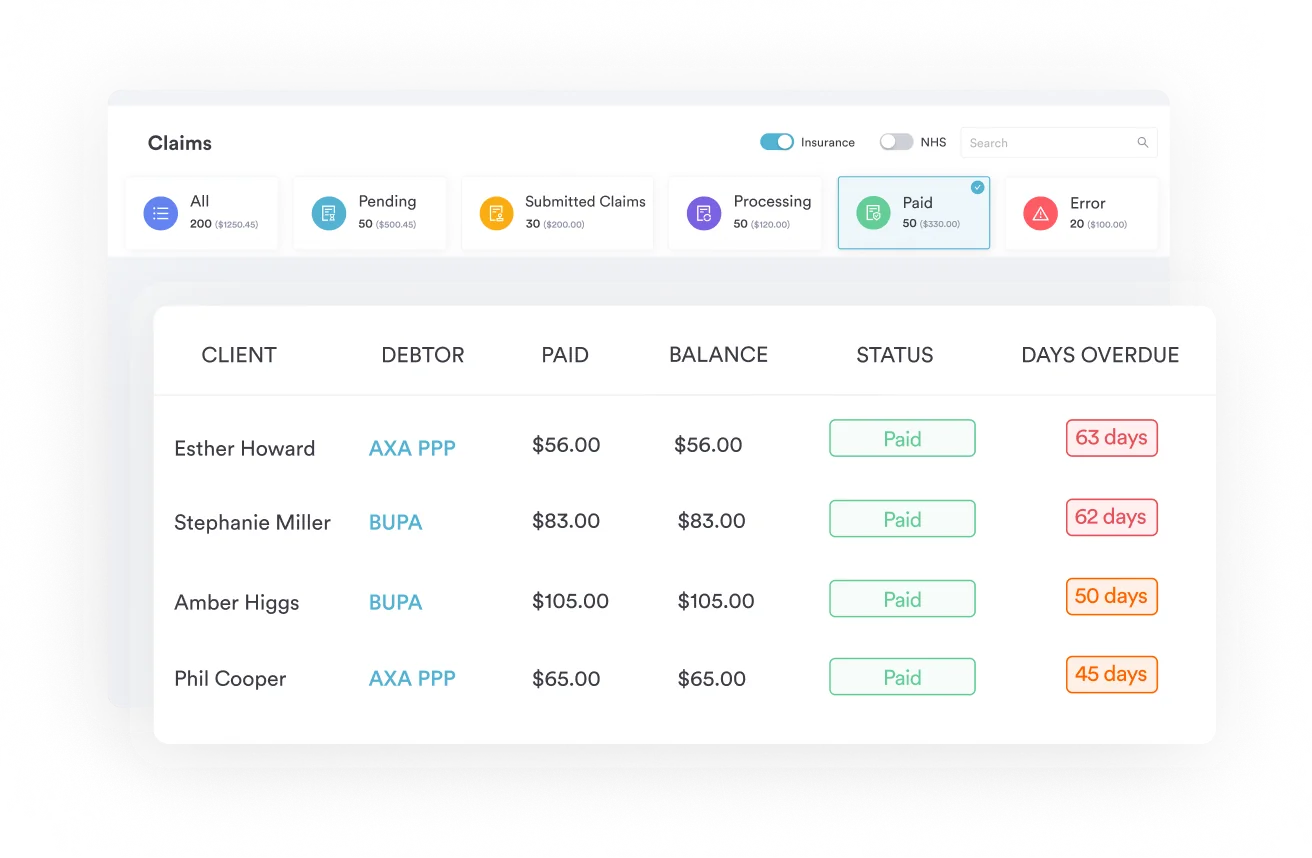
Pabau’s claims management software helps dermatology and plastic surgery practices reduce coding errors and track claim status in real time.
CPT code 11601 reports the excision of a malignant skin lesion, including margins, on the trunk, arms, or legs, with a total excised diameter of 0.6 to 1.0 cm. Medicare requires a pathology report confirming malignancy, and the excised diameter must include surgical margins, not just the visible lesion.
Malignant skin lesion excisions are among the most frequently billed dermatology procedures, and coding them incorrectly costs practices money on every claim. CPT code 11601 sits in the middle of the 11600-11646 code family, covering a specific anatomical location and size range that billers must get exactly right to avoid denial.
This reference guide covers the CPT code 11601 descriptor, excised diameter measurement rules, applicable modifiers, ICD-10 pairings for medical necessity, Medicare reimbursement benchmarks, and the most common billing errors that trigger denials for this code.
The American Medical Association (AMA) CPT code set describes CPT code 11601 as: Excision, malignant lesion including margins, trunk, arms, or legs; excised diameter 0.6 to 1.0 cm. Practices using claims management software can flag miscoded anatomical sites before submission, reducing avoidable rejections from the start.
The anatomical scope is precise. “Trunk, arms, or legs” covers the chest, back, abdomen, buttocks, upper and lower extremities, and the shoulders. Billers must not use CPT code 11601 for lesions on the face, ears, eyelids, nose, lips, or genitalia — those fall under the 11640-11646 family.
The measurement that determines which code to use is the total excised diameter, not the visible lesion size. Surgeons must add the margin width on all sides to the lesion diameter before selecting a code. A 0.4 cm lesion with 0.2 cm margins on each side produces a 0.8 cm excised diameter, placing it squarely under CPT code 11601. Documenting only the lesion size and ignoring margins is a frequent audit trigger.
CMS LCD Article A57660 explicitly lists CPT code 11601 as one of the codes covered when paired with appropriate malignant neoplasm diagnosis codes. Every claim must carry at least one ICD-10-CM code that confirms the lesion is malignant or of uncertain morphology warranting excision. Practices using dermatology EMR software can build code pairing templates that auto-populate the correct ICD-10 codes based on documented diagnosis, removing manual lookup errors.
Commonly paired ICD-10-CM codes include:
Medicare requires a pathology report confirming malignancy before processing the claim as medically necessary. Submitting CPT code 11601 without corresponding pathology documentation is one of the leading causes of post-payment audits in dermatology. Use the CrossCoder CPT-to-ICD-10 crosswalk to verify pairing accuracy before each submission. Clinics that standardize full body mole mapping workflows alongside excision procedures can capture complete diagnosis documentation at the point of care.
Document the ICD-10 code at the time of biopsy result, not at the time of excision scheduling. When the pathology report arrives, immediately link the confirmed malignancy code to the pending excision encounter in your practice management system. This closes the documentation gap that auditors most commonly flag.
Modifier selection for CPT code 11601 depends on the clinical scenario and payer. Using the wrong modifier, or omitting one that a payer requires, results in bundling edits or outright denials. Dermatology and plastic surgery EMR platforms that support modifier tracking by payer rule set help billing teams stay current as individual payer policies change. For additional CPT modifier references across procedure types, CPT code reference guides on Pabau cover common modifier scenarios in detail.
Multiple Surgery Reduction Rule (MSRR): When CPT code 11601 is billed as a secondary procedure on the same date as a primary excision, Medicare may reduce reimbursement by 50%. This is a CMS policy applied through modifier -51. Confirm current MSRR applicability for your payer mix using the CMS Physician Fee Schedule lookup tool, as reduction percentages and applicability can vary by year and payer.
Pabau's claims management tools help dermatology and skin clinic teams pair the right ICD-10 codes, flag modifier issues, and track claim status without switching between systems.

CMS calculates Medicare reimbursement for CPT code 11601 using the Resource-Based Relative Value Scale (RBRVS). The national non-facility rate typically falls in the range of $130 to $200 depending on the geographic practice cost index (GPCI) applied to your region. These figures change annually with each CMS Physician Fee Schedule update. Verify the current rate for your locality using the FastRVU 2026 RVU lookup tool before quoting estimated patient cost-sharing. Practice management tools that auto-populate digital intake forms with current fee estimates help reduce billing surprises at checkout.
Commercial payer rates vary considerably and are often negotiated as a percentage of the Medicare fee schedule. Practices should confirm contracted rates for CPT code 11601 with each payer before scheduling to avoid underpayment write-offs.
CPT code 11601 carries different RVU values depending on where the procedure is performed. Non-facility (office) rates are higher because the physician’s overhead includes the procedure room, instruments, and supplies. Facility rates (hospital outpatient or ASC) are lower because CMS pays the facility separately for resources. Always confirm with your billing team which place of service code (POS) they are submitting to ensure the correct fee schedule applies.
Run a quarterly audit of your CPT 11601 claims against the current Medicare fee schedule for your locality. Use the CMS Physician Fee Schedule lookup to pull your locality’s conversion factor and compare against actual payments received. A 5% discrepancy on a high-volume code adds up quickly across a full year of claims.
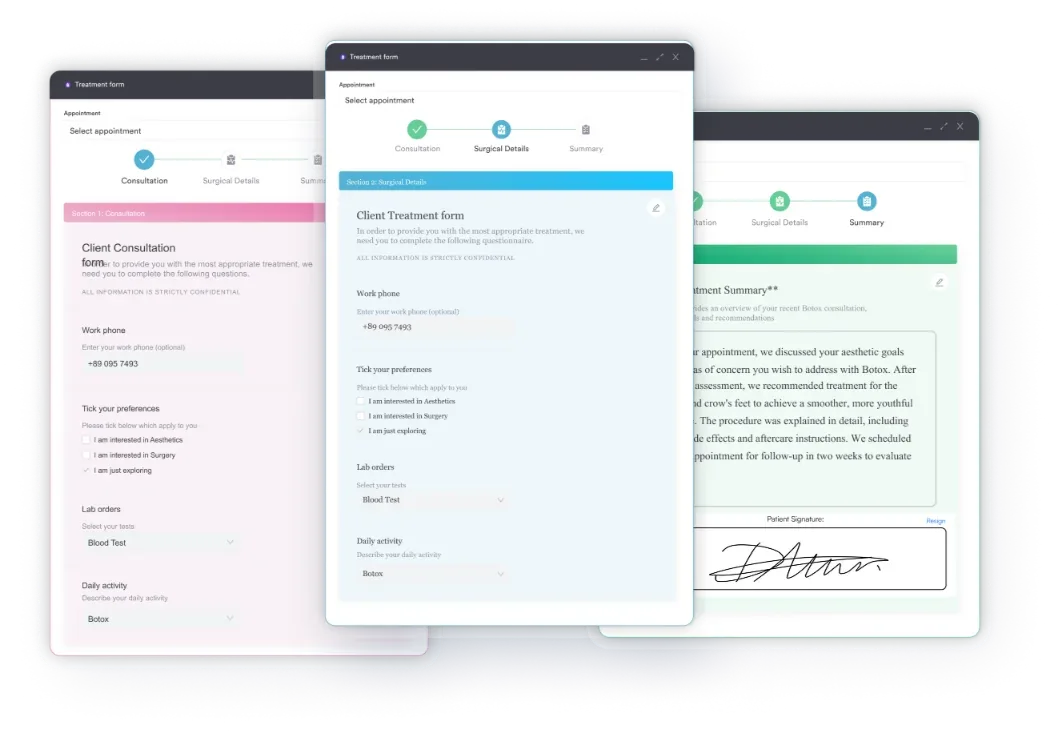
Complete documentation is the single strongest defense against denials and post-payment audits for CPT code 11601. Structured medical documentation forms that prompt providers to record all required data points at the time of service prevent retrospective chase-and-correct workflows. Good skin clinic software builds these prompts into the clinical note template so nothing is missed under time pressure.
Required documentation for CPT code 11601 claims includes:
When a malignant excision requires wound closure beyond simple closure, billing a separate repair code is appropriate. CPT 12031 (intermediate repair, 2.5 cm or less) is the most common repair code paired with CPT code 11601. To bill both on the same date, append modifier -59 or -XS to CPT 12031 to indicate a separate, distinct service. Medical spa compliance requirements for documenting combination procedures are similar: each service needs its own operative note section with size, location, and medical necessity rationale. Use the AAPC Codify CPT lookup to confirm current bundling edits for any code pair before billing.
When multiple malignant lesions are excised at the same session, bill each excision separately using the appropriate size-tier code. Bill the largest excision first at 100% of the fee schedule. Medicare may subject subsequent excisions to MSRR reductions under modifier -51. Practice management tools for plastic surgeons that support multi-procedure encounters help billing teams sequence codes correctly and apply modifiers in the right order.
Accurate billing for malignant skin excisions starts with measuring correctly and documenting completely. CPT code 11601 is one of the most commonly billed codes in dermatology and plastic surgery, and payers audit it more than almost any other code in the family. Getting the excised diameter right, pairing the correct ICD-10-CM code, and attaching the pathology report before submission are the three actions that prevent the majority of denials.
Pabau’s practice management software supports dermatology and skin clinic teams with structured clinical note templates, integrated claims workflows, and diagnosis code pairing tools. To see how Pabau handles surgical billing documentation end-to-end, book a demo.
Managing dermatology billing across multiple sites? Dermatology EMR software from Pabau supports structured clinical notes and multi-location claim tracking.
Looking for skin-specific practice management features? Skin clinic software with integrated billing workflows reduces the time between excision and clean claim submission.
Want a full overview of surgical billing best practices? Claims management software helps practices catch ICD-10 pairing gaps and modifier errors before claims go out the door.
CPT code 11601 is used to report the excision of a malignant skin lesion, including surgical margins, located on the trunk, arms, or legs, with a total excised diameter of 0.6 to 1.0 cm. It is used by dermatologists, plastic surgeons, and general surgeons and requires a supporting pathology report for Medicare medical necessity.
CPT 11600 applies to malignant excisions on the trunk, arms, or legs with an excised diameter of 0.5 cm or less, while CPT 11601 applies when the excised diameter (including margins) measures 0.6 to 1.0 cm. Both require pathology confirmation and appropriate ICD-10-CM diagnosis codes.
Yes. CMS LCD Article A57660 requires a pathology report verifying malignancy for CPT 11601 to be considered medically necessary under Medicare. Claims submitted without pathology documentation are subject to denial or post-payment audit.
Yes, when the excision requires intermediate wound closure. Append modifier -59 or -XS to CPT 12031 to indicate it is a distinct service from the excision. Billing both codes without a modifier on the same date triggers NCCI bundling edits and automatic rejection.
The excised diameter includes the lesion and all surgical margins, measured as the greatest single dimension of the entire specimen. The margin width is added to the lesion diameter before code selection. Documenting only the lesion size and omitting margins is an audit trigger and may result in incorrect code selection.