Time Lapse Assessment Template
Download Your Free Time-Lapse Assessment Time-Lapse Assessment A comprehensive t...
March 30, 2026

Buy now, pay later is now available in Pabau
AMH levels interpretation helps clinics assess ovarian reserve, but a single result never tells the full fertility story
Normal AMH ranges from 1.2 to 5.0 ng/mL, though values decline naturally with age
Low AMH signals diminished ovarian reserve, not infertility, and natural conception remains possible
High AMH (above 5.0 ng/mL) may indicate PCOS and requires adjusted IVF stimulation protocols
Pairing AMH with antral follicle count and FSH gives clinics the most accurate picture of a patient’s reproductive potential
AMH levels interpretation is one of the most common tasks fertility clinics face daily. Anti-mullerian hormone (AMH) offers a window into a patient's ovarian reserve, helping practitioners plan treatment protocols, set realistic expectations, and guide conversations about reproductive timelines. But the numbers alone can be misleading without proper context. A single AMH result, taken in isolation, risks causing unnecessary panic in patients with low values or false confidence in those with high ones.
This guide breaks down AMH levels interpretation at every stage, how to read results accurately by age, and how your clinic can use these numbers to deliver better patient care.
Anti-mullerian hormone is a protein produced by the granulosa cells of developing ovarian follicles. Its concentration in the blood reflects the size of the remaining follicle pool, making it one of the most reliable biomarkers for ovarian reserve available today.
Unlike follicle-stimulating hormone (FSH), which fluctuates throughout the menstrual cycle and must be tested on specific days, AMH remains relatively stable cycle to cycle. That means your clinic can draw blood for an AMH test on any day of the cycle, which simplifies scheduling and reduces the back-and-forth that comes with cycle-dependent testing.
For fertility clinics, AMH testing serves several practical purposes:
It is worth noting that AMH measures quantity of remaining eggs, not quality. A patient with a low AMH can still conceive naturally if the eggs she does have are healthy. This distinction matters enormously when counselling patients on their results.
AMH levels decline naturally as women age, following a predictable downward trajectory. Understanding these age-stratified ranges is essential for accurate AMH levels interpretation in your clinic.
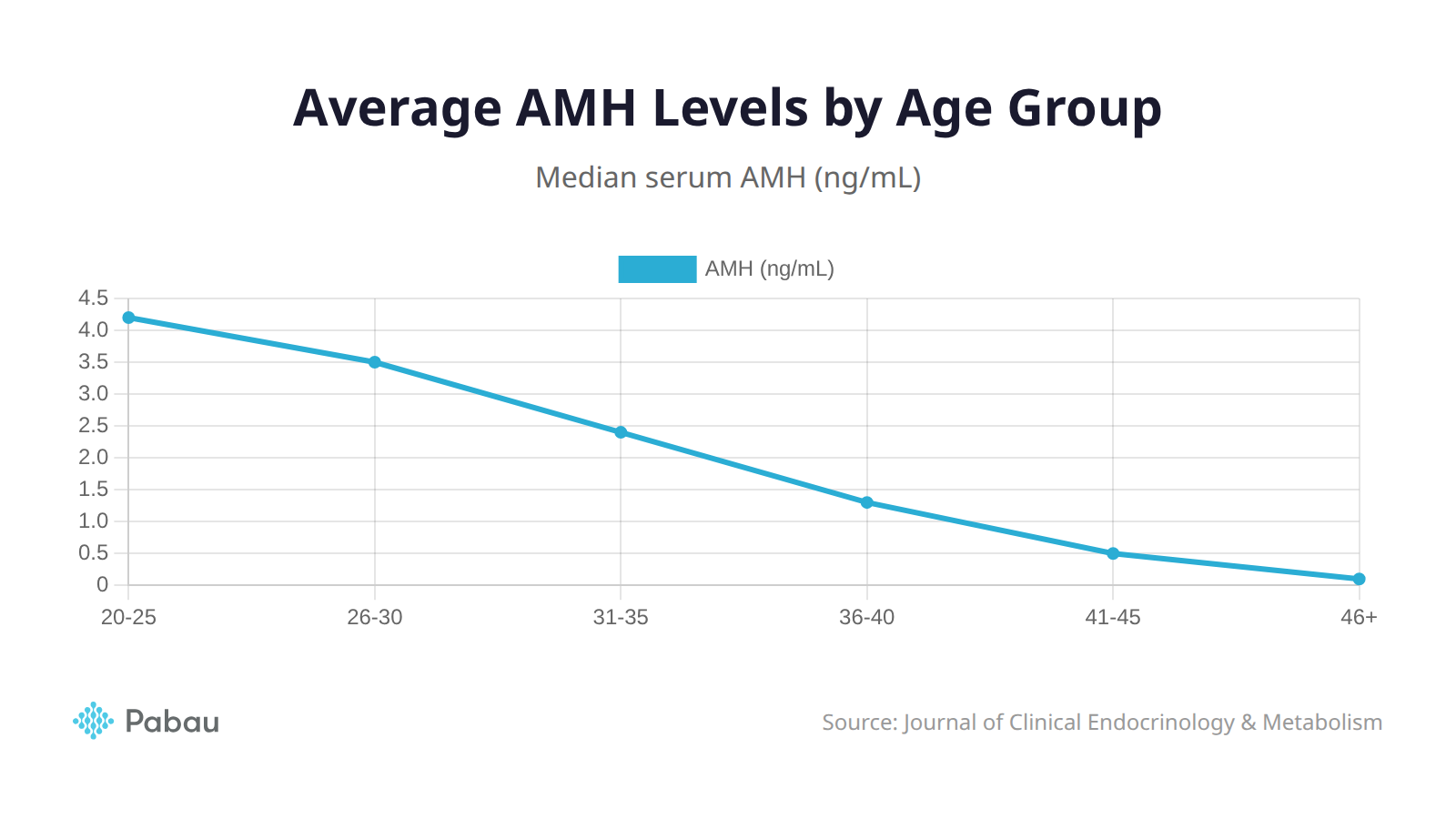
Accurate AMH levels interpretation starts with knowing what's normal for each age bracket. Here are the median AMH values by age group, based on data from large cohort studies including Iwase et al. (2024) published in the Journal of Obstetrics and Gynaecology Research:
| Age Group | Median AMH (ng/mL) | Clinical Interpretation |
|---|---|---|
| 20-25 | 4.2 | High reserve, peak reproductive years |
| 26-30 | 3.5 | Strong reserve, gradual decline beginning |
| 31-35 | 2.4 | Moderate reserve, closer monitoring advised |
| 36-40 | 1.3 | Lower reserve, treatment planning critical |
| 41-45 | 0.5 | Significantly reduced reserve |
| 46+ | 0.1 | Near-menopausal levels |
One critical point for clinicians: AMH exists on a continuum. The difference between 1.1 ng/mL and 0.9 ng/mL is clinically minimal, even though it might push a patient across a threshold in a reference table. As noted by Advanced Fertility Center of Chicago, these boundaries are guidelines, not hard cutoffs. Treating them as rigid categories can lead to over-interpretation and unnecessary patient distress.
Additionally, a large cohort study of 22,920 women found that the median AMH value drops below 1.2 ng/mL by age 36, reinforcing that age remains the strongest predictor of ovarian reserve decline.
When presenting AMH results to patients, avoid categorising their value as simply ‘low’ or ‘normal.’ Instead, show them where their number falls on the age-adjusted spectrum. Context reduces anxiety and builds trust.
Low AMH, generally defined as below 1.0 ng/mL (though this threshold shifts with age), indicates diminished ovarian reserve (DOR). For a 28-year-old, an AMH of 0.8 ng/mL is more clinically significant than the same reading in a 42-year-old, where it falls within the expected range.
What low AMH tells your clinic:
What low AMH does not mean:
For your clinical workflow, the priority when a patient presents with low AMH is to avoid catastrophising. Repeat testing after 2-3 months can confirm the result. Pairing AMH with an antral follicle count (AFC) on ultrasound gives a much more reliable composite picture. If both AMH and AFC are low, the clinical picture is clearer and treatment planning can proceed with greater confidence.
When documenting these results, standardised templates in your electronic medical records system help ensure consistency across your clinical team. Every practitioner should be recording AMH alongside AFC and FSH in a unified view.
High AMH, typically defined as above 5.0 ng/mL, is not always good news. While it suggests a large follicle pool, it is also strongly associated with polycystic ovary syndrome (PCOS), a condition affecting approximately 8-13% of women of reproductive age according to the World Health Organisation.
Clinical implications of high AMH:
High AMH does not guarantee better IVF outcomes. While more eggs may be retrieved, the quality of those eggs is influenced by age, genetics, and other factors that AMH does not measure. Clinics should resist framing a high AMH result as universally positive.
“Since switching to Pabau, we’ve been able to track patient biomarker results alongside treatment notes in one place. It has completely streamlined how we manage consultations and follow-up care for our patients.”

Integrating AMH testing effectively into your clinic's workflow requires more than just ordering a blood test. Here is how to get the most clinical value from every AMH result.
When to order AMH testing:
Pairing AMH with complementary markers:
Reliable AMH levels interpretation depends on context. The results become far more meaningful when combined with other data points:
Accounting for lab variability:
Different assay platforms (Elecsys, Access, picoAMH) can produce different absolute values for the same patient. Your clinic should ideally use the same lab and assay for serial testing to ensure results are comparable. When referencing published ranges, check which assay the reference data used.
Tracking AMH trends over time in your patient management software provides more clinical insight than any single snapshot. A patient whose AMH dropped from 2.5 to 1.2 ng/mL over 12 months is in a different clinical situation to one who has been stable at 1.2 for years.
Build an AMH result template in your EMR that auto-populates the reference range for the patient’s age group. This saves time during consultations and ensures every clinician on your team interprets results against the correct benchmark.
AMH levels interpretation is the easy part. The conversation that follows is where clinics truly add value.
Common patient reactions and how to handle them:
Practical counselling strategies:
Building standardised counselling workflows into your practice management system ensures every patient receives consistent, evidence-based information regardless of which clinician they see. Pre-built consent forms for fertility testing can also include educational content about AMH interpretation, setting expectations before results even arrive.
For clinics looking to go deeper on interpreting biomarkers without overpromising, the key is balancing honesty with hope. Patients need the truth, but they also need to hear about their options.
Struggling to keep patient records organised across your team? See the best EMR software for medical and aesthetic practices in 2026.
Want to improve how your clinic manages appointments and follow-ups? Explore patient scheduling software built for medical practices.
Looking for a system that handles CRM, records, and billing in one place? Healthcare CRM software could be the answer.
AMH levels interpretation can offer some clues about menopause timing, but it is not precise enough to give an exact date. Research suggests that very low AMH levels (below 0.2 ng/mL) may indicate menopause within the next 5-6 years, but individual variation is significant. AMH should be viewed as a general indicator rather than a countdown.
Hormonal contraceptives, particularly combined oral contraceptives, can suppress AMH levels by 20-30%. This means patients tested while on birth control may receive artificially low results. Most fertility specialists recommend testing AMH at least 2-3 months after discontinuing hormonal contraception for the most accurate reading.
AMH reflects the size of the remaining egg pool, which is largely determined by genetics and age. There is no strong evidence that diet, exercise, or supplements can increase AMH levels. However, maintaining overall reproductive health through a balanced diet, not smoking, and managing weight may support the quality of the eggs that remain.
For patients under active fertility monitoring or treatment, retesting every 6-12 months provides useful trend data. For patients not currently trying to conceive but interested in their reproductive timeline, annual testing from age 30 onwards gives a reasonable baseline. Avoid retesting within the same menstrual cycle, as short-term fluctuations are common.
Coverage varies widely by country and insurer. In the UK, AMH testing is available through the NHS as part of a fertility workup when referred by a GP, or privately for approximately £50-80. In the US, coverage depends on the patient's plan and whether infertility has been diagnosed. Clinics should advise patients to check with their insurer before testing to avoid unexpected costs.