ICD-10 code N83.8: Other noninflammatory disorders of ovary
ICD-10 Code N83.8 is the billable ICD-10-CM code for other noninflammatory disor...
Last Updated: July 28, 2026
C25.7 is a billable ICD-10-CM code covering malignant neoplasm of other parts of pancreas, including the neck, uncinate process, and ectopic pancreatic tissue
C25.7 groups into MS-DRG 435, 436, and 437 under MS-DRG v43.0, with reimbursement varying by MCC and CC presence
Never default to C25.9 (unspecified) when operative or pathology reports identify the neck or uncinate process as the tumor site
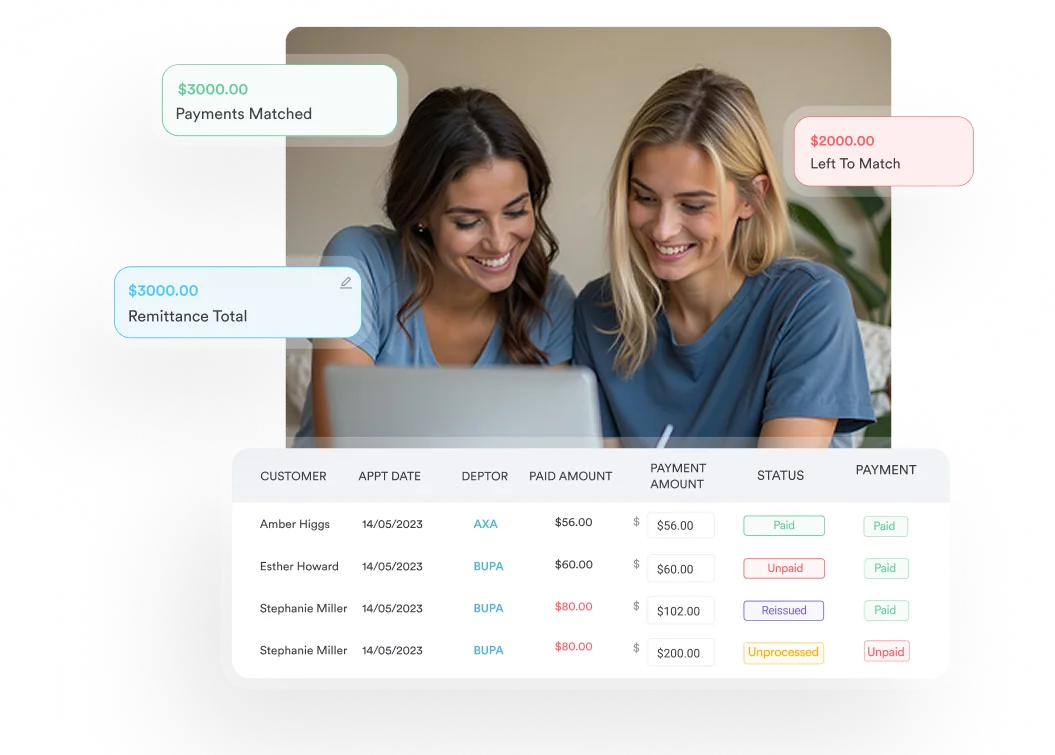
Practice management software like Pabau helps oncology and gastroenterology billing teams track C25.7 claims and reduce pancreatic cancer coding errors
ICD-10 Code C25.7 is the billable ICD-10-CM diagnosis code for malignant neoplasm of other parts of pancreas, including the neck of the pancreas. It is valid for HIPAA-covered transactions beginning October 1, 2024, per ICD List. The code sits within chapter C00-D49 (Neoplasms) of the ICD-10-CM tabular list, under category C25 (Malignant neoplasm of pancreas).
C25.7 captures pancreatic tumors located at sites not individually represented by the other C25 subcategories. On a claim it identifies a malignant neoplasm of the pancreas, what clinical notes may record as carcinoma of the pancreas, at the neck or another qualifying site. This article covers the anatomical scope, code hierarchy, MS-DRG groupings, HCC mapping, documentation requirements, and the most common coding pitfalls for C25.7.
The ICD-10-CM tabular list includes one official “Applicable To” note under C25.7:
The neck is the short segment connecting the head and body of the pancreas, situated anterior to the superior mesenteric vessels. Clinicians and pathologists sometimes also document tumors of the uncinate process here when the site does not clearly belong to the head (C25.0). Coders should verify anatomical language in the operative or pathology report before assigning C25.7 to uncinate process tumors. When ambiguous, query the physician.
Ectopic pancreatic tissue is functioning pancreatic tissue found outside the normal gland, most often in the stomach, duodenum, or jejunum. When a malignancy arises in that tissue, the ICD-10-CM Neoplasm Table routes it to C25.7 under the “pancreas, ectopic tissue” entry rather than to a code for the organ where the tissue physically sits.
The practical rule is straightforward. If pathology names ectopic or aberrant pancreatic tissue as the origin of the malignancy, C25.7 is the site-specific code. Reserve C25.9 only for records where neither a named C25 segment nor ectopic tissue is documented. The AHA Coding Clinic has addressed this exact C25.7-versus-C25.9 decision for ectopic tissue cases.
Getting C25.7 right means knowing the full C25 family. Each subcategory maps to a distinct anatomical segment, so documentation specificity drives code selection.
C25.9 is a last resort. When clinical documentation identifies any of the specific sites above, use the most precise code. Defaulting to C25.9 on a chart that documents “neck of pancreas” creates an audit risk and may reduce HCC capture accuracy.
C25.9 is appropriate only when the treating physician has not documented a specific site and a physician query would be clinically unreasonable. If radiology, pathology, or operative notes name the neck, code C25.7. Using ICD-10 documentation guidelines to support site specificity protects reimbursement and risk-adjustment accuracy. According to the CMS ICD-10 coding guidance, coders must assign the code that reflects the highest level of specificity supported by the documentation.
C25.8 applies when a tumor explicitly spans two or more contiguous, named sites in the C25 family. A tumor described as involving “the neck and body” warrants C25.8, not C25.7. When documentation is ambiguous, coders should query the treating physician before assigning either code.
C25.7 groups into three MS-DRGs under version 43.0, with reimbursement determined by the presence or absence of complications and comorbidities (CC) and major complications and comorbidities (MCC).
Documenting secondary diagnoses that qualify as MCCs (such as sepsis, respiratory failure, or acute renal failure) shifts the encounter from DRG 437 to DRG 435, with a substantially higher geometric mean length of stay and reimbursement weight. Accurate secondary-diagnosis coding on these encounters has direct financial implications.
Run a monthly audit of C25.7 claims that landed in DRG 437. Cross-reference the clinical documentation for any secondary diagnoses that qualified as CC or MCC that were not coded. A single missed MCC on a pancreatic malignancy encounter can cost hundreds of dollars in lost reimbursement per case.
Under the CMS Hierarchical Condition Category (HCC) model, pancreatic malignancies carry significant risk-adjustment weight. C25.7 maps to HCC categories associated with severe cancers, which drive higher Risk Adjustment Factor (RAF) scores for Medicare Advantage and other risk-adjusted payment models.
According to CMS risk-adjustment education materials, pancreatic cancer codes including C25.7 fall under HCC 8 (Metastatic Cancer and Acute Leukemia) or HCC 9 (Lung and Other Severe Cancers), depending on whether metastatic disease is also documented. The distinction matters: HCC 8 carries a higher RAF coefficient than HCC 9, reflecting the greater resource utilization and cost burden of metastatic disease.
Use the HCC ICD-10 Crosswalk to verify the current-year HCC mapping for C25.7 against the applicable CMS model version, as HCC assignments can shift between model years.
Practices using claims management software with integrated diagnosis tracking can set alerts to flag C25.x encounters where metastatic codes may be missing, reducing the risk of undercoded HCC categories on RAF-sensitive patient panels.
Three source documents determine whether C25.7 is supportable: the operative report, the pathology report, and the treating physician’s clinical notes. Each has a different level of authority depending on the clinical setting.
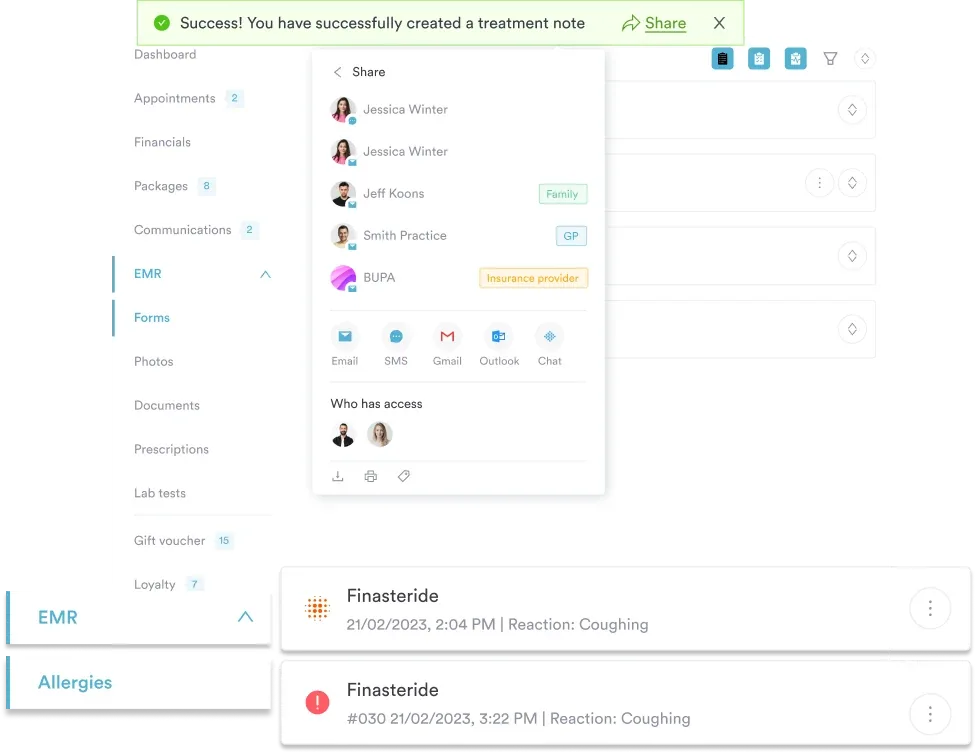
Maintaining HIPAA-compliant documentation practices means retaining the full clinical record to support ICD-10-CM code assignment during payer audits. Patient record management systems that timestamp physician entries and link pathology attachments directly to the encounter note reduce audit exposure substantially.
Outpatient encounters follow the ICD-10-CM Official Guidelines Section IV, which prohibit coding a confirmed malignancy from radiology findings alone without physician documentation of the diagnosis. Inpatient encounters follow Section II, where the coder may reference pathology and radiology if the attending physician has not contradicted those findings in the discharge summary. For C25.7, this means outpatient coders in oncology or gastroenterology practices should obtain a written diagnosis from the treating physician before assigning the code, even when the pathology is unambiguous.
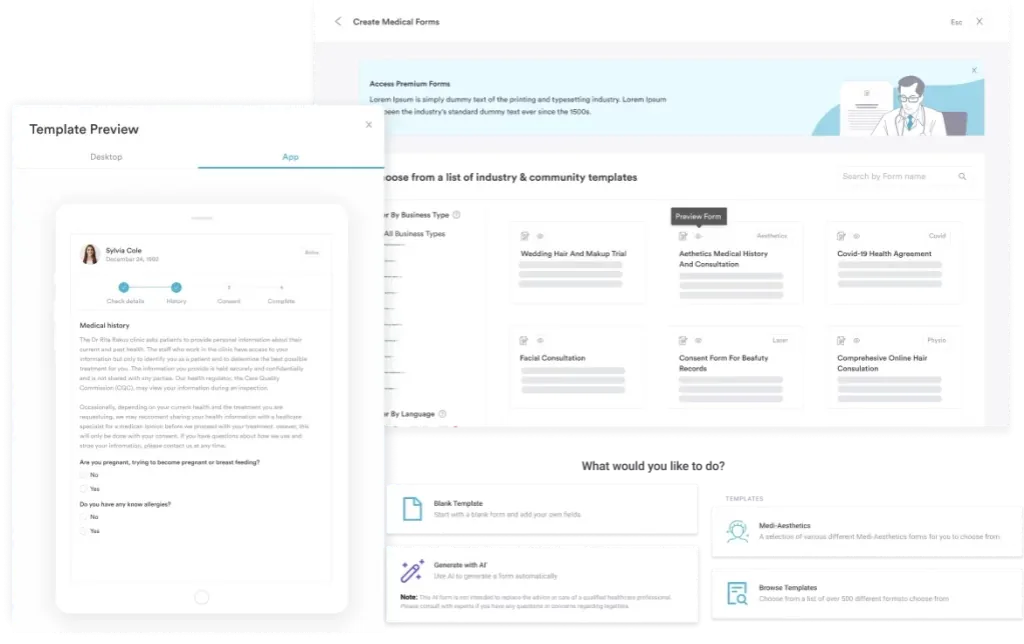
Streamlining this process through digital clinical forms that capture physician sign-off at the point of care reduces the documentation lag that leads to delayed coding and denied claims.
Pabau's claims management tools help oncology and gastroenterology billing teams track ICD-10 codes accurately, flag missing secondary diagnoses, and stay audit-ready across every encounter.

Pancreatic cancer coding attracts payer scrutiny because of its high reimbursement weight. These are the four patterns most likely to trigger a denial or an overpayment recoupment.
The most common error. When the pathology report reads “primary adenocarcinoma of the neck of the pancreas,” C25.9 is incorrect and C25.7 is the required code. Payers running clinical data analysis tools can identify high C25.9 rates against a backdrop of surgical and pathology claims that imply site specificity, flagging practices for coding accuracy reviews. Consistent use of ICD-10-CM code selection protocols tied to documentation review reduces this risk.
Coding neuroendocrine carcinoma of the pancreas is contested among coders. C25.4 (malignant neoplasm of endocrine pancreas) covers islet cell tumors and neuroendocrine tumors arising from endocrine cells. C25.7 applies when the neuroendocrine tumor’s anatomical site is the neck and the pathology does not specify an islet cell origin. Because this distinction is genuinely uncertain in some cases, the AHA Coding Clinic is the authoritative reference. Until official guidance is published, the safest approach is to query the treating physician when pathology reports describe a neuroendocrine carcinoma of the neck of the pancreas without further histological detail. Malignant, well-differentiated pancreatic neuroendocrine tumors are classified in category C7A (C7A.8), which carries an Excludes2 note for malignant pancreatic islet cell tumors (C25.4). Confirming differentiation and cell origin in the pathology report is what decides whether a case belongs in C25.4, C25.7, or C7A.8.
Pancreatic cancer frequently presents with hepatic or peritoneal metastases at diagnosis. When metastatic disease is documented, secondary malignancy codes (e.g., C78.7 for secondary malignant neoplasm of liver) must be coded alongside C25.7. Omitting them understates disease severity, reduces HCC capture, and misrepresents the clinical complexity that drives DRG assignment. EHR integration for billing workflows that flag metastasis-related diagnosis codes at encounter creation helps prevent this omission.
For practices handling pre-October 2015 records or cross-walking for research purposes, the predecessor ICD-9-CM code for C25.7 was 157.8 (Malignant neoplasm of other specified sites of pancreas). This crosswalk is one-to-one but should be verified for any legacy billing or retrospective analysis. The AAPC Codify ICD-10-CM lookup includes ICD-9 conversion tools for this purpose.
Flag all C25.x encounters in your practice management system for a secondary-diagnosis completeness review before claim submission. Build a checklist: (1) Is metastatic disease documented? Code secondary sites. (2) Is a complication present (biliary obstruction, malnutrition, pain)? Code it. (3) Is the anatomical site specific? Use C25.0-C25.7 before defaulting to C25.9.
The neck of the pancreas is a surgically significant location. Its proximity to the superior mesenteric artery and portal vein means tumors here are frequently borderline-resectable or unresectable at presentation, according to the National Library of Medicine’s clinical terminology resources and published oncology literature.
Clinically, pancreatic adenocarcinoma is the predominant histology across all C25.x codes. Neuroendocrine tumors are less common and behave differently: they tend to be slower-growing and more amenable to surgical resection. The distinction matters for coding because histology drives the secondary procedure and treatment codes that accompany C25.7 on a claim.
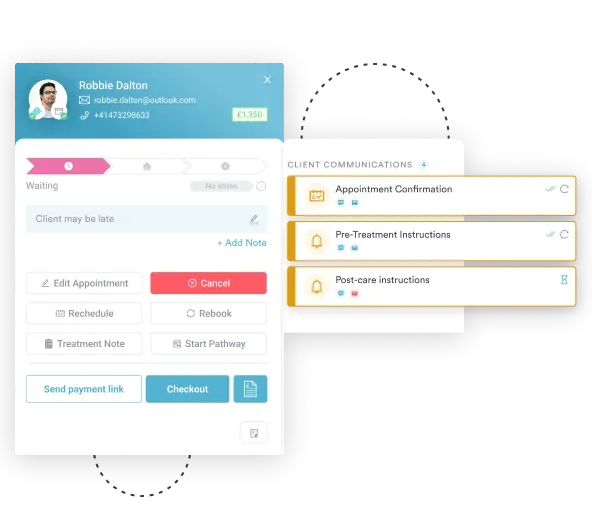
Practices managing oncology patients benefit from a structured automated workflow that routes new malignancy encounters through a coding review checkpoint before submission. This is particularly relevant for multi-specialty practices where a gastroenterologist initiates the diagnosis but surgical and oncology teams generate subsequent claims.
The WHO’s ICD-10 browser classifies C25.7 under Malignant neoplasms of digestive organs, providing the international coding framework that aligns with the U.S. ICD-10-CM adaptation maintained by the CDC/NCHS ICD-10-CM web tool.
Defaulting to C25.9 on a pancreatic cancer chart that clearly documents the neck as the tumor site is one of the most common and most costly coding errors in oncology billing. C25.7 is the correct, specific, billable code for that scenario, and using it accurately captures HCC risk scores, supports the right MS-DRG assignment, and withstands payer audits.
Pabau’s claims management software gives oncology and gastroenterology billing teams the tools to track secondary diagnosis completeness, flag under-coded malignancy encounters, and maintain the documentation audit trail that supports C25.x code accuracy. Book a demo to see how Pabau handles complex oncology billing workflows.
Need a structured framework for clinical documentation compliance? HIPAA compliance for medical offices covers the documentation requirements that support accurate diagnosis coding and audit defense.
Looking for guidance on managing intraparenchymal and other complex ICD-10 diagnoses? Intraparenchymal hemorrhage ICD-10 codes walks through another high-complexity diagnostic coding scenario with documentation and sequencing guidance.
Want to reduce billing errors across your oncology or gastroenterology practice? Practice management software explains how integrated platforms reduce claim errors and support complete secondary-diagnosis coding at scale.
ICD-10 Code C25.7 is the billable ICD-10-CM diagnosis code for malignant neoplasm of other parts of pancreas, including the neck of the pancreas. It is valid for HIPAA-covered transactions from October 1, 2024 and sits within the C25 (Malignant neoplasm of pancreas) category of the ICD-10-CM tabular list.
C25.7 officially includes the neck of the pancreas as an “Applicable To” inclusion. The uncinate process may also be coded here when it does not clearly belong under C25.0 (head), though this requires careful review of operative and pathology documentation and, where ambiguous, a physician query.
C25.9 is reserved for pancreatic malignancies where the specific anatomical site is not documented or cannot be determined. C25.7 must be used instead whenever the treating physician, pathology report, or operative notes identify the neck of the pancreas as the tumor location. Using C25.9 when site-specific documentation exists is a coding error.
Under MS-DRG v43.0, C25.7 groups into MS-DRG 435 (with MCC), MS-DRG 436 (with CC), or MS-DRG 437 (without CC/MCC). The assigned DRG depends on secondary diagnoses coded during the same inpatient encounter, making complete complication and comorbidity coding critical for accurate reimbursement.
This is a contested area. C25.4 covers endocrine pancreas tumors (islet cell origin), while C25.7 covers other anatomical sites including the neck. When pathology identifies a neuroendocrine carcinoma at the neck without specifying islet cell origin, query the treating physician and consult the AHA Coding Clinic for the most current guidance before assigning either code.
Yes. C25.7 is a billable, specific ICD-10-CM diagnosis code valid for HIPAA-covered transactions with a date of service on or after October 1, 2024. It has no child subcodes and can be submitted directly on claims without further specification.
Adenocarcinoma is the predominant histology across pancreatic malignancies, but ICD-10-CM codes the site, not the cell type. Assign the code for the documented location: C25.0 (head), C25.1 (body), C25.2 (tail), or C25.7 for the neck and other parts. There is no separate adenocarcinoma code, so the site drives selection.
Once treatment is complete and there is no evidence of active disease, use Z85.09 (personal history of malignant neoplasm of other digestive organs) instead of C25.7. C25.7 codes an active malignancy, so applying it to a treated, disease-free patient overstates the current condition on the claim.