Antisocial Personality Disorder Test
What is an Antisocial Personality Disorder Test? An antisocial personality disor...
April 6, 2026

Buy now, pay later is now available in Pabau
Psychiatry practice technology now centres on AI clinical documentation and measurement-based care integration
2026 telehealth billing rules stabilise remote psychiatric care reimbursement across most payers
Controlled substance prescribing requires EPCS certification and active PDMP integration for compliance
Practice profitability depends on credentialing strategy, accurate CPT coding, and workflow automation
Most psychiatrists see 15-25 patients weekly-sustainable caseload management prevents clinician burnout
Running a psychiatry clinic in 2026 demands operational precision across six domains: clinical documentation workflows, insurance credentialing timelines, controlled substance compliance, telehealth billing regulations, technology integration, and caseload sustainability. The Centre for Medicare & Medicaid Services (CMS) finalised long-term telehealth stability rules in late 2025, removing the temporary status that defined pandemic-era psychiatric care delivery. This shift creates predictable reimbursement structures but introduces stricter documentation requirements for remote patient monitoring and digital therapeutic tools.
Psychiatrists establishing or optimising practices face three operational challenges that distinguish this specialty from general mental health services. Controlled substance prescribing under Drug Enforcement Administration (DEA) oversight requires Electronic Prescribing for Controlled Substances (EPCS) certification and active Prescription Drug Monitoring Programme (PDMP) integration-infrastructure most therapy-focused practices never encounter. Insurance credentialing for psychiatric services takes 90-180 days longer than non-prescribing mental health providers due to malpractice verification and hospital affiliation checks. Finally, psychiatric billing workflows depend on accurate CPT code selection across evaluation, psychotherapy, and medication management combinations that therapy practices rarely navigate.
This guide addresses the operational realities psychiatrists encounter when building sustainable clinic operations. We examine practice management technology that automates documentation without sacrificing clinical accuracy, compliance frameworks that prevent DEA audit exposure, and staffing models that maintain 15-25 patient weekly caseloads without clinician burnout. Revenue optimisation strategies centre on credentialing efficiency, measurement-based care implementation, and billing accuracy-not patient volume expansion. By the end, you’ll understand how to structure a psychiatry clinic that delivers consistent clinical outcomes while maintaining operational profitability across regulatory changes.
State medical board licensing represents the first operational gate. Most jurisdictions require board certification or board eligibility in psychiatry, active malpractice coverage between £1-3 million per occurrence, and completion of state-specific jurisprudence examinations. Processing times range from 45-90 days for initial applications. Plan ahead-clinics cannot bill insurance or schedule patient appointments until licensing clears.
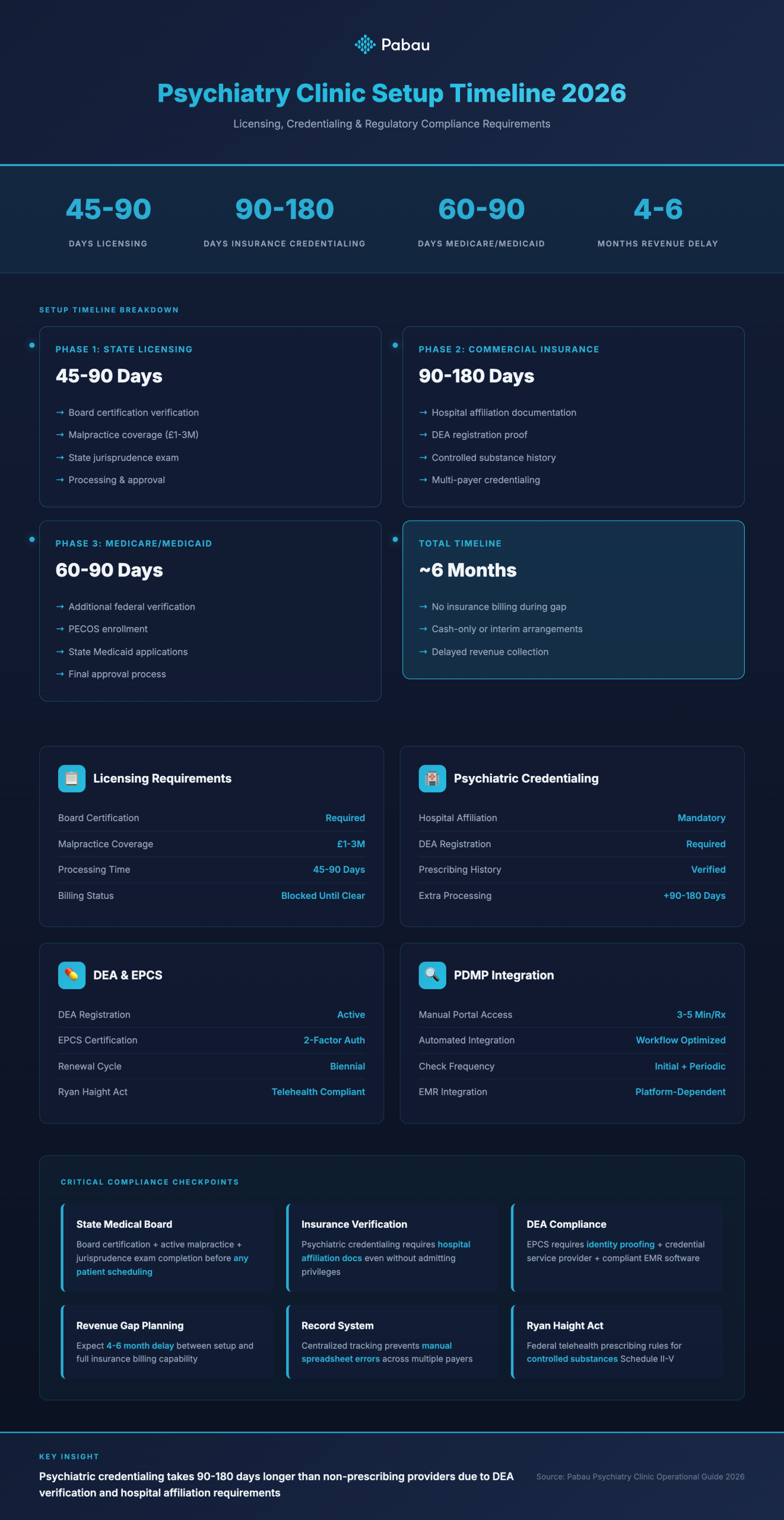
Insurance credentialing follows licensing but extends timelines significantly. Psychiatric credentialing requires additional verification steps beyond general practitioners: hospital affiliation documentation (even if you don’t admit patients), DEA registration proof, and controlled substance prescribing history. Commercial payers process psychiatric applications in 90-180 days. Medicare and Medicaid credentialing adds another 60-90 days. During credentialing gaps, clinics operate cash-only or use interim billing arrangements that delay revenue by 4-6 months. Centralised patient record systems help track credentialing status across multiple payers without manual spreadsheet updates.
DEA registration carries federal oversight that general therapy practices never face. Schedule II-V controlled substance prescribing requires active DEA registration, biennial renewal, and compliance with the Ryan Haight Act for telehealth prescribing. EPCS certification mandates two-factor authentication, identity proofing through a credential service provider, and software that meets DEA’s stringent security requirements. Not all psychiatric EMR systems include EPCS functionality-verify this before committing to a platform.
PDMP integration prevents controlled substance diversion and satisfies state monitoring requirements. Most jurisdictions mandate PDMP checks before initial controlled substance prescriptions and periodic reviews for ongoing patients. Manual PDMP portal access disrupts clinical workflow-automated PDMP queries within the prescribing interface save 3-5 minutes per prescription. Some EMR platforms offer direct PDMP integration; others require middleware services.
The Mental Health Parity and Addiction Equity Act requires insurers to cover psychiatric services at parity with medical/surgical benefits. However, payers frequently deny psychiatric claims for “medical necessity” when documentation lacks specific clinical detail. Claims denial rates for psychiatric services run 15-25% higher than primary care due to documentation gaps. According to CMS guidance, psychiatric notes must document symptom severity using standardised assessment tools, link treatment interventions to specific DSM-5-TR diagnoses, and justify service intensity through measurable functional impairment. Vague progress notes trigger automatic denials.
Measurement-based care (MBC) tools reduce denial rates by embedding objective symptom tracking into clinical documentation. PHQ-9, GAD-7, and YMRS scores provide quantifiable evidence of treatment necessity and response. Payers increasingly require MBC documentation for reimbursement-particularly for higher-intensity services like intensive outpatient programmes or collaborative care management. Clinics that integrate MBC into routine workflows report 18-22% fewer claim denials than those using narrative-only documentation.
See how Pabau streamlines controlled substance prescribing, PDMP integration, and insurance credentialing workflows in one platform-built for psychiatric practice compliance.

Electronic health record (EHR) selection determines daily workflow efficiency for psychiatric practices. Core requirements differ from general mental health EMRs: psychiatric EHRs must support complex CPT code combinations (e.g., 90833 + 90836 for psychotherapy with medication management), integrate with e-prescribing systems that meet EPCS standards, and accommodate measurement-based care tools without custom workarounds. Solo psychiatrists report spending 45-60 minutes daily on documentation tasks-systems that streamline note generation reclaim 12-18 hours weekly.
AI clinical documentation tools now offer real-time transcription during patient sessions. These systems capture spoken dialogue, identify clinically relevant content, and generate structured SOAP notes that align with billing requirements. Early adopters report 40-50% reduction in after-hours charting. However, AI-generated notes require clinician review-automated outputs sometimes miss context or insert incorrect diagnoses. AI-powered clinical note generation works best when configured with psychiatry-specific templates that prompt for DSM-5-TR criteria, safety assessments, and medication side effect monitoring.
CMS finalised permanent telehealth coverage for psychiatric services in December 2025, removing pandemic-era temporary flexibilities. Psychiatrists can now bill telehealth at parity with in-person visits for established patients, but new patient telehealth evaluations face geographic restrictions in some states. HIPAA-compliant telehealth platforms must include encrypted video transmission, waiting room functionality, and business associate agreements with the software provider.
Remote patient monitoring (RPM) billing codes now apply to digital therapeutic tools and symptom tracking apps. CPT codes 98975-98977 allow psychiatrists to bill for passive data collection and analysis of patient-generated health data. However, reimbursement requires at least 20 minutes of clinical review time monthly and documented treatment plan adjustments based on monitored data. Not all insurers reimburse RPM codes for psychiatric conditions yet-verify coverage before implementing monitoring programmes.
Measurement-based care extends beyond initial assessments. Effective MBC workflows administer validated instruments at intake, every 3-4 sessions during active treatment, and quarterly for maintenance phases. Automated MBC systems remind patients to complete assessments before appointments, flag symptom worsening for clinical review, and generate longitudinal outcome reports for treatment plan adjustments. Clinics that automate MBC administration report 65-70% patient completion rates versus 30-40% for manual paper-based systems.
Common psychiatric assessment tools include PHQ-9 for depression severity, GAD-7 for anxiety symptoms, MDQ for bipolar screening, and PCL-5 for PTSD monitoring. Selecting assessment tools depends on patient population-child psychiatry practices require paediatric-specific instruments like the SCARED for anxiety or the Vanderbilt for ADHD. EHR systems should calculate scores automatically, display results in clinical dashboards, and alert clinicians when scores cross clinical thresholds indicating crisis risk.
Build assessment completion into appointment check-in workflows. Patients complete MBC tools on tablets in the waiting room or via secure patient portals before sessions. This approach eliminates session time spent on paperwork and ensures consistent data capture without relying on patient recall during appointments.
Psychiatric billing complexity stems from CPT code combinations most practices never encounter. A single patient session might combine evaluation codes (90791, 90792), psychotherapy codes (90832-90838), and medication management add-ons (99354-99355 for prolonged services). Incorrect code pairing triggers automatic denials-for example, billing 90833 without a corresponding psychotherapy base code. According to American Medical Association (AMA) guidelines, psychiatric CPT codes follow strict hierarchical rules that determine which combinations insurers accept.
Claims submission accuracy depends on documentation specificity. Payers audit psychiatric claims at higher rates than other specialties-particularly for higher-value codes like 90838 (psychotherapy with medication management, 60 minutes). Superbills must specify session start time, end time, and clinical activities performed. Vague time documentation (“approximately 45 minutes”) increases audit risk. Automated claims management systems flag common billing errors before submission: missing diagnosis codes, incorrect modifier usage, and time-based code selection that doesn’t match session duration.
Initial psychiatric evaluations use CPT codes 90791 (without medical services) or 90792 (with medical services such as physical examination or prescription management). Code selection depends on whether the session includes medical decision-making beyond diagnostic interview. Follow-up psychotherapy sessions split into three time bands: 90832 (30 minutes), 90834 (45 minutes), and 90837 (60 minutes). Add-on codes 90833, 90836, and 90838 apply when psychotherapy includes medication management discussion.
Collaborative care management (CoCM) billing uses CPT codes 99492-99494 for integrated behavioural health services in primary care settings. CoCM requires at least 70 minutes of care coordination monthly, systematic outcome tracking using validated instruments, and psychiatric consultation to the primary care team. Psychiatrists participating in CoCM arrangements bill consultation time separately from direct patient contact-this model generates additional revenue streams beyond traditional fee-for-service psychiatry.
Prior authorisation requirements vary widely across insurers. Some payers require pre-approval for all outpatient psychiatric services beyond 6-8 sessions annually. Others restrict authorisation requirements to specific procedure codes like transcranial magnetic stimulation (TMS) or electroconvulsive therapy (ECT). Processing times range from 2-14 business days-clinics must submit authorisation requests before scheduling appointments to avoid patient access delays.
When payers deny claims, structured appeal processes recover 40-50% of initially rejected revenue. First-level appeals require clinical documentation that addresses the specific denial reason: missing diagnosis codes, insufficient medical necessity justification, or incorrect CPT code selection. Second-level appeals escalate to peer-to-peer clinical review-prepare a 10-15 minute case presentation highlighting DSM-5-TR diagnostic criteria, treatment response data from MBC tools, and evidence-based treatment rationale. According to CMS regulations, payers must respond to first-level appeals within 30 days and second-level appeals within 60 days.
Sustainable psychiatric practice operations balance clinician caseload against revenue requirements. Most psychiatrists maintain 15-25 active patients weekly to prevent burnout while meeting productivity targets. Session scheduling determines daily patient volume: back-to-back 30-minute medication management appointments generate higher hourly revenue than 60-minute psychotherapy sessions but increase documentation burden. Mixed scheduling models alternate between brief medication checks and longer therapy sessions-this approach maintains clinical variety while optimising revenue per clinical hour.
Appointment booking systems should automate three operational workflows: new patient intake screening, returning patient self-scheduling, and cancellation waitlist management. New patients complete intake questionnaires, insurance verification, and consent forms before their first session-this pre-visit preparation reduces administrative time during clinical appointments. Patient self-scheduling portals allow established patients to book follow-up sessions without staff intervention, reducing phone call volume by 60-70%. Waitlist functionality automatically contacts patients when earlier appointments become available through cancellations.
Solo psychiatric practices require at least one full-time administrative staff member for every 20-25 patients seen weekly. Administrative responsibilities include insurance verification, appointment scheduling, billing submission, and patient communication. Some psychiatrists outsource billing to revenue cycle management companies that charge 5-8% of collected revenue-this model eliminates in-house billing staff costs but reduces revenue margin.
Group practices introduce care coordination complexity. Multi-provider schedules require centralised appointment management, shared clinical protocols, and cross-coverage arrangements for urgent patient needs. Team management systems track provider availability, patient assignment, and clinical handoffs when patients see multiple clinicians. Practices with 3-5 psychiatrists typically employ one practice manager, one billing specialist, and one intake coordinator-this staffing ratio supports 60-80 patient encounters weekly across all providers.
After-hours documentation represents the largest controllable time drain in psychiatric practice. Psychiatrists spend an average 90-120 minutes daily completing clinical notes, responding to patient messages, and reviewing lab results outside scheduled appointments. Structured note templates reduce charting time by 30-40% compared to free-text documentation. Templates prompt clinicians for required elements-mental status examination findings, suicide risk assessment, medication side effects-without forcing rigid narrative structure.
Voice dictation tools allow clinicians to complete notes during or immediately after sessions. Real-time dictation captures clinical observations while fresh, reducing recall errors that occur when charting hours later. Some psychiatrists dictate brief clinical bullets during sessions, then expand notes with contextual detail in the final 5-10 minutes of the appointment slot. This hybrid approach maintains patient engagement while documenting key clinical data before memory fades.
Block 15-minute administrative periods between every 3-4 patient appointments. Use these intervals to complete documentation for recent sessions, return patient phone calls, and review upcoming appointment preparation needs. Scheduled admin time prevents evening documentation backlog and maintains separation between clinical and personal time.
Psychiatric patient engagement extends beyond appointment attendance. Effective engagement systems facilitate medication adherence monitoring, crisis intervention pathways, and between-session symptom tracking. Secure messaging platforms allow patients to report medication side effects, request prescription refills, and communicate non-urgent clinical updates without scheduling full appointments. However, unstructured patient messaging creates documentation burden-clinics must log all clinical communications in patient records for medicolegal protection.
Automated appointment reminders reduce no-show rates by 40-50%. Text message reminders sent 48 hours and 24 hours before scheduled appointments generate higher attendance than email or phone call reminders. Reminder content should include appointment date, time, clinician name, and check-in instructions. Some practices include brief pre-appointment questionnaires in reminders-patients rate current symptoms on 1-10 scales, flag medication concerns, and note any acute stressors requiring session time.
Psychiatric practices require documented crisis response protocols. Patients experiencing acute suicidal ideation, psychotic symptoms, or medication adverse reactions need immediate clinical guidance outside scheduled appointment times. After-hours coverage models include: on-call clinician rotation among group practice providers, contracted crisis line services, or automatic redirection to emergency departments for specific symptom presentations.
Patient portals should clearly display crisis contact information separate from routine appointment scheduling. Prominent messaging like “If you are experiencing a mental health emergency, call 999 (UK) or 988 (US) immediately” prevents patients from using non-urgent communication channels during crises. Some practices integrate crisis risk screening into patient portal login-brief safety questions trigger immediate clinical alerts when patients endorse acute risk.
Medication non-adherence accounts for 30-50% of psychiatric treatment failures. Monitoring systems track prescription refill dates, flag missed refills, and prompt clinical outreach when patients don’t collect medications on schedule. Electronic prescribing platforms provide refill history data-clinicians can identify adherence gaps during appointments and address barriers like cost concerns, side effect intolerance, or forgetfulness.
Automated refill request workflows reduce administrative burden. Patients submit refill requests through secure portals, pharmacy systems send refill notifications to prescribers, and clinicians approve routine refills without phone tag. For controlled substances, refill workflows must include additional verification steps: confirming recent appointments, checking PDMP data, and documenting clinical rationale for continued prescribing. Centralised prescription management systems maintain controlled substance logs, track DEA reporting requirements, and flag patients due for medication reviews.
Psychiatry clinic marketing differs fundamentally from general medical practice promotion. Direct-to-consumer advertising faces ethical constraints-aggressive marketing of psychiatric services risks exploiting vulnerable populations. Instead, professional reputation, referral network development, and educational content drive sustainable patient acquisition. Most new psychiatric patients arrive through three channels: primary care physician referrals (40-50%), existing patient word-of-mouth (25-30%), and online search for specific treatment needs (20-25%).
Primary care referral relationships require consistent communication. Send consultation notes to referring physicians within 24-48 hours of initial evaluations. Provide treatment recommendations, medication rationale, and follow-up plans that integrate with the patient’s overall medical care. Physicians refer to psychiatrists who respond promptly, communicate clearly, and accept new patients without months-long waitlists. Some psychiatrists offer reserved appointment slots for urgent referrals from key referring practices-this arrangement builds referral loyalty by solving the access problem most primary care physicians face when seeking psychiatric consultation.
Professional websites serve as credibility markers rather than lead generation tools. Patients research psychiatrists online before booking appointments-clinic websites should display credentials, treatment philosophy, accepted insurance plans, and new patient availability. Avoid generic stock imagery and marketing language. Instead, use straightforward descriptions of services offered: medication management for depression and anxiety, ADHD evaluation and treatment, bipolar disorder care, psychotherapy modalities offered.
Educational blog content positions psychiatrists as subject matter experts. Write practical guidance on topics patients actively search: “When to consider medication for anxiety,” “ADHD medication options for adults,” “Understanding bipolar disorder treatment stages.” Content that answers specific clinical questions ranks higher in search results than generic mental health information. Integrated marketing automation tools can schedule blog posts, track content performance, and connect website traffic to appointment booking patterns.
Insurance panel participation decisions determine patient access and revenue structure. In-network psychiatrists receive lower per-session reimbursement but attract higher patient volume through insurer referral directories. Out-of-network practices charge higher self-pay rates but limit patient access to those who can afford $200-400 per session. Mixed models participate with select high-volume commercial payers while remaining out-of-network for others.
Evaluate panel participation based on three factors: reimbursement rates relative to self-pay fees, administrative burden of credentialing and claims submission, and patient demographic alignment. If most potential patients in your service area carry specific insurance plans, in-network participation expands access. However, some insurers reimburse psychiatric services at rates 40-50% below self-pay market rates-accepting those contracts reduces revenue per clinical hour. Most psychiatrists maintain panels with 3-5 major commercial insurers plus Medicare, avoiding payers with consistently low reimbursement or high administrative friction.
Need structured assessment tools for clinical workflows? Psychiatric Evaluation Template provides a step-by-step framework for comprehensive psychiatric assessments with integrated DSM-5-TR criteria.
Setting up telehealth for psychiatric practice? Telehealth Software explains HIPAA-compliant video consultation requirements, remote patient monitoring integration, and documentation standards for virtual psychiatric care.
Building compliance workflows for controlled substance prescribing? Prescription Management Software details EPCS certification requirements, PDMP integration options, and DEA reporting automation for psychiatric practices.
Running a psychiatry clinic in 2026 requires operational precision across clinical, regulatory, and financial domains. Technology integration streamlines documentation workflows, but only when configured with psychiatry-specific templates and controlled substance compliance features. Insurance credentialing timelines extend 3-6 months longer than therapy-focused practices due to DEA verification and malpractice review requirements-plan cash flow accordingly during startup phases.
Sustainable practice models prioritise clinician wellbeing alongside revenue targets. Maintaining 15-25 patient encounters weekly prevents burnout while generating sufficient income when combined with efficient billing practices and accurate CPT code selection. Measurement-based care implementation reduces claim denials by 18-22% through quantifiable clinical documentation that satisfies payer medical necessity requirements. Automated appointment reminders, self-scheduling portals, and structured crisis protocols reduce administrative burden while improving patient engagement metrics.
The practices that thrive operationally master three elements: clinical technology that automates documentation without sacrificing accuracy, compliance systems that prevent DEA audit exposure, and billing workflows that maximise reimbursement through proper code pairing and appeal processes. Focus operational development on these domains before expanding patient volume or adding providers. A well-structured solo practice generates more consistent revenue than a poorly managed group practice with three psychiatrists.
The best psychiatric EHR includes EPCS certification for controlled substance prescribing, integrated PDMP access, MBC tool administration, and CPT code pairing validation. Solo psychiatrists should prioritise systems that automate documentation workflows, support telehealth delivery, and provide claims scrubbing before submission to prevent billing errors.
Psychiatrists most commonly use CPT codes 90791/90792 for initial evaluations, 90834 and 90837 for psychotherapy sessions, and add-on codes 90836/90838 when sessions include medication management. Collaborative care management uses CPT codes 99492-99494 for integrated behavioural health services in primary care settings.
AI clinical documentation tools reduce charting time by 40-50% for early adopters. Psychiatrists typically spend 45-60 minutes daily on documentation-AI transcription and structured note generation can reclaim 12-18 hours weekly. However, all AI-generated notes require clinician review before finalisation to ensure clinical accuracy.
Some psychiatric EHR systems offer direct PDMP integration that automatically queries state prescription monitoring databases during the prescribing workflow. Others require middleware services or manual PDMP portal access. Automated PDMP integration saves 3-5 minutes per prescription and ensures compliance with state monitoring requirements.
Psychiatrists can prescribe most controlled substances via telehealth under the Ryan Haight Act, provided they have an active DEA registration and follow state-specific telehealth prescribing rules. Some states require at least one in-person evaluation before initiating controlled substance prescriptions, while others allow fully remote prescribing for Schedule III-V medications.
CMS finalised permanent telehealth coverage for psychiatric services in December 2025, removing pandemic-era temporary flexibilities. Psychiatrists can now bill telehealth at parity with in-person visits for established patients, but new patient telehealth evaluations face geographic restrictions in some states. Remote patient monitoring codes (98975-98977) now apply to digital symptom tracking tools when combined with at least 20 minutes of clinical review monthly.