HCPCS code A4210: Needle-free injection device billing guide 2026
HCPCS code A4210 is the Level II supply code for a needle-free injection device,...
July 21, 2026
ICD-10 code C61 is the billable diagnosis code for malignant neoplasm of the prostate, covering active prostate cancer under ICD-10-CM range C60-C63.
After definitive treatment with no residual disease, switch to Z85.46 (personal history of malignant neoplasm of prostate), not C61, to avoid claim denials.
Metastatic prostate cancer requires C61 as the primary code plus secondary site codes such as C79.51 (bone) or C79.82 (genital organs), always sequencing C61 first.
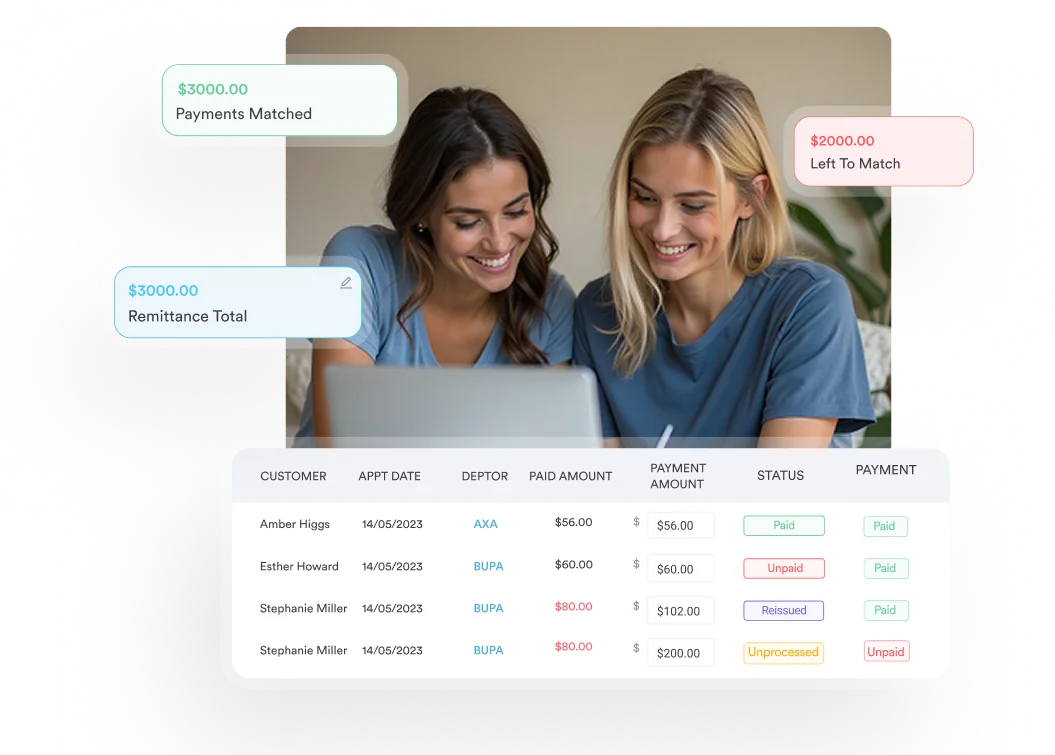
Pabau’s claims management software and structured client records help oncology and men’s health practices document staging, treatment status, and hormone therapy accurately for clean claims.
C61 is the ICD-10 code for prostate cancer, malignant neoplasm of the prostate, and it’s the billable ICD-10-CM diagnosis (dx) code you report for cancer at the primary site. It sits within the C60-C63 range (malignant neoplasms of male genital organs) under the broader C00-D49 neoplasm chapter. The men’s health clinic software category is where this code appears most in practice management contexts, but C61 is relevant to any specialty that treats or monitors prostate malignancy, including urology, radiation oncology, and primary care.
The code descriptor covers carcinoma of the prostate regardless of histological subtype (adenocarcinoma, small cell, ductal), provided the malignancy is located at the prostate as the primary site. It does not distinguish by Gleason score, TNM stage, or Grade Group. Those clinical details belong in the physician’s documentation to support the code selection, not in the code itself.
The distinction between the C61 leaf node and the C61- header category matters. The header (C61-) is listed as non-billable in many code lookup tools because it is a category header; the leaf node C61 is the specific, billable code. Always report C61, not C61-, on claims.
Use C61 when the patient has a confirmed, active diagnosis of prostate cancer and the malignancy is at the primary site. The code applies across all treatment phases: active surveillance, watchful waiting, ongoing radiation therapy, chemotherapy, hormone therapy, and surgical treatment where residual disease remains or has not yet been confirmed absent.
More than 95% of prostate malignancies are acinar adenocarcinoma, and every one of them codes to C61. The adenocarcinoma of the prostate ICD-10 assignment does not change with histologic variant. Ductal, mucinous, and small cell or neuroendocrine carcinomas of the prostate still report C61 as the prostate cancer ICD-10 code, with the specific subtype captured in pathology documentation rather than a separate code. The one exception is a pre-invasive lesion: carcinoma in situ is D07.5, not C61.
For patient care management that spans multiple providers and treatment phases, consistent code assignment across encounters reduces downstream billing discrepancies and supports continuity in care coordination records.
This is the most common coding error in prostate cancer management. Many practices continue using C61 indefinitely after the patient completes definitive treatment, when the correct code switches to Z85.46 (personal history of malignant neoplasm of prostate). Using C61 after the cancer is no longer present creates claim confusion and may trigger medical necessity reviews.
The rule is straightforward in principle: when the prostate has been removed and there is no clinical or pathological evidence of residual or recurrent disease, Z85.46 is the correct code. Continuing to report C61 misrepresents the clinical status and can lead to inappropriate treatment authorizations or audit issues. For ICD-10 coding guidance on related oncology scenarios, the same active-versus-history distinction applies across cancer code families.
Document the clinical basis for code selection at every encounter. For post-treatment monitoring visits, the physician note should explicitly state whether active disease is present, suspected, or absent. That single sentence determines whether C61 or Z85.46 applies, and it is your audit defense.
Prostate cancer rarely codes in isolation. Most encounters require one or more additional codes to reflect metastatic sites, treatment history, or concurrent therapies. Knowing which secondary codes attach to C61, and in what sequence, prevents the most common claim rejections in oncology billing. The AAPC Codify ICD-10-CM lookup provides current crosswalk data for each of these codes. For context on how ICD-10 diagnostic codes are structured across different disease categories – from oncology entries like C61 to dermatological codes such as unspecified contact dermatitis due to chemicals – the hierarchical logic is consistent throughout the classification system.
When prostate cancer has spread to secondary sites, the metastatic prostate cancer ICD-10 sequence follows one clear rule: C61 is always the primary (first-listed) code, and the secondary site codes follow. This reflects that the prostate is the primary site of origin, even when the metastatic disease drives the clinical encounter.
Bone metastasis is the most clinically significant secondary site in prostate cancer. According to the CDC/NCHS ICD-10-CM web tool, C79.51 is the standard code for secondary malignant neoplasm of bone and is the most frequently paired secondary code with C61 in Medicare claims data.
Bone is the site prostate cancer spreads to first in most metastatic cases, so C79.51, secondary malignant neoplasm of bone, is the code you pair with C61 most often. Report the primary site first, then the metastatic site, then any ongoing therapy:
Never reverse this sequence. Listing C79.51 first signals to the payer that the bone is the primary site, which misrepresents the malignancy and can change the DRG grouping, the medical necessity determination, and the reimbursement amount.
When prostate cancer has spread to both bone and other organs (bladder, lymph nodes, distant organs), report C61 first and then each secondary site code separately. The WHO ICD-10 browser describes the hierarchical logic governing primary-to-secondary sequencing across neoplasm categories. There is no limit on the number of secondary site codes that can accompany C61, provided each is clinically documented.
Pabau's claims management tools help urology and oncology practices document staging, treatment status, and hormone therapy coding accurately – reducing errors before submission.

The code C61 is only as defensible as the documentation behind it. CMS and payer auditors look for specific clinical elements in the record before accepting a malignancy code on a claim. Missing any of these creates exposure on retrospective review.
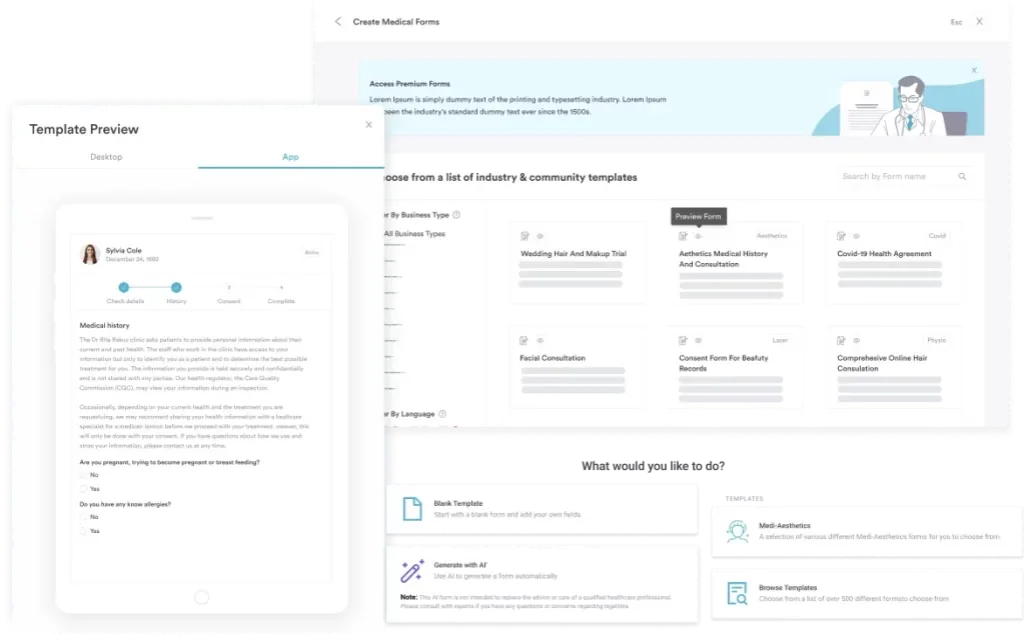
Practices using patient intake software can build prostate cancer-specific templates that prompt clinicians for all required documentation fields at point of care. Combining that with structured patient records ensures that staging data, treatment history, and current status are consistently captured and retrievable. For the kind of audit trail this requires, clinical coding documentation standards in other oncology contexts follow the same underlying CMS guidance.
Build a prostate cancer encounter template in your EHR that prompts for Gleason score, TNM stage, current treatment modality, and PSA trend at every oncology visit. Incomplete documentation is the single most preventable cause of C61 claim denials.
Under MS-DRG v43.0, an inpatient stay for prostate cancer that includes an operating-room procedure such as radical prostatectomy groups into one of two surgical DRGs, depending on whether a complication or comorbidity (CC) or major complication or comorbidity (MCC) is present:
The CC/MCC distinction matters because DRG 715 carries a higher relative weight and therefore a higher Medicare base payment than DRG 716. Documenting and coding comorbidities accurately – not just the prostate cancer itself – directly affects inpatient reimbursement. A patient admitted for radical prostatectomy who also has hypertension, diabetes, a treatment-related condition such as secondary sideroblastic anemia due to disease, or a documented surgical complication may qualify for DRG 715; failure to capture those comorbidities on the claim means the facility receives the lower DRG 716 rate. Note that DRGs 715 and 716 apply only when an O.R. procedure is performed; a non-surgical prostate cancer admission groups instead into MS-DRG 722-724 (malignancy, male reproductive system, with MCC, with CC, or without CC/MCC).
Using claims management workflows that flag missing secondary diagnoses before submission reduces this revenue leakage. Practices with compliance management tools integrated into their billing workflow are better positioned to catch CC/MCC documentation gaps at coding review, not after a remittance shortfall. HIPAA-compliant medical records practices also protect the audit trail that supports DRG assignment during external reviews.
Androgen deprivation therapy is a cornerstone treatment for intermediate- and high-risk prostate cancer, and the ICD-10-CM tabular list includes a “use additional code” instruction for ongoing antiandrogen use. When the patient is currently receiving ADT (LHRH agonists, LHRH antagonists, or antiandrogens such as enzalutamide or abiraterone), report Z79.81 alongside C61.
Z79.81 is specifically designated for long-term (current) use of antiandrogens. It is distinct from Z79.890, which covers hormone replacement therapy in other clinical contexts. Using Z79.890 for prostate cancer ADT is incorrect; the tabular instruction points specifically to Z79.81 for antiandrogen use. Per the CMS ICD-10-CM Official Guidelines, “use additional code” instructions are not optional: where the clinical scenario applies, the additional code should be reported.
Prostate cancer coding pivots on three decisions: whether the disease is still active (C61 vs. Z85.46), whether metastatic sites need secondary codes in the correct sequence, and whether hormone therapy warrants Z79.81. Getting any of these wrong generates denials, audit exposure, and inaccurate DRG assignments.
Pabau’s practice management tools give urology and men’s health practices the documentation structure and claims workflows to get C61 coding right at the point of care, not during a rework cycle. To see how Pabau supports accurate oncology billing, book a demo.
Need documentation templates for oncology encounters? Digital clinical forms covers how structured intake and clinical templates reduce documentation gaps at point of care.
Managing men’s health coding across multiple locations? Men’s health clinic software outlines the workflow and compliance features built for this specialty.
Looking for related oncology coding reference? Clinical coding documentation standards covers ICD-10 sequencing principles applicable across oncology and acute conditions.
ICD-10 code C61 is the billable diagnosis code for malignant neoplasm of the prostate, covering active prostate cancer at the primary site under the ICD-10-CM classification maintained by the CDC/NCHS. It falls within the C60-C63 range (malignant neoplasms of male genital organs) and applies to all histological subtypes of prostate malignancy provided the prostate is the primary site of origin.
Use C61 when active prostate cancer is present, including during active surveillance, ongoing treatment, and documented recurrence. Switch to Z85.46 (personal history of malignant neoplasm of prostate) only after definitive treatment – typically radical prostatectomy or radiation – when there is no clinical evidence of residual or recurrent disease. Continuing to report C61 after cancer is no longer present creates claim confusion and may trigger audits.
Yes, C61 is a billable ICD-10-CM code. The parent category header C61- is listed as non-billable in some lookup tools because it functions as a category header, but the leaf node C61 itself is fully billable and valid for diagnosis reporting on claims for FY 2026 (effective October 1, 2025).
Report C61 first (primary site), followed by C79.51 (secondary malignant neoplasm of bone) as the secondary code. If androgen deprivation therapy is ongoing, add Z79.81 (long-term use of antiandrogens) as a third code. Never reverse the sequencing: listing C79.51 first misrepresents the bone as the primary malignant site, which changes DRG assignment and reimbursement.
Under MS-DRG v43.0, C61 groups into DRG 715 (Other male reproductive system O.R. procedures for malignancy with CC/MCC) or DRG 716 (without CC/MCC) for inpatient claims. DRG 715 carries a higher relative weight and reimbursement rate; capturing all documented comorbidities and complications accurately determines which DRG applies.
C61 represents active invasive malignancy of the prostate. D07.5 represents carcinoma in situ of the prostate, a pre-invasive lesion that has not yet invaded the surrounding tissue. The two codes are mutually exclusive for the same site: use D07.5 for pre-invasive findings and C61 only once a diagnosis of invasive malignancy is confirmed by pathology.
Use Z12.5 (encounter for screening for malignant neoplasm of prostate) for an asymptomatic screening visit, not C61. If the PSA comes back raised but no cancer is confirmed, report R97.20 (elevated PSA) instead. C61 applies only once a biopsy confirms malignancy.
Z80.42 (family history of malignant neoplasm of prostate) documents a patient’s inherited risk, usually on screening or surveillance encounters. It records why a man is being monitored and never stands in for C61, which is reserved for an active, confirmed diagnosis.
Report R97.20 for a nonspecific raised prostate specific antigen result, or R97.21 for a rising level following treatment. A high reading alone does not support C61, which requires pathology confirmation of active prostate cancer.
Code C61 as the first-listed diagnosis, then add a secondary neoplasm code for each site the disease has reached. Bone spread is reported with C79.51, and other organ sites each take their own C79.x code. The primary tumor always sequences ahead of the metastatic sites, which keeps the DRG grouping and reimbursement accurate.
C61 is the code for unspecified prostate cancer. The classification does not subdivide malignant neoplasm of the prostate by laterality or histologic subtype, so a confirmed prostate malignancy with no further specification still maps to C61, with any subtype captured in the pathology report.