ICD-10 Code Q25.8: Other congenital malformations of other great arteries
ICD-10 Code Q25.8 is the billable ICD-10-CM diagnosis code for other congenital ...
Last Updated: July 27, 2026
H26.9 is the ICD-10-CM code for unspecified cataract, billable and valid for FY2026 under the Disorders of Lens block (H25-H28).
Use H26.9 when documentation does not specify cataract type, etiology, or laterality; it is the Alphabetic Index default for ‘Cataract.’
H25.9 applies to age-related (senile) cataracts; H26.9 is the correct fallback when etiology is absent from the clinical record.
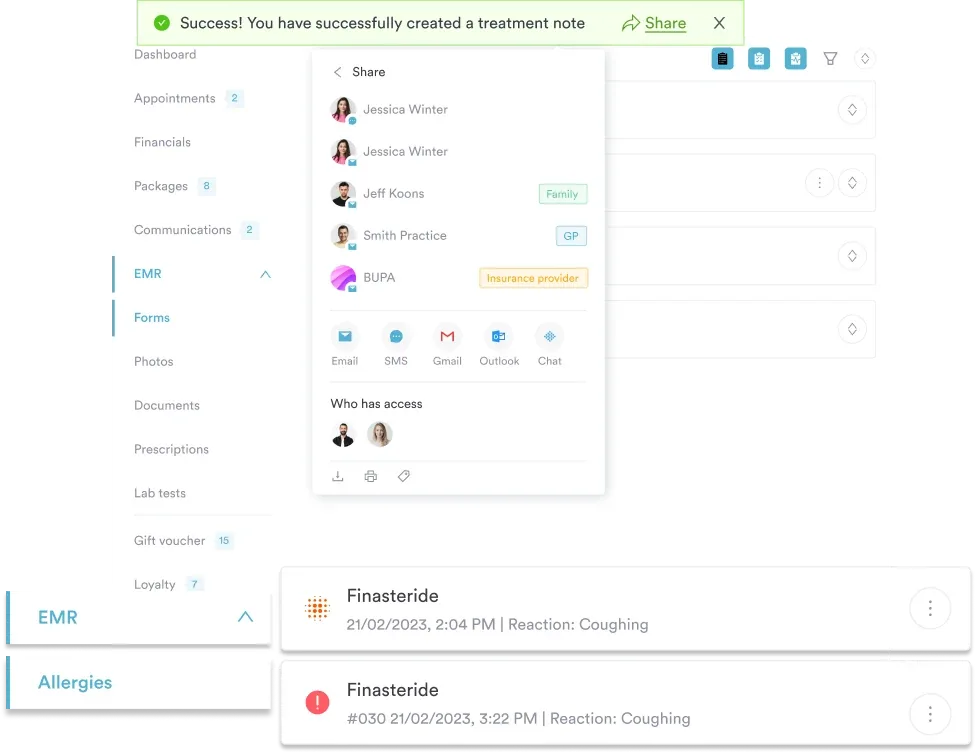
Pabau’s claims management software flags unspecified diagnosis codes before submission, reducing denials linked to insufficient documentation.
ICD-10 Code H26.9 represents Unspecified Cataract within the ICD-10-CM classification, maintained jointly by the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). It belongs to Chapter 7 (Diseases of the Eye and Adnexa, H00-H59), specifically the Disorders of Lens block (H25-H28), under the parent category H26 Other cataract.
A cataract is a clouding of the crystalline lens that progressively impairs vision. The “unspecified” designation in H26.9 means the clinical record does not identify the type (nuclear, cortical, subcapsular), the cause (age-related, traumatic, drug-induced, congenital), or the precise laterality at the time of coding.
According to the WHO ICD-10 browser, cataracts fall under opacification of the crystalline lens. The unspecified designation is reserved for presentations where the clinical encounter does not yield enough detail to assign a more granular code.
H26.9 is a valid, billable ICD-10-CM diagnosis code for FY2026. It requires no additional characters to be reportable, which makes it one of the few codes in the H26 category that stands alone without a laterality or type suffix.
Because H26.9 carries no laterality requirement, it is also used in practice when bilateral cataracts are present but no further type specification appears in the documentation. Per guidance from the AAPC Codify ICD-10-CM lookup, modifiers are not appended to ICD-10-CM diagnosis codes, so a single H26.9 covers bilateral presentations when specificity is absent.
Practices that manage ophthalmology workflows alongside other specialties benefit from structured patient records in practice management software like Pabau, which flag missing documentation elements before a claim reaches the payer. When a chart note says “cataract OD” without specifying age-related, traumatic, or congenital origin, H26.9 is the appropriate code. Payer scrutiny rises when an unspecified code pairs with a complex procedure like cataract extraction.
Run an internal audit of cataract claims coded H26.9 over the past 90 days. Flag any paired with CPT codes 66982 or 66984 (cataract extraction). Payers may request documentation proving specificity was genuinely unavailable, not overlooked. A brief notation in the chart such as ‘etiology undetermined at this encounter’ reduces denial risk substantially.
The most frequent coding error in this category is using H26.9 when H25.9 (Unspecified age-related cataract) applies. These two codes cover the same surface concept but diverge on a single clinical distinction: whether the cataract is documented as age-related (also called senile).
Practices covering mixed ophthalmology and primary care panels should build query templates into their digital intake forms to capture patient age, trauma history, and systemic diagnoses upfront. A diabetes eye exam template standardizes this intake for patients with a diabetic history. This reduces the frequency of unspecified fallback coding and supports more accurate specificity across the encounter.
The same documentation habits apply to other nonspecific ophthalmic codes, such as H01.9 (unspecified inflammation of eyelid) and H02.9 (unspecified disorder of eyelid). When an eyelid finding progresses to surgical correction, our eyelid surgery (blepharoplasty) template covers the associated documentation.
When a cataract affects both eyes but the record still names no type, cause, or age-related origin, H26.9 is reported once. ICD-10-CM diagnosis codes carry no bilateral modifier, so a single unspecified cataract code covers a bilateral presentation rather than two separate line items.
Laterality works differently once the cataract is specified. The age-related codes carry a laterality digit, so H25.13 is age-related nuclear cataract of both eyes, while H26.9 stays unspecified whether the cataract is in the right eye, the left eye, or both. If the chart records which eye is affected but nothing about type or etiology, H26.9 is still correct. Documented laterality alone does not move the code to a more specific option.
This distinction matters most on surgical claims. Cataract extraction is billed per eye using a laterality modifier on the procedure code, but the diagnosis stays H26.9 for each date of service until the documentation supports a specified type. Coders who go looking for a dedicated “bilateral cataract” ICD-10 code lose time searching for one that was never created.
Payers increasingly scrutinize unspecified diagnosis codes, particularly when paired with surgical procedures. The CDC/NCHS ICD-10-CM coding tool and the ICD-10-CM Official Guidelines for Coding and Reporting consistently emphasize coding to the highest level of specificity documented. H26.9 is appropriate, but the chart must actively support the choice. Choosing the right clinical documentation software makes that support easier to produce consistently.
Minimum documentation elements to support an H26.9 claim:
For practices using EHR or practice management systems, AI-assisted clinical documentation can prompt physicians to capture these specificity markers during the encounter rather than after the fact. Tools covered in our guide to AI clinical documentation shorten the lag between the exam and the chart note a coder ultimately reviews.
Retroactive chart amendment is permitted under ICD-10-CM guidelines, but addenda added after a claim denial carry less weight than contemporaneous notes. The same documentation principle applies across all ICD-10 unspecified codes: document why specificity was unavailable, not just that it was.
Pabau helps ophthalmology and optometry practices capture the clinical detail needed to code accurately the first time. Structured intake forms, AI-assisted notes, and built-in claims management reduce unspecified-code denials before they happen.

Understanding the codes adjacent to H26.9 helps coders select the most appropriate option and reduces the risk of payer queries. The H25-H28 block covers the full range of lens disorders in the ICD-10-CM Tabular List.
Per the ICD10Data.com reference, synonyms included under H26.9 include anterior capsular lens opacities, anterior lens opacities, and anterior subcapsular cataract where no further type specification is available.
Practices managing high volumes of complex ICD-10 diagnosis codes across specialties benefit from centralized compliance management workflows that enforce documentation standards at the point of care rather than at claims review. Linking the diagnosis code selection to a templated note structure reduces the rate of unspecified fallback coding across the board.
Cataract encounters generate claims beyond the diagnosis code itself. Procedure codes commonly billed alongside H26.9 include CPT 92002 (intermediate eye exam for new patients), CCSD C7520 (phacoemulsification of lens with implant), and CPT 66999 (unlisted procedure, anterior segment of eye) when the surgical approach doesn’t match a listed code.
Post-surgical vision correction adds another billing layer. Practices commonly report the following codes for eyewear dispensed after cataract surgery:
Coders working across the H00-H59 chapter encounter the same specificity-first logic in other nonspecific codes, including H16.8 (other keratitis) and H34.9 (unspecified retinal vascular occlusion).
Check payer Local Coverage Determinations (LCDs) before submitting H26.9 paired with cataract surgery CPT codes. Some Medicare contractors and commercial payers require a more specific ICD-10 code to approve prior authorization for lens extraction. Confirm documentation supports the unspecified designation before submission.
Unspecified diagnosis codes are not coding errors. H26.9 exists precisely for clinical encounters where etiology and type are genuinely undetermined. The risk comes from submitting H26.9 without documentation that explains why specificity was unavailable.
Pabau’s claims management software helps ophthalmology and optometry practices build the documentation habits that support accurate coding from the first encounter. Structured intake, AI-assisted notes, and pre-submission claim checks reduce the denials that follow unspecified codes into payer review. Book a demo to see how Pabau handles ophthalmology documentation workflows end to end.
Need a structured clinical notes framework? Safer clinical notes covers documentation practices that reduce audit exposure across all diagnosis categories.
ICD-10 Code H26.9 is the ICD-10-CM diagnosis code for Unspecified Cataract, a billable code valid for FY2026 under Chapter 7 (Diseases of the Eye and Adnexa) in the Disorders of Lens block (H25-H28). It is used when clinical documentation identifies a cataract but does not specify its type, cause, or laterality.
Use H26.9 when the chart does not document any information about the cataract’s cause or type. Use H25.9 (Unspecified age-related cataract) when the physician’s notes confirm the cataract is age-related or senile, even if the morphological subtype is not specified. The distinction rests entirely on whether “age-related” appears in the documentation.
Yes. H26.9 is a valid, billable ICD-10-CM diagnosis code for FY2026. It requires no additional characters and can be reported independently without a laterality or type suffix, making it the appropriate code when documentation genuinely lacks specificity.
When bilateral cataracts are present but no further type or etiology is documented, H26.9 is reported as a single code. The ICD-10-CM Alphabetic Index maps the default entry for “Cataract” to H26.9, and diagnosis codes do not accept bilateral modifiers. If the bilateral cataracts are confirmed as age-related, H25.9 applies instead.
H26.9 has no laterality character, so it applies to a cataract in the right eye, the left eye, or both when the type and cause are not documented. Knowing which eye is affected does not make the diagnosis more specific on its own. To move beyond an unspecified cataract code, the record needs the morphology or etiology, such as age-related, traumatic, or congenital.
In medical coding, “unspecified cataract” means the clinical documentation does not provide enough detail to assign a more granular code. That reflects incomplete clinical detail at the encounter rather than a coding error. Coders should always select the most specific code the documentation supports, and H26.9 is the correct choice when no further detail exists.