Closed vs Open Reduction: Clinical Comparison Guide
Closed vs Open Reduction: Clinical Comparison at a Glance Fracture reduction rep...
March 5, 2026
Discover free eBooks, guides and med spa templates on our new resources page

Buy now, pay later is now available in Pabau
Read case studies from our satisfied clients
Compare Pabau with alternative systems

Learn why this holistic care and aesthetic medicine clinic chose Pabau to power patient care and performance.
Read moreClosed reduction manipulates fractures externally without incision; open reduction requires surgical exposure
Closed techniques have lower infection risk but limited visualisation of fracture alignment
Open reduction with internal fixation (ORIF) provides direct anatomical reduction and stable fixation
CPT codes differ significantly: 27766 for closed treatment vs 27792 for open treatment of tibial shaft fractures
Recovery timelines vary based on fracture complexity, patient factors, and fixation method chosen
Fracture reduction represents one of the most fundamental decisions in sports medicine and orthopedic practice. Closed reduction manipulates bone fragments through intact skin using manual techniques and fluoroscopic guidance. Open reduction surgically exposes the fracture site to achieve direct visualisation and anatomical alignment. Both techniques serve distinct clinical roles based on fracture pattern, soft tissue injury, and patient-specific factors.
The choice between closed and open reduction determines patient outcomes, infection risk, rehabilitation protocols, and healthcare costs. According to the American Academy of Orthopaedic Surgeons (AAOS), appropriate technique selection reduces complications by 40% compared to mismatched interventions. Understanding the clinical, operational, and coding differences between these approaches helps orthopedic practices deliver evidence-based care while maintaining documentation accuracy.
This guide compares closed reduction versus open reduction across technique mechanics, clinical indications, recovery protocols, complication profiles, and billing workflows. Whether you manage an orthopedic physical therapy clinic coordinating post-reduction rehabilitation or an outpatient surgical centre performing definitive fracture care, these distinctions shape daily clinical decisions.
Closed reduction relies on external manipulation of bone fragments without surgical incision. The practitioner applies longitudinal traction, angular correction, and rotational alignment while monitoring fluoroscopic images in real time. Success depends on the surgeon’s tactile feedback, radiographic interpretation, and understanding of fracture biomechanics. The technique preserves the periosteal blood supply and soft tissue envelope, which accelerates healing in appropriately selected cases.
Open reduction surgically exposes the fracture site through a carefully planned incision. Direct visualisation allows anatomical reduction of articular surfaces, removal of interposed soft tissue, and precise placement of internal fixation devices. Plates, screws, rods, or pins stabilise the fracture in the corrected position. This approach achieves superior alignment for complex fracture patterns but introduces surgical trauma, infection risk, and prolonged operative time.
The fundamental trade-off between these techniques balances soft tissue preservation against alignment precision. Closed reduction minimises tissue disruption but accepts slightly less anatomical accuracy. Open reduction internal fixation (ORIF) maximises alignment control but increases biological cost. According to NICE guidance on fracture management, technique selection should follow a risk-benefit analysis incorporating fracture geometry, patient comorbidities, and functional expectations.
The closed reduction sequence begins with adequate anesthesia – local hematoma blocks for simple fractures, procedural sedation for more complex reductions, or general anesthesia when muscle relaxation is required. Longitudinal traction overcomes muscle spasm and disengages fracture fragments. Angular and rotational forces recreate the deforming mechanism in reverse, allowing fragments to interdigitate into acceptable alignment.
Fluoroscopy confirms reduction quality in orthogonal planes. Acceptable alignment parameters vary by anatomic location: diaphyseal fractures tolerate minimal angulation, metaphyseal regions allow more deformity based on remodeling potential, and articular surfaces demand near-anatomical restoration. Following reduction, the limb is immobilised in a cast, splint, or brace that maintains alignment while soft tissues heal.
Open reduction proceeds through surgical exposure that balances adequate visualisation against soft tissue preservation. Surgeons select approaches that avoid neurovascular structures while providing access to the fracture zone. Once exposed, fracture hematoma is irrigated, interposed periosteum or muscle is removed, and bone fragments are reduced under direct vision.
Internal fixation devices stabilise the reduction. Compression plates apply interfragmentary compression that enhances primary bone healing. Bridge plates span comminuted zones while preserving blood supply. Intramedullary nails provide load-sharing fixation for diaphyseal fractures. Screw configurations vary based on fracture pattern – lag screws compress oblique fractures, while positional screws maintain reduction without compression. The choice of implant and fixation strategy follows AO principles established through decades of biomechanical research.
Fracture characteristics drive technique selection more than any other variable. Simple, extra-articular fractures with acceptable alignment after closed manipulation rarely require surgery. Complex patterns with displacement, comminution, or intra-articular extension often demand open reduction to restore anatomy and function.
Closed reduction works best when the fracture geometry allows stable positioning without internal fixation. Metaphyseal impaction, intact periosteal hinge, or minimal soft tissue interposition predict successful non-operative management. According to research published in the Journal of Orthopaedic Trauma, closed reduction achieves union rates exceeding 95% for appropriately selected simple fracture patterns.
The decision for open reduction often involves fracture-specific algorithms. Tibial plateau fractures with joint depression exceeding 3mm undergo ORIF. Distal radius fractures with dorsal angulation over 20 degrees or intra-articular step-off typically require surgical correction. Femoral shaft fractures in adults almost universally receive intramedullary nailing due to superior biomechanics and early mobilisation. These protocols standardise care while allowing clinician judgment for borderline cases.
Manage fracture care workflows, track reduction outcomes, and coordinate multidisciplinary rehabilitation teams in one unified platform. Pabau supports orthopedic practices with clinical documentation, automated scheduling, and integrated billing for both operative and non-operative fracture management.

Recovery timelines and rehabilitation intensity differ substantially between closed and open reduction techniques. Closed methods generally allow earlier weight-bearing and joint motion because the soft tissue envelope remains intact. Open approaches require surgical wound healing and cautious progression to avoid hardware failure or wound complications.
Immobilisation duration depends on fracture location and stability. Upper extremity fractures typically require 4-6 weeks of casting followed by progressive range-of-motion exercises. Lower extremity fractures demand 6-12 weeks before full weight-bearing, with protected mobilisation starting earlier when fracture stability permits. Serial radiographs at 2, 6, and 12 weeks confirm maintained alignment and callus formation.
Physical therapy focuses on joint mobility adjacent to the fracture, muscle strengthening, and gradual return to function. Patients often resume light activities at 8-10 weeks and full unrestricted activity at 12-16 weeks. Complications like malunion or stiffness become apparent during this period. Practices using integrated physical therapy EMR systems track recovery milestones and flag delayed progressions for clinical review.
Surgical wounds require 10-14 days for primary healing before suture removal. During this period, the operated limb is protected but gentle range-of-motion exercises prevent stiffness. The stability of internal fixation often allows earlier mobilisation compared to closed reduction – rigid plate fixation may permit immediate weight-bearing for some lower extremity fractures.
Rehabilitation protocols vary by fixation method. Compression plating enables aggressive therapy beginning week two. Bridge plating over comminuted zones requires protected weight-bearing until bridging callus appears radiographically. Intramedullary nails allow early full weight-bearing because the implant shares load with healing bone. Physical therapists working within sports medicine clinics coordinate these protocols with surgical teams to optimise outcomes while preventing hardware complications.
Return to full activity typically requires 12-16 weeks for uncomplicated cases. High-level athletes or manual labourers may need 4-6 months before unrestricted participation. Hardware removal becomes necessary in 10-15% of cases due to irritation, with the second procedure adding recovery time and cost.
Accurate coding distinguishes closed from open reduction procedures and captures the complexity of fracture treatment. CPT codes differ not only by technique but also by anatomic location, fracture extent, and whether manipulation was performed. Understanding these distinctions prevents claim denials and ensures appropriate reimbursement.
Closed treatment codes follow a three-tiered structure: without manipulation, with manipulation, and with or without skeletal fixation (percutaneous pinning). Codes vary by anatomic site. For example, tibial shaft fractures use CPT 27750 (closed treatment without manipulation), 27752 (closed treatment with manipulation), or 27756 (percutaneous skeletal fixation). The manipulation modifier captures the work of achieving and maintaining reduction.
Fluoroscopy during closed reduction is separately reportable using CPT 77002. Anesthesia services are coded independently – procedural sedation (99152-99153) for moderate sedation or appropriate anesthesia CPT codes for general anesthesia. Cast application is included in the global fracture care code when performed by the treating surgeon, but separately billable when applied by a different provider.
Documentation must specify fracture type, manipulation performed, and imaging used. According to CMS physician fee schedule guidelines, inadequate documentation of manipulation may result in downcoding to the without-manipulation tier, reducing reimbursement by 30-40%.
Open reduction codes bundle surgical exposure, fracture reduction, internal fixation, and wound closure. The primary code reflects anatomic location and fracture complexity. Tibial shaft fractures use CPT 27792 for open treatment without internal fixation or 27766 for open treatment with internal fixation using plates, screws, or intramedullary devices. The code selection depends on fixation method employed.
Additional procedures performed during the same operative session may be separately billable with appropriate modifiers. Bone grafting (20900-20902), hardware removal from a previous surgery (20680), or treatment of associated soft tissue injuries can be coded in addition to the primary fracture care. However, services inherent to fracture treatment – such as routine debridement or wound closure – are included in the global surgical package.
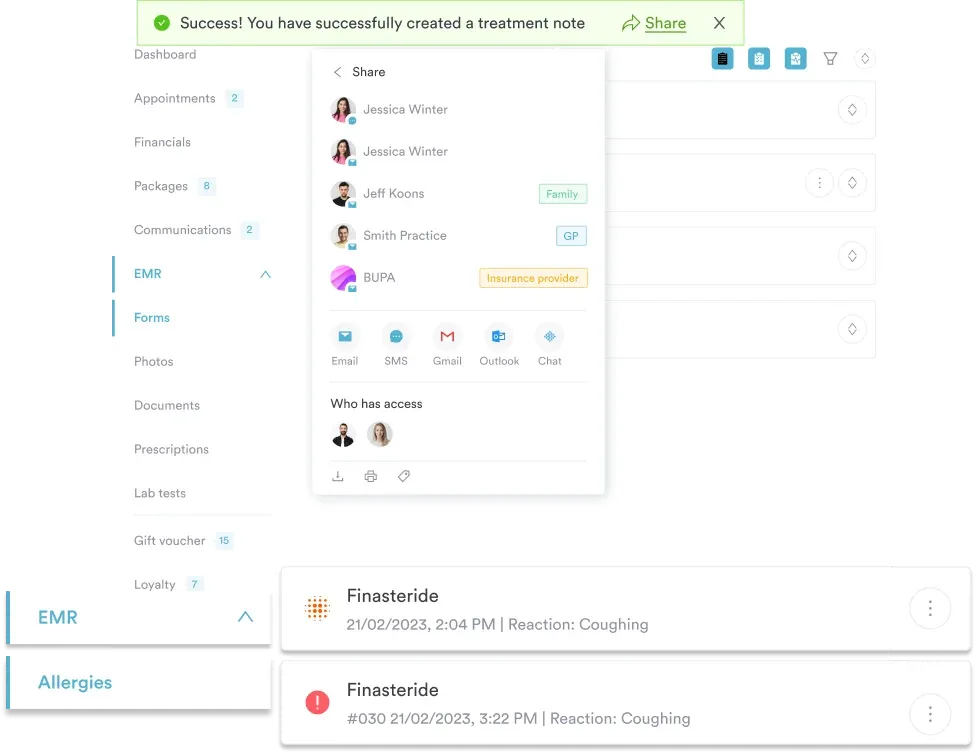
Practices managing complex orthopedic billing workflows benefit from integrated claims management systems that link CPT codes to procedure documentation. This reduces coding errors and accelerates claim submission.
Fracture diagnosis codes specify laterality, encounter type, and fracture characteristics. Initial encounter codes (seventh character “A”) apply to the acute treatment episode. Subsequent encounters use “D” for routine healing or “G”/”K” for delayed/nonunion complications. Closed fractures without open wounds use “A”, while open fractures require grade specification (Gustilo-Anderson classification).
For example, a closed tibial shaft fracture is coded S82.20XA (initial encounter). An open Grade II fracture of the same site uses S82.20XB. Accurate seventh-character assignment affects payer acceptance – claims with encounter mismatches trigger manual review and payment delays. Orthopedic practices using structured digital intake forms capture injury mechanism and fracture details at the point of care, improving coding accuracy.
Complication profiles differ substantially between techniques. Closed reduction avoids surgical site infection but accepts higher malunion rates. Open reduction achieves superior alignment but introduces deep infection risk, hardware complications, and neurovascular injury during exposure.
Radiographic monitoring detects loss of reduction early. Weekly films during the first three weeks identify displacement before significant healing consolidates malalignment. When detected, closed re-reduction or conversion to operative fixation prevents long-term functional deficits.
Risk mitigation strategies include meticulous surgical technique, perioperative antibiotics, and careful patient selection. Smoking cessation, diabetic control, and nutritional optimisation before elective surgery reduce infection and nonunion rates by 40-60%. Practices offering integrative medicine services can coordinate pre-surgical optimisation protocols that improve surgical outcomes.
Document reduction quality with standardised radiographic measurements at every follow-up visit. Angular deformity, translation, and rotational alignment should be quantified in degrees and millimeters. This creates defensible records if complications arise and supports quality improvement initiatives tracking reduction accuracy across your practice.
Managing post-fracture rehabilitation protocols? Return to Running Protocol for Physical Therapy provides evidence-based progressions for lower extremity fracture recovery.
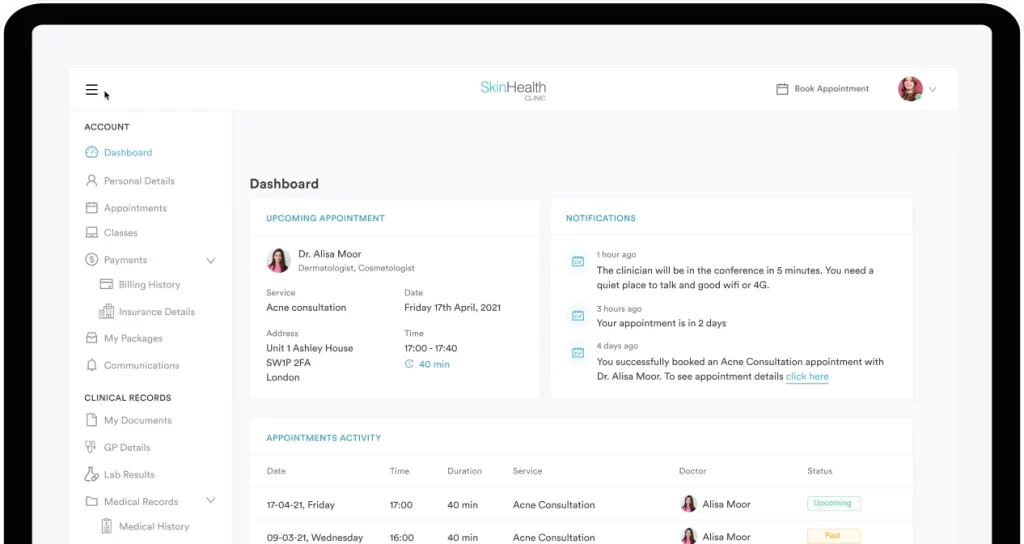
Tracking outcomes across reduction techniques? Clinic Dashboard Management aggregates complication rates, union times, and patient-reported outcomes to guide clinical decision-making.
Coordinating multidisciplinary fracture care? Chiropractic Software enables seamless communication between orthopedic surgeons, physical therapists, and manual therapy providers managing musculoskeletal injuries.
The decision between closed and open reduction balances anatomical precision against biological cost. Closed techniques preserve soft tissues and minimise infection risk, making them ideal for simple fractures with acceptable alignment parameters. Open reduction achieves superior fracture reduction and stable fixation, justifying the increased surgical risk for complex patterns requiring anatomical restoration.
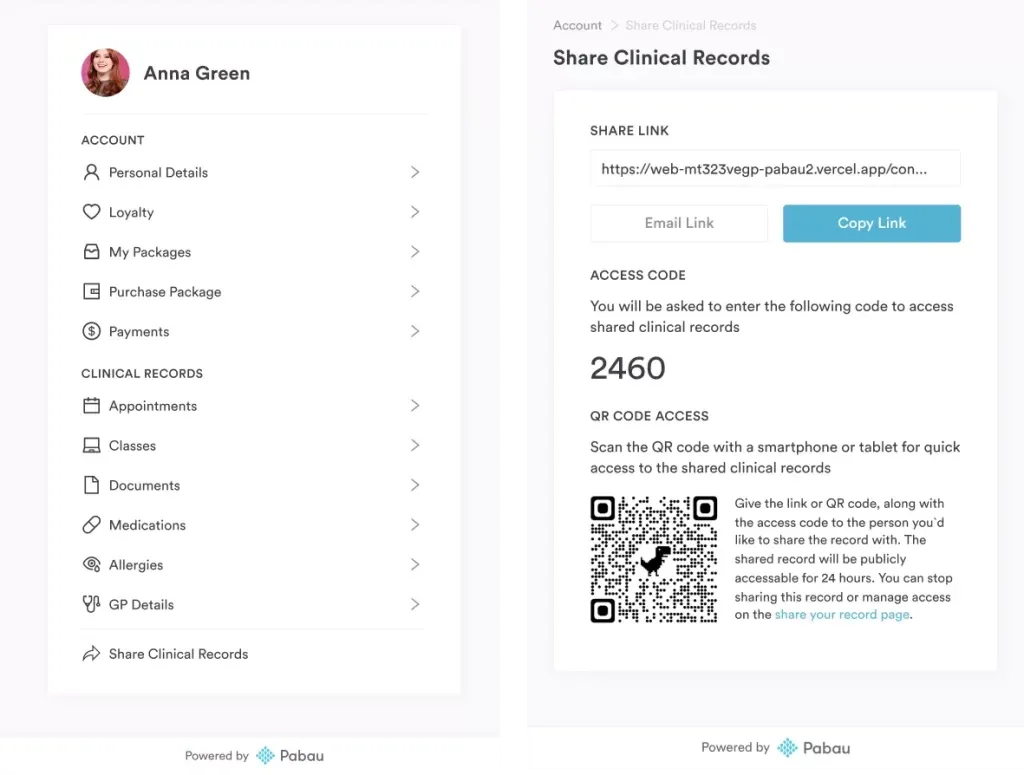
Clinical algorithms guide technique selection, but individual patient factors – comorbidities, functional demands, and treatment preferences – influence the final decision. Shared decision-making that educates patients about trade-offs improves satisfaction and compliance with rehabilitation protocols. Practices using patient portal systems provide educational resources and track patient-reported outcomes throughout the recovery period.
Orthopedic practices benefit from clinical pathways that standardise fracture management while allowing clinician judgment for borderline cases. Accurate documentation and coding ensure appropriate reimbursement for both closed manipulation and complex surgical fixation. As fracture care evolves with improved implants and minimally invasive techniques, the fundamental principles distinguishing closed from open reduction remain central to orthopedic practice.
Closed reduction manipulates fractures externally through intact skin using manual techniques and fluoroscopic guidance, while open reduction surgically exposes the fracture site to achieve direct visualisation and anatomical alignment with internal fixation devices. The primary difference lies in soft tissue disruption and visualisation quality.
Open reduction becomes necessary for intra-articular fractures with step-offs exceeding 2mm, displaced fractures that cannot be adequately aligned with closed techniques, open fractures requiring irrigation and debridement, and cases where closed reduction fails to achieve or maintain acceptable alignment. Complex fracture patterns with comminution or soft tissue interposition also typically require surgical intervention.
Closed reduction causes significant discomfort without adequate anesthesia. Most procedures use local hematoma blocks, procedural sedation, or general anesthesia to ensure patient comfort during manipulation. Post-reduction pain is typically managed with oral analgesics and resolves within 48-72 hours as soft tissues stabilise.
Closed reduction typically requires 6-12 weeks for bone healing with an additional 4-8 weeks for return to full activity. Open reduction recovery spans 8-16 weeks for bone union, with total rehabilitation extending to 12-24 weeks depending on fracture complexity and fixation method. Surgical wounds add 10-14 days for primary healing before aggressive therapy can begin.
ORIF carries risks including surgical site infection (2-8%), hardware failure requiring revision (3-8%), nonunion (5-10% for open fractures), iatrogenic neurovascular injury (under 2%), and hardware irritation necessitating removal (10-15%). These risks must be balanced against the superior alignment and earlier mobilisation that internal fixation provides for appropriate fracture patterns.