Tebra Pricing in 2026: Modules, Add-Ons, and Real Costs
Most independent practices evaluating EHR software run into the same wall when t...
April 30, 2026

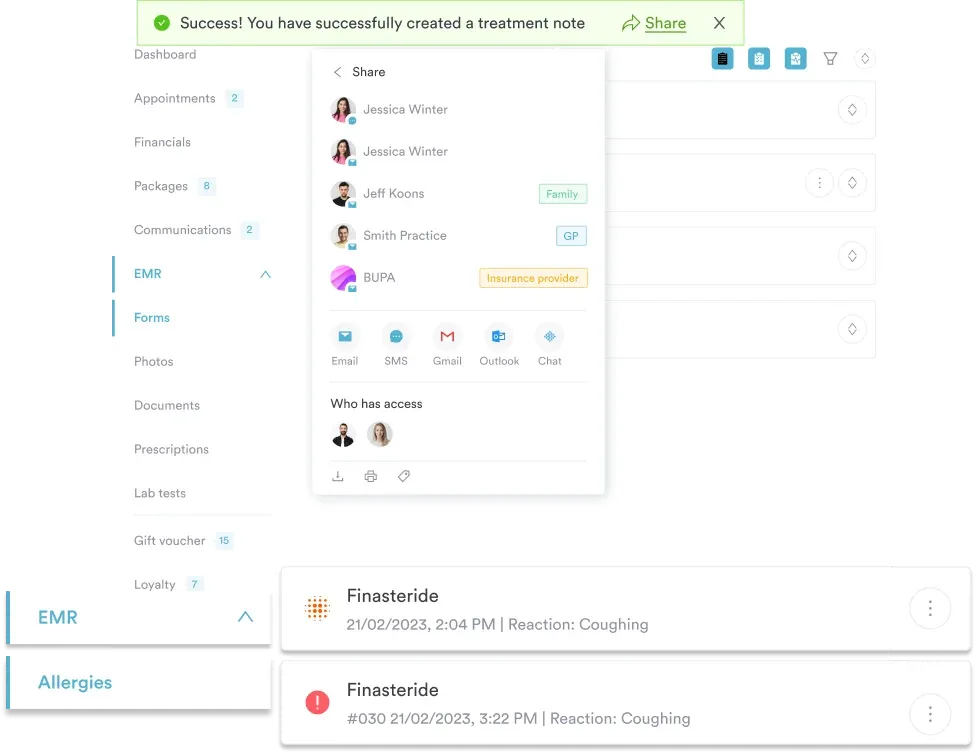
Buy now, pay later is now available in Pabau
EMRs store clinical data within a single practice
EHRs enable cross-provider data sharing and interoperability
Every EHR functions as an EMR, but not vice versa
EHRs support broader care coordination workflows
Practice size and specialty influence system choice
Electronic Medical Records (EMR) and Electronic Health Records (EHR) represent two distinct approaches to clinical documentation, yet the terms are often used interchangeably. The distinction matters for clinic operators evaluating systems: EMRs function as digital versions of paper charts within a single practice, while EHRs enable data sharing across multiple providers and healthcare settings. According to HealthIT.gov, the EMR term emerged first for clinical diagnosis and treatment, whereas “health” relates to the broader condition of being sound in body and mind.
This difference affects workflows, integration requirements, and operational decisions. A solo physiotherapy clinic tracking treatment progress may operate effectively with EMR functionality. A multi-location aesthetic practice coordinating care with referring physicians needs EHR capabilities.
Understanding which category your practice requires determines vendor selection, implementation costs, and long-term scalability. Because there are various types of EHR systems available today, the choice isn’t purely technical. It shapes how your team documents care, shares information, and manages patient relationships across the care continuum.
An EMR captures patient information generated within a single healthcare provider’s practice. It stores medical history, diagnoses, medications, immunisation records, laboratory results, and clinician notes. EMRs replace paper charts with searchable digital records, enabling practitioners to track patient data over time and identify when preventive care or screenings are due. These systems remain confined to the practice where the data originated – a physiotherapy clinic’s EMR doesn’t automatically share treatment notes with the patient’s GP.
EHRs expand beyond single-practice boundaries. They integrate information from multiple providers, creating a comprehensive view of a patient’s health across settings. When a dermatologist documents a skin cancer diagnosis in an EHR, the patient’s primary care physician can access that information immediately. EHRs support patient portals where individuals view their complete medical history, request prescription refills, and communicate with their care team. This interoperability defines the functional boundary between EMR and EHR systems.
The Elevance Health framework clarifies the distinction: EMRs capture information from a single care provider, available only to that provider. EHRs share complete information instantly across authorised users. This isn’t just theoretical – it affects how clinics exchange referral notes, coordinate treatment plans, and manage continuity when patients move between providers. A practice using EMR-only functionality may still need to fax records or print summaries for specialists, while EHR-enabled clinics exchange structured data electronically through practice management software integrations.
Every EHR is an EMR, but not all EMRs are EHRs. This hierarchy reflects technical architecture: EMR systems focus on clinical documentation within a closed environment, while EHRs add Health Information Exchange (HIE) capabilities. HIE infrastructure enables secure data transmission between disparate systems using standardised protocols. Without HIE integration, practices resort to manual data transfer – printing records, scanning documents, or re-entering information into multiple systems.
Interoperability operates on three levels. Foundational interoperability allows data transmission between systems without interpretation – one system sends a file, another receives it. Structural interoperability defines data field formats so receiving systems understand what each piece of information represents. Semantic interoperability ensures different systems interpret data identically – a blood pressure reading means the same thing regardless of where it was recorded. EHRs aim for semantic interoperability; many EMRs achieve only foundational exchange.
For clinic operators, this distinction manifests in integration complexity. A dermatology EMR might export PDFs to send via secure email, requiring manual re-entry at the receiving practice. An EHR-capable system pushes structured data through standardised interfaces, populating fields automatically in the recipient’s system. The Office of the National Coordinator for Health Information Technology (ONC) mandates interoperability standards for certified EHR systems, including adoption of USCDI Version 3 data standards and FHIR-based APIs effective January 2026. These certification requirements create a baseline for cross-platform data exchange that EMR-only systems don’t necessarily meet.
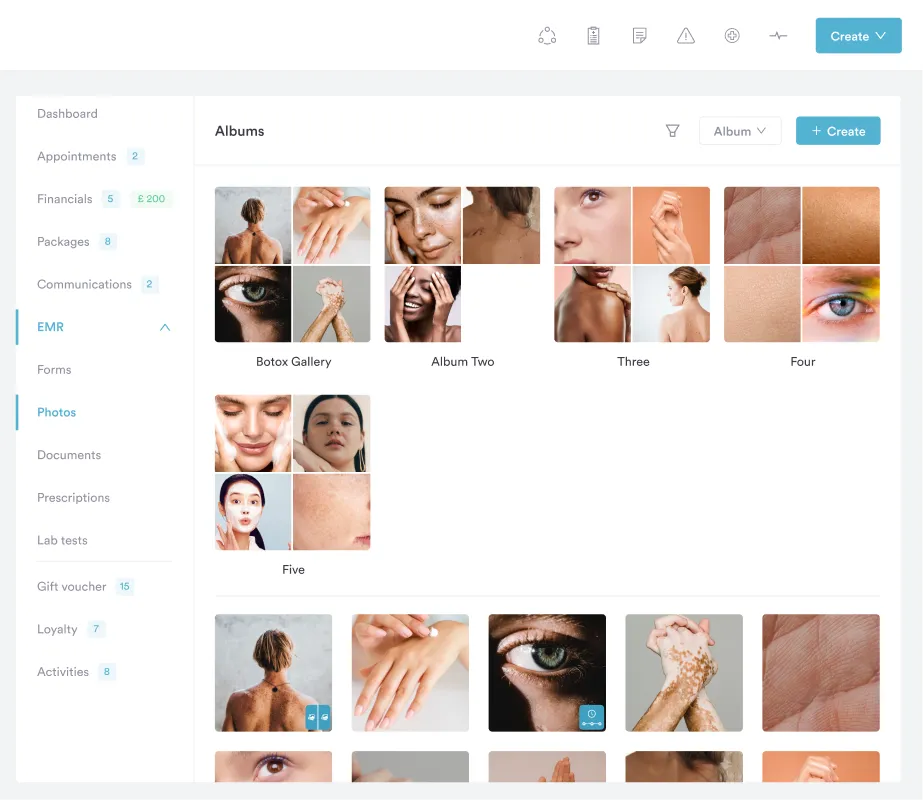
Solo practitioners and single-location clinics often operate effectively with EMR functionality. A boutique aesthetic clinic performing cosmetic procedures may never need to exchange structured clinical data with other providers. Their documentation requirements centre on treatment protocols, consent forms, before-and-after photography, and inventory management – functions an EMR handles without requiring external data exchange. The added cost and complexity of full EHR certification delivers marginal value when the practice operates as a contained ecosystem.
Multi-practitioner groups and specialties that rely on referrals benefit from EHR capabilities. A physical therapy practice receiving referrals from orthopaedic surgeons needs structured access to surgical notes, diagnostic imaging reports, and post-operative restrictions. An integrated care model – where GPs, specialists, and allied health providers coordinate treatment for chronic conditions – requires real-time data visibility across systems. These workflows justify the implementation costs and ongoing maintenance of certified EHR platforms.
Practice size affects vendor selection. Small practices with 1-3 clinicians may prioritise ease of use and lower subscription costs, accepting limited interoperability. Practices with 10+ providers across multiple locations typically require enterprise-grade EHR systems with robust integration capabilities, advanced reporting, and centralised administration. The Centers for Medicare & Medicaid Services (CMS) incentivises EHR adoption through its Promoting Interoperability Programs – formerly the Meaningful Use programme – which has distributed payments to nearly 550,000 healthcare providers since 2018. These incentives apply primarily to eligible professionals participating in federal reimbursement systems, making them less relevant for private-pay aesthetic or wellness clinics.
Pabau combines clinical documentation, patient records, and operational management in one platform. Book a demo to see how practices coordinate care without manual data transfer.

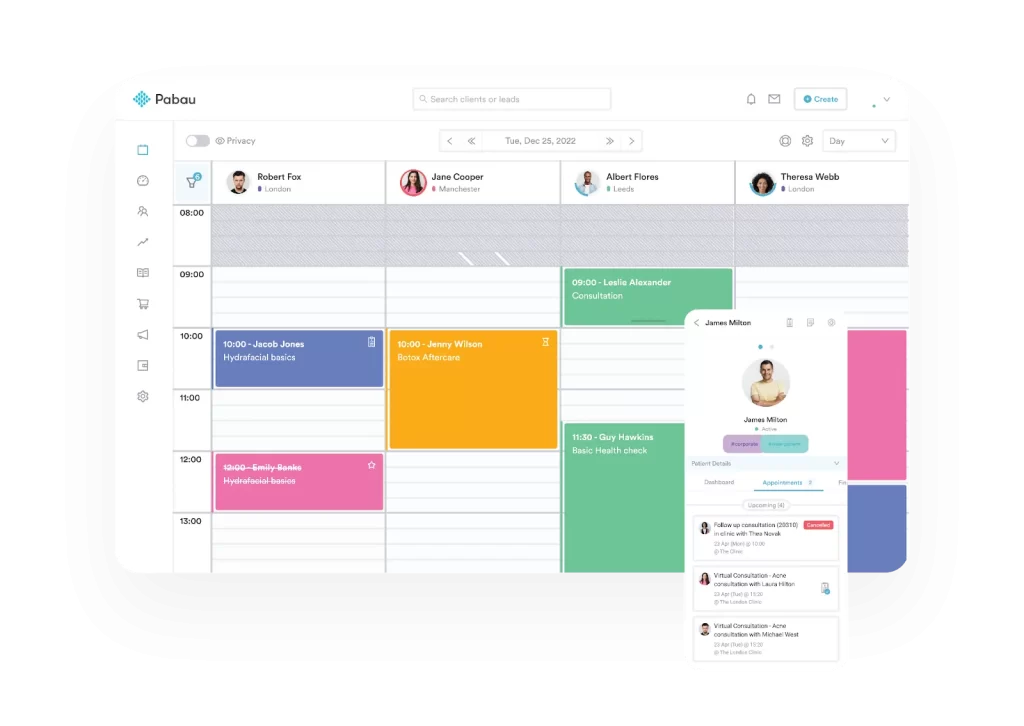
EMR systems optimise for clinical note-taking within a single practitioner’s workflow. Clinicians document patient encounters, record treatment plans, and track follow-up requirements without coordinating with external systems. An aesthetic nurse using an EMR records Botox injection sites, documents contraindications, and schedules follow-up appointments within their practice’s closed system. The workflow remains linear: patient check-in, treatment documentation, payment processing, and next appointment booking.
EHR workflows accommodate multi-provider coordination. A patient seeing both a dermatologist and an aesthetic practitioner for skin cancer follow-up requires bidirectional information flow. The dermatologist documents biopsy results and clearance for aesthetic procedures; the aesthetic practitioner notes treatment modifications based on medical history. This coordination happens through structured data exchange, not phone calls or faxed summaries. Digital intake forms populated with existing EHR data reduce redundant patient questioning and ensure consistent medical histories across encounters.
Documentation burden differs between systems. EMRs allow practice-specific templates and shortcuts tailored to a single workflow. EHRs must accommodate standardised data fields required for interoperability, sometimes forcing clinicians into structured formats that feel restrictive. A therapy practice using EMR functionality might create freeform progress notes matching their exact clinical approach. The same practice adopting certified EHR standards must use problem-oriented medical record formats, standardised terminology, and discrete data elements – increasing initial documentation time but enabling meaningful data exchange.
HIPAA applies to both EMR and EHR systems, mandating identical security standards for protected health information. Encryption, access controls, audit logging, and breach notification requirements don’t distinguish between system types. A practice storing patient records electronically must implement HIPAA-compliant safeguards regardless of whether they label their system EMR or EHR. The American Health Information Management Association (AHIMA) emphasises that data protection obligations remain constant across clinical documentation platforms, and that electronic documentation tools must have processes in place to ensure health information is valid, accurate, complete, and timely.
EHR certification introduces additional requirements. The ONC certifies systems meeting specific technical standards for data capture, interoperability, security, and clinical decision support. Certified EHR Technology (CEHRT) enables practices to participate in federal incentive programmes and demonstrates baseline functionality for meaningful use. Certification costs vendors significant development and testing resources, often reflected in higher subscription fees. Private practices not seeking federal incentives may avoid certification requirements by selecting EMR-only systems without ONC validation.
State-level regulations vary. Some jurisdictions mandate electronic prescribing capabilities that functionally require EHR features. Others specify data retention periods and patient access requirements affecting both system types. UK practices face General Data Protection Regulation (GDPR) obligations beyond HIPAA, requiring explicit consent for data processing and stronger patient data access rights. Compliance frameworks evolve faster than software development cycles, making vendor responsiveness to regulatory changes a critical selection factor.
Document your practice’s actual data exchange requirements before vendor selection. Track how many times monthly you need to send or receive clinical information from external providers. If that number exceeds 10-15 exchanges, full EHR capabilities justify the cost premium. Below that threshold, robust EMR functionality with secure messaging may suffice.
EMR implementation typically costs less than EHR deployment. A basic EMR system for a solo practitioner might run £50-200 monthly with minimal setup fees. The practice purchases licences, conducts limited staff training, and begins documenting within weeks. Data migration from paper charts or legacy systems requires manual entry but doesn’t involve complex interface mapping. Ongoing costs remain predictable: monthly subscriptions, occasional support tickets, and annual software updates.
EHR implementations demand greater investment. Enterprise systems with interoperability features cost £300-1,000+ monthly per provider, plus implementation fees ranging from £5,000-50,000 depending on practice size and integration complexity. Careful planning and strategy are crucial for a successful EHR implementation to minimize disruption and maximize clinical workflow efficiency. Connecting to Health Information Exchanges requires interface development, testing, and ongoing maintenance. Staff need extensive training on structured documentation, standardised terminology, and system workflows. A practice transitioning to a certified EHR should budget 3-6 months for full deployment, workflow optimisation, and ongoing EHR optimization to refine templates, integrations, and data exchange processes as the system matures.
Hidden costs emerge post-implementation. EMR-only systems require manual processes for external data exchange – staff time spent printing records, scanning incoming documents, and re-entering data from other providers. This operational overhead compounds as patient volume grows. EHR systems incur different costs: interface maintenance fees, HIE participation charges, and ongoing training as interoperability standards evolve. Neither approach is universally cheaper; the cost-benefit analysis depends on how frequently the practice exchanges clinical information and the value placed on automated coordination.
EMR systems serve single-location practices with contained workflows. Boutique aesthetic clinics, standalone spas, private counselling practices, and specialty providers operating independently function well with EMR capabilities. These practices document treatments, manage appointments, process payments, and track inventory without needing structured data exchange. A medical spa offering cosmetic injections, laser treatments, and skincare services doesn’t typically coordinate with external physicians – their clinical documentation remains internal.
EHR systems benefit integrated care environments. Multi-specialty groups, hospital-affiliated practices, accountable care organisations, and providers participating in coordinated care models require interoperability. A wellness clinic offering functional medicine, IV therapy, and preventive care while coordinating with patients’ primary care physicians needs bidirectional data flow. Physical therapy practices receiving referrals from orthopaedic surgeons and sports medicine physicians must access diagnostic reports, surgical notes, and treatment protocols – workflows that EMR-only systems handle through manual document exchange.
Growth trajectory influences system choice. A solo practitioner planning to remain independent might prioritise EMR simplicity and lower costs. That same practitioner anticipating practice expansion, potential mergers, or health system affiliation should evaluate EHR platforms early. Migrating from EMR to EHR post-implementation requires data conversion, workflow redesign, and staff retraining – disruptions avoided by selecting scalable systems initially. Research published in the Journal of Medical Internet Research confirms that despite advances in EHR technology over the past 25 years, implementation and adoption challenges persist, with benefits often falling below expectations during migration periods. Practices experiencing unplanned system migrations face 18-24 month productivity declines during transitions.
Evaluating integrated payment workflows? Payment Processing explores how clinical platforms handle transactions, deposits, and reconciliation alongside documentation.
Considering telehealth integration? Telehealth Software examines how virtual care capabilities affect EMR and EHR system requirements.
Need multi-location coordination tools? Multi-Location Management covers centralised administration for practices operating across multiple sites.
The EMR versus EHR decision hinges on interoperability requirements, not marketing labels. Practices operating as self-contained units – documenting care, managing appointments, and processing payments without external clinical coordination – function effectively with EMR systems. Those participating in referral networks, coordinated care models, or multi-provider treatment plans need EHR capabilities to avoid manual data transfer bottlenecks.
System selection should reflect current operations and anticipated growth. A solo aesthetic practitioner might start with EMR functionality and migrate to EHR-capable platforms as the practice expands. A new clinic planning rapid scaling or health system affiliations should invest in certified EHR systems initially. Neither approach is inherently superior – the right choice depends on how your practice exchanges clinical information, your patient population’s care coordination needs, and your operational priorities. Evaluate vendors by asking: how many external data exchanges do we handle monthly, what manual processes could automation eliminate, and what does structured interoperability actually enable for our specific workflows?
Hospitals use EHR systems because they coordinate care across multiple departments, specialties, and external providers. A hospital patient’s records must be accessible to emergency physicians, specialists, surgeons, and post-discharge care coordinators simultaneously. This requires interoperability features that EMR-only systems don’t provide.
Epic Systems operates as a comprehensive EHR platform with extensive interoperability capabilities. It enables data exchange across health systems, supports patient portals, and integrates with external laboratories, pharmacies, and referring providers. While Epic includes EMR functionality, its architecture and certification position it firmly as an EHR system.
EHR costs vary significantly by vendor, practice size, and feature requirements. Solo practitioners might spend £300-800 monthly for cloud-based EHR systems, while enterprise deployments for large practices can exceed £50,000 in implementation costs plus £1,000+ per provider monthly. Certified systems with advanced interoperability features typically cost more than basic EMR platforms.
EHR transitions require vendor selection, data migration planning, staff training, and workflow redesign. Start by documenting current processes and identifying integration requirements. Select a vendor offering implementation support and data conversion services. Plan for 3-6 months between contract signing and full system deployment, with reduced patient scheduling during the transition period to accommodate training and system testing.
EMR systems can operate nationally within a single practice or organisation, but they don’t automatically share data across unaffiliated providers without manual export and import processes. Multi-location practices using the same EMR platform access patient records across sites within their network. However, exchanging information with external providers requires manual document transfer unless the EMR includes EHR-level interoperability features.