CPT code 19357: Tissue expander placement in breast reconstruction
CPT code 19357 covers tissue expander placement plus every fill visit inside the...
Last Updated: August 3, 2026
Starting a dermatology practice requires at minimum six months of preparation before opening day, covering licensing, business entity formation, facility setup, and credentialing.
Your choice of specialty mix (medical, cosmetic, or surgical dermatology) determines your facility footprint, equipment budget, and patient acquisition strategy before you sign a lease.
Insurance credentialing and Medicare enrollment can take 90-180 days, so submit applications before construction or renovation begins to avoid revenue gaps at launch.
Pabau’s dermatology EMR software centralizes patient records, digital consent forms, before-and-after photos, and automated appointment workflows in one platform built for skin-focused practices.
Most dermatologists who leave employment underestimate how long the runway actually is. According to Dermatology Times, physicians should allow a minimum of six months of preparation before opening day – though in practice, most new dermatology offices need 9 to 18 months from serious planning to first patient. That six-month floor assumes you already know your specialty focus, your market, and your funding source. Factor in credentialing delays, build-out timelines, and equipment procurement, and the realistic window stretches closer to 12 months for a well-organized launch. This guide covers how to start a dermatology practice from the business plan through to your first patient appointment, with the specific decisions that separate practices that thrive from those that stall.
Whether you are a resident finishing training and weighing independence against employment, or an employed dermatologist ready to build something of your own, this guide walks through every major decision in sequence: business planning, licensing, facility design, technology, billing, and patient acquisition. Each section addresses the trade-offs specific to dermatology rather than repeating generic advice that applies to any medical specialty.
The business plan is not a formality for a bank loan. It is the document that forces you to answer questions most new practice owners avoid: Who exactly is your patient? What procedures will you perform in year one versus year three? What does your break-even look like at 15 patients per day versus 25?
Your first structural decision is the specialty mix. Medical dermatology, cosmetic dermatology, and surgical dermatology each carry different reimbursement profiles, equipment requirements, and patient demographics. A practice focused on insurance-reimbursed medical derm operates on higher volume with tighter margins. A cosmetic-heavy practice operates on lower volume with higher per-visit revenue and zero insurance dependency, but requires different marketing, a different physical space, and a patient base willing to pay out of pocket.
Your business entity choice carries tax, liability, and operational implications. Most dermatologists form a Professional Limited Liability Company (PLLC) or Professional Corporation (PC), though S-Corp elections are common for tax efficiency once revenue scales. This decision requires a healthcare attorney who understands your state’s corporate practice of medicine rules. Do not rely on a general business attorney here.
Startup costs vary significantly by market, specialty mix, and facility size. A solo medical derm practice in a suburban market typically requires between $250,000 and $500,000 to reach opening day, covering build-out, equipment, working capital, and initial staffing. A cosmetic-focused practice with laser equipment can run considerably higher. The U.S. Small Business Administration offers SBA 7(a) and 504 loan programs specifically suited to medical practice startups, and many physician-focused lenders offer unsecured practice loans to board-certified physicians without requiring collateral.
Before a single patient walks through the door, you need several layers of credentials and registrations in place. Missing any one of them delays your opening or creates compliance exposure from day one.
| Credential/Registration | Issuing Body | Typical Timeline |
|---|---|---|
| State medical license | State Medical Board | 60-90 days |
| DEA registration | Drug Enforcement Administration | 4-6 weeks |
| NPI Number (individual + group) | CMS / NPPES | 1-2 weeks |
| Medicare enrollment | Centers for Medicare and Medicaid Services | 90-120 days |
| Medicaid enrollment | State Medicaid agency | 60-120 days |
| Commercial insurance credentialing | Individual payers (BCBS, Aetna, etc.) | 90-180 days |
| ABD board certification | American Board of Dermatology | Pre-existing requirement |
The American Board of Dermatology requires completion of an accredited residency program and passage of board examinations before you can hold yourself out as a board-certified dermatologist. This is a pre-opening requirement, not something you pursue concurrently. What new practice owners consistently underestimate is the insurance credentialing timeline. Submitting your payer applications the day you sign a lease means you may be credentialed and ready to bill insurance within your build-out window. Submit six weeks after signing and you will likely open without the ability to bill your most common payers, creating a revenue gap that can stretch two to three months.
Submit your Medicare enrollment application (CMS-855I) and commercial payer credentialing applications on the same day you execute your office lease. The credentialing clock starts ticking the moment you submit, not the moment you open. Running these in parallel with your build-out is the single most effective way to prevent a revenue gap in your first 90 days.
OSHA compliance is a separate obligation. Dermatology practices that perform biopsies, injections, or any procedures involving sharps or bloodborne pathogens must maintain written exposure control plans, train staff annually, and document that training. The Occupational Safety and Health Administration enforces these requirements for medical offices regardless of practice size.
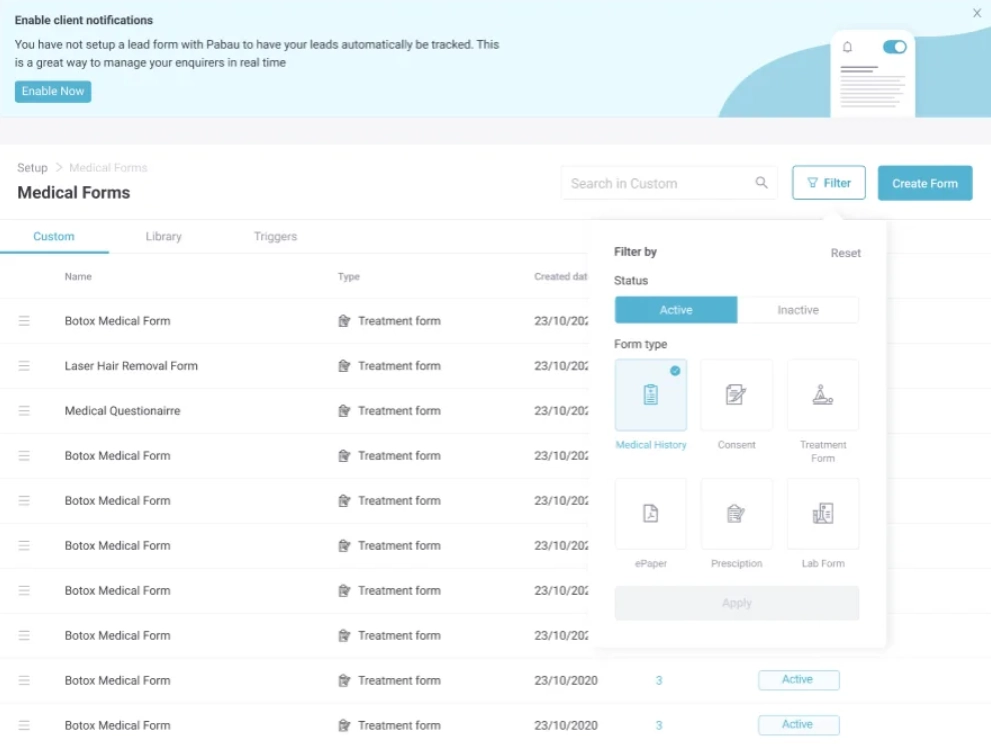
Patient-facing paperwork belongs on the same pre-opening checklist: line up a customizable dermatology consent form for each core procedure so you are not drafting risk disclosures the week you open.
Location decisions in dermatology are more nuanced than in general medicine. Patients with cosmetic concerns will travel to reach a trusted provider, making proximity less critical than reputation and parking. Patients seeking medical dermatology for chronic conditions often choose the nearest available appointment. Your specialty mix should drive your location decision, not the other way around.
A new practice can typically open with one to two exam rooms and scale from there. Each medical derm room can support roughly 8-10 patient slots per day with efficient scheduling. A surgical suite for Mohs procedures requires additional square footage, specialized lighting, and a procedure prep area. Cosmetic practices benefit from a separate consultation room where patients can review before-and-after photos in a private, unhurried setting, which meaningfully improves treatment conversion rates.
A solo dermatologist launching a new practice typically needs three to four clinical and administrative staff from day one. Trying to run a practice with fewer people usually creates a bottleneck at intake, checkout, or clinical prep that limits how many patients you can actually see.
Compensation benchmarks matter. Underpaying clinical staff in a competitive labor market creates turnover that costs more than a salary premium would have. For medical practice startups, staff retention in the first 12 months is a direct driver of patient experience and practice reputation.
The technology stack you choose at launch shapes your clinical workflows, your billing accuracy, and your patient experience for years. Switching EHR systems 18 months after opening is expensive, disruptive, and avoidable with the right upfront evaluation.
Dermatology has specific documentation requirements that general-purpose EHRs handle poorly. Skin lesion descriptions, body site mapping, dermoscopy image attachment, before-and-after photo management, and cosmetic treatment planning all require purpose-built functionality. A system that forces workarounds for these workflows adds documentation time per patient and creates audit risk when records are reviewed.
Pabau’s dermatology EMR software handles these requirements natively, including before-and-after photo management, digital intake and consent forms, injection plotting, and automated patient workflows from booking confirmation through post-treatment follow-up. For practices running both medical and cosmetic services, having a single platform that handles insurance billing alongside cash-pay cosmetic services eliminates the operational complexity of running two separate systems.
Beyond the EHR, your technology stack at launch should include an online booking system, automated appointment reminders (SMS and email), a patient portal for document collection, and integrated payment processing. Each of these can be sourced separately or consolidated into one of the top practice management software solutions. Consolidation reduces per-transaction costs and eliminates data reconciliation between systems, which is a common source of billing errors in the first year.
Telehealth is worth evaluating during setup rather than as an afterthought. Follow-up consultations for acne management, post-procedure check-ins, and prescription renewals are well-suited to video visits. Telehealth regulations vary by state, particularly around prescribing, so verify your state’s requirements before launching a virtual care component. Pabau includes integrated telehealth software that keeps virtual visits within the same patient record, avoiding the documentation gaps that occur when telehealth runs on a separate platform.
Pabau brings scheduling, digital forms, before-and-after photos, billing, and automated patient communications into one platform. No workarounds, no separate systems.

Dermatology billing is more complex than most primary care specialties. A single patient encounter may involve an evaluation and management code, a procedure code for a biopsy, and a pathology handling code, all billed together with specific modifier requirements. Getting this wrong costs revenue through undercoding, triggers audits through overcoding, and creates claim denials that take weeks to resolve.
The American Academy of Dermatology provides coding guidance through its practice management resources for member physicians. These are updated annually to reflect CMS changes and are far more reliable than generic billing guides. New practice owners should either hire a biller with specific dermatology experience or contract with a revenue cycle management company that specializes in dermatology rather than general medical billing.
Overhead management matters from month one. Industry benchmarks show that operating expenses vary widely by specialty mix. Medical dermatology practices that rely primarily on insurance reimbursement typically run overhead between 55% and 65% of net revenue, driven by higher staffing ratios, billing infrastructure, and claims processing costs. Surgical and Mohs-focused practices often achieve lower overhead percentages – sometimes closer to 40% – because per-procedure revenue is substantially higher. Cosmetic-heavy practices can also run leaner overhead because cash-pay procedures eliminate claims processing costs and payer contract fee schedules entirely. Track your overhead by category (staffing, facility, supplies, administrative) from the first month so you can identify where costs are drifting before they become structural problems.
Pabau’s claims management software integrates directly with patient records, reducing the manual re-entry that creates coding errors. For new practices without a dedicated biller, automated claim scrubbing before submission catches the most common denial triggers before they reach the payer.
Waiting rooms do not fill themselves. A new practice in a market with established dermatologists needs a deliberate patient acquisition strategy, not a general marketing plan. The channels that fill that gap fastest are mapped out in this guide to marketing a new dermatology practice.
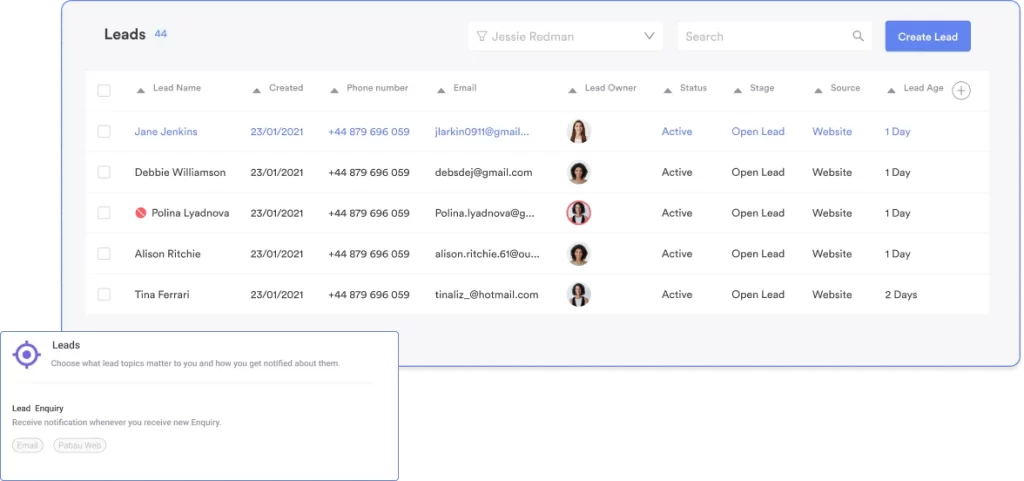
Referral relationships are the highest-value acquisition channel for medical dermatology. Primary care physicians, internal medicine, and pediatricians refer patients with skin concerns regularly, and they need a dermatologist they trust to respond quickly and communicate findings clearly. A structured outreach program to PCPs within a 10-mile radius in your first 90 days, combined with reliable referral loop communication (sending a note back after every referral visit), builds a referral engine that compounds over time.
Online presence drives patient acquisition differently for medical versus cosmetic practices. For medical derm, patients search for appointment availability and proximity. For cosmetic derm, patients search for specific treatments, read before-and-after content, and evaluate the provider’s aesthetic sensibility before booking. A cosmetic dermatology practice that does not invest in before-and-after documentation and social proof is leaving its most effective marketing channel unused. Pabau’s before-and-after photo tools make it easy to build this library systematically from every treatment visit.
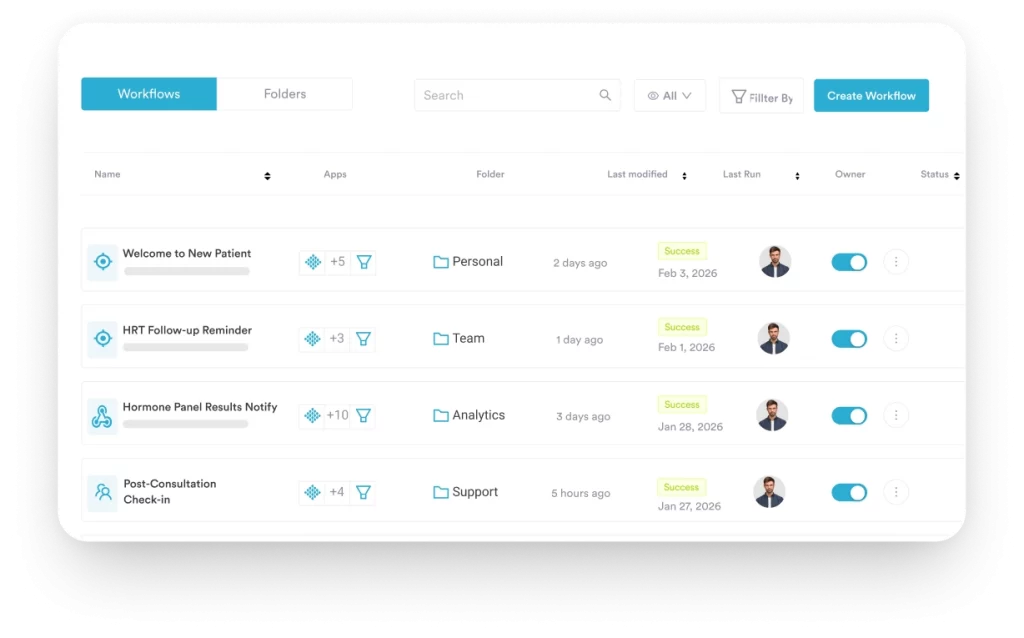
Patient experience drives retention and referrals more than any paid channel. Automated appointment reminders, pre-visit intake forms that patients complete from their phones, post-treatment care instructions delivered by SMS, and online review prompts sent at the right moment in the patient journey each contribute to a patient experience that generates organic word-of-mouth. Practices that rely on manual processes for these touchpoints do them inconsistently, which is why workflow automation becomes a revenue tool rather than just an efficiency tool. Each referral that comes from a satisfied patient costs nothing and converts at a far higher rate than any paid advertisement.
For practices pursuing a local SEO strategy, Google Business Profile optimization and a consistent review generation process are foundational. The review management features within Pabau send automated review requests after appointments, systematically building the online reputation that new patients use to evaluate providers they have never met.
Need a detailed guide for launching your medical practice? Starting a Medical Practice covers the business, legal, and operational steps relevant to any specialty launch.
Want to understand what your practice management platform should actually do? Practice Management Software: A Complete Guide breaks down every feature category and what to evaluate before you commit.
Building your dermatology patient acquisition engine? Patient Acquisition Strategies outlines referral, digital, and retention channels that work for clinical practices.
Opening a cosmetic dermatology practice and need a business plan framework? Medical Aesthetics Business Plan provides a structured template for aesthetic and cosmetic clinical practices.
Learning how to start a dermatology practice is ultimately a project management exercise with clinical stakes. The practices that open cleanly are those that ran their credentialing, facility setup, staffing, and technology decisions on parallel tracks rather than in sequence.
Pabau’s purpose-built dermatology EMR platform gives new practices the infrastructure to run clinical documentation, patient communications, booking, and billing from a single system, reducing the operational complexity that derails practices in their first year. If you’re setting up your technology stack now, book a demo to see how Pabau supports dermatology practices at every stage of growth.
A solo medical dermatology practice typically requires $250,000 to $500,000 to reach opening day (see the business plan section above for a full breakdown). Beyond those baseline figures, malpractice insurance adds $10,000 to $30,000 annually depending on your state and whether you perform Mohs surgery, which carries higher premium tiers. One cost category that catches new owners off guard is the credentialing gap – if you open before payer contracts are active, you may absorb 60 to 90 days of unreimbursed patient visits. Budget three to six months of working capital specifically to cover that window.
The credentialing table above covers the core requirements. Beyond those, watch for state-specific requirements that are easy to miss: some states require a separate facility license for any office performing surgical procedures, others mandate a specific CLIA waiver category if you run an in-office pathology lab, and states like California and New York have corporate practice of medicine rules that restrict how your business entity can be structured. Contact your State Medical Board early to get the full checklist for your jurisdiction rather than relying on a generic list.
The financial math depends heavily on your market. Before deciding, evaluate whether your target area can support another dermatologist by checking the dermatologist-to-population ratio (the national average is roughly 3.4 per 100,000 people). If your area is well below that, independent practice has a stronger demand-side case. If it is at or above, joining an established group may give you access to a patient panel that would take years to build independently. Also factor in that private equity consolidation has tightened referral networks in many metro markets, making it harder for solo practices to capture PCP referrals without an existing reputation.
Evaluate software by running a real patient scenario through each demo rather than comparing feature checklists. Document a simulated acne visit (E&M code, biopsy, pathology requisition), a cosmetic Botox appointment (consent form, injection mapping, cash-pay checkout), and a follow-up telehealth visit. The system that handles all three without workarounds or manual re-entry is the right fit. Pay particular attention to how each platform manages before-and-after photo storage, body site mapping, and mixed billing for practices that combine insurance and cash-pay services.
Most practices take 12 months from serious planning to first patient, with a realistic range of 9 to 18 months. The critical path is almost always insurance credentialing (90 to 180 days) running in parallel with facility build-out (60 to 120 days). If you are relocating to a new state, add 60 to 90 days for state medical licensure before you can even begin payer applications. The fastest launches happen when physicians start credentialing paperwork and lease negotiation simultaneously, ideally six to nine months before their target opening date.