HCPCS
HCPCS Code J7327: Monovisc Billing and Reimbursement Guide
Viscosupplementation claims are among the most denial-prone drug injection codes...
April 6, 2026

Buy now, pay later is now available in Pabau
CPT 27570 requires general anesthesia per code descriptor
Documentation must prove failed conservative treatment before billing
Pre-authorization requirements vary significantly by payer
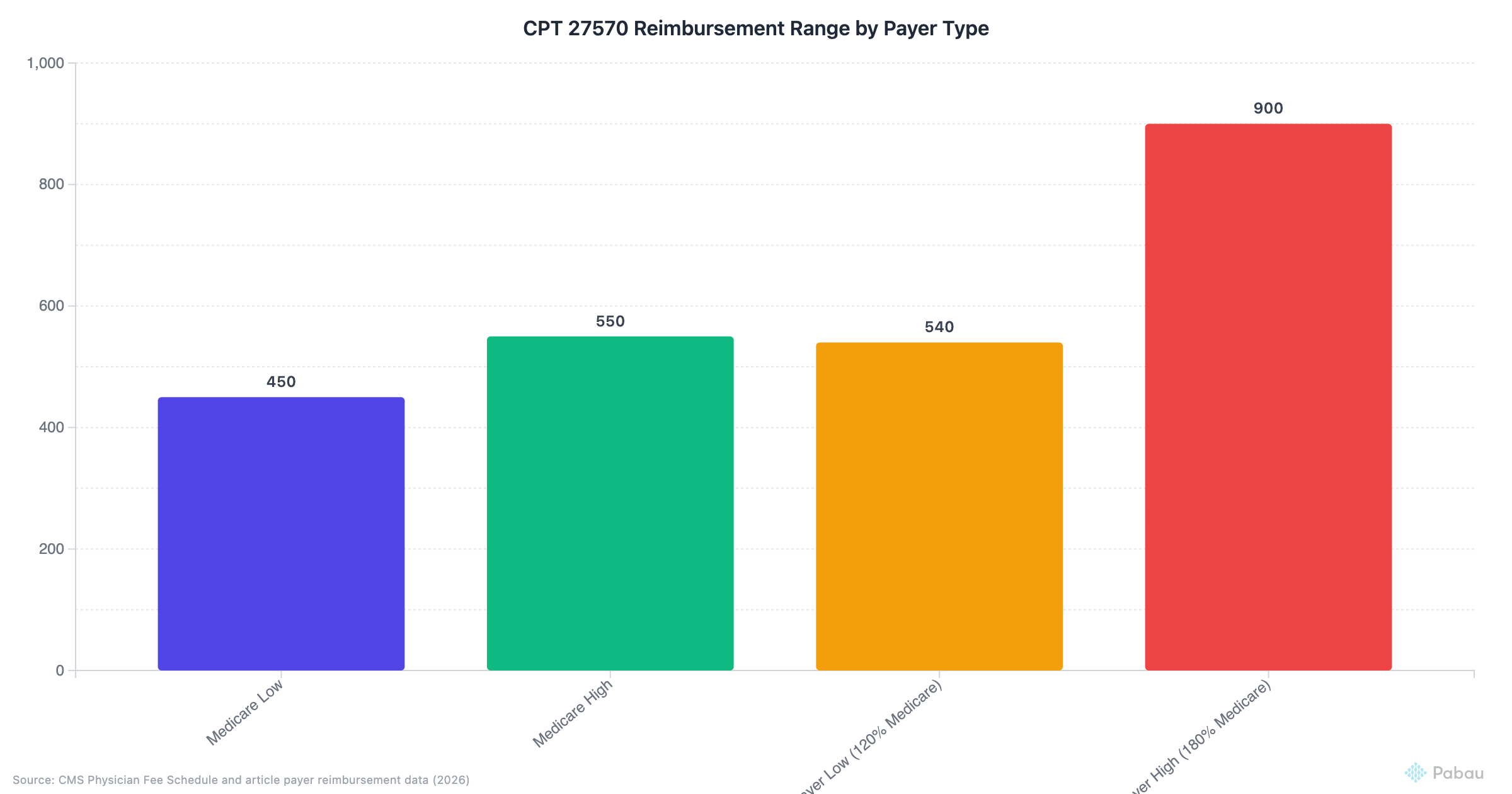
Reimbursement ranges $300–$800 depending on locality and contract
Common denials occur from anesthesia type mismatches and insufficient documentation
CPT code 27570 describes manipulation of the knee joint under general anesthesia. Orthopedic surgeons and sports medicine specialists use this procedure when a patient develops significant stiffness or restricted range of motion following knee surgery or injury. The manipulation aims to break up scar tissue (arthrofibrosis) that limits joint mobility, restoring functional movement through controlled force applied while the patient is unconscious.
According to the American Medical Association’s CPT code set, this code specifically requires general anesthesia—a critical billing detail many practices overlook. Using moderate sedation or regional blocks instead creates documentation conflicts that trigger claim denials. This guide covers when to use CPT 27570, documentation workflows that satisfy payer audits, modifier applications, reimbursement expectations, and denial prevention strategies orthopedic practices face regularly.
Understanding the specific requirements for CPT 27570 prevents revenue leakage from preventable denials. Claims management software designed for orthopedic workflows helps practices track authorization status, flag documentation gaps before submission, and monitor reimbursement patterns across different payers.
The full CPT 27570 descriptor states: “Manipulation of knee joint under general anesthesia (includes application of traction or other fixation devices).” This procedure addresses post-surgical or post-traumatic knee stiffness when conservative measures fail. Patients typically present with flexion contractures limiting their ability to bend the knee past 90 degrees or extension deficits preventing full straightening—functional losses that interfere with walking, stair climbing, and daily activities.
Surgeons consider manipulation after a minimum trial of physical therapy, home exercises, and anti-inflammatory management proves insufficient. Most payers require documentation showing at least 6–12 weeks of supervised therapy before approving manipulation. The procedure itself involves controlled force applied to the flexed and extended knee while the patient remains under general anesthesia, allowing the surgeon to break adhesions without patient guarding or pain response.
The anesthesia specification distinguishes CPT 27570 from less invasive manipulation techniques. General anesthesia ensures complete muscle relaxation, enabling the surgeon to apply sufficient force to disrupt scar tissue without risk of patient movement. If a practice performs the manipulation under regional block or monitored anesthesia care (MAC), different coding applies—creating a common source of claim rejections when the procedure note contradicts the billed code. Anesthesia records must explicitly document general anesthesia administration to support CPT 27570.
The code descriptor’s parenthetical note—”includes application of traction or other fixation devices”—clarifies that any traction apparatus, continuous passive motion (CPM) machine setup, or temporary splinting applied during the manipulation is bundled into the base code. Practices cannot bill separately for these components. Local infiltration anesthesia, if used in addition to general anesthesia, also falls within the global surgical package and should not be coded separately.
The Centers for Medicare & Medicaid Services (CMS) Physician Fee Schedule assigns CPT 27570 a work relative value unit (RVU) of approximately 5.50, translating to base reimbursement between $450 and $550 depending on geographic locality adjustments. Private payers typically reimburse 120–180% of Medicare rates, pushing the range to $540–$900 for contracted orthopedic groups. Reimbursement variance reflects regional cost differences, payer contract terms, and whether the manipulation occurs in an ambulatory surgery center (ASC) or hospital outpatient department (HOPD).
The 10-day global period means post-manipulation follow-up visits within that window are included in the procedure payment and should not be billed separately unless a distinct, unrelated service occurs. Most practices schedule a 7-day follow-up to assess range of motion gains and adjust physical therapy protocols—this visit uses no additional E/M code. If the patient develops an unrelated issue (e.g., urinary tract infection) during the global period, modifier 24 allows billing that service separately.
Payer audits for CPT 27570 focus on three core documentation elements: medical necessity justification, anesthesia type verification, and procedure detail. Missing any component triggers payment denials or downcoding to a lower-value manipulation code. Orthopedic practices using physical therapy EMR software that integrates therapy notes into the surgical record streamline this documentation chain, reducing claim rejection rates from incomplete files.
The operative note must reference prior conservative treatment and its failure. Acceptable documentation includes physical therapy visit summaries showing persistent range-of-motion deficits despite 6–12 weeks of supervised therapy, home exercise logs demonstrating patient compliance, and progress notes documenting pain or stiffness levels. Phrases like “patient completed 10 weeks of PT with minimal ROM improvement” or “flexion remains limited to 85 degrees despite 8 weeks of supervised therapy” establish medical necessity.
The anesthesia record must explicitly state “general anesthesia” or “GA” in the anesthesia type field. Phrases like “monitored anesthesia care” or “regional block with sedation” contradict the CPT 27570 descriptor and create automatic denial triggers. If an anesthesiologist bills a general anesthesia code (e.g., 01402) but the surgical note describes “light sedation,” payers flag the discrepancy. Both records must align.
The operative note should describe the manipulation technique in functional terms—flexion force applied, extension force applied, palpable adhesion release, post-manipulation range achieved. Example: “Under general anesthesia, knee manipulated with gradual flexion to 130 degrees (from preoperative 85 degrees), palpable scar tissue release noted, extension to 0 degrees achieved.” This level of detail satisfies audit requirements and supports billing integrity.
Audit manipulation notes quarterly for the phrase ‘general anesthesia’—missing this term is the most common documentation gap leading to CPT 27570 denials. Flag cases where anesthesia records show MAC or regional blocks for billing review before claim submission.
Modifier application determines whether a CPT 27570 claim processes at full payment, reduced payment, or denial. The most frequently used modifiers indicate laterality (left vs. right knee), bilateral procedures, and distinct procedural services performed during the same session. Misapplied modifiers trigger downcoding or bundling edits from the National Correct Coding Initiative (NCCI), reducing reimbursement below expected levels.
Modifier LT (left side) or RT (right side) specifies which knee received manipulation. Most payers require laterality modifiers on all orthopedic procedures to prevent duplicate payments. Omitting the modifier creates ambiguity—payers may deny the claim as “incomplete” or request medical records to determine laterality manually, delaying payment by 30–60 days.
Modifier 50 applies when both knees undergo manipulation during the same anesthesia session. Most payers reimburse bilateral procedures at 150% of the unilateral rate (not 200%), recognising shared anesthesia and facility costs. Some payers require two line items (27570-LT and 27570-RT with modifier 50 on the second line), while others accept a single line with modifier 50 and quantity 2. Check payer-specific billing guidelines before submitting bilateral claims to avoid processing errors.
Modifier 59 unbundles CPT 27570 from other procedures performed during the same session when the manipulation is distinct and separate. Example: If a surgeon performs arthroscopic meniscus repair (29881) and then manipulates the knee under the same anesthesia to address pre-existing stiffness unrelated to the arthroscopy, modifier 59 on CPT 27570 signals these are separate services. Without modifier 59, NCCI edits bundle the manipulation into the arthroscopy, denying separate payment. However, if the stiffness is a direct result of the arthroscopy just performed, modifier 59 is inappropriate—the manipulation becomes part of the surgical work and should not be billed separately.
CPT 27570 requires diagnosis codes that support the medical necessity of knee manipulation under general anesthesia. The diagnosis must reflect joint stiffness or restricted range of motion, typically as a sequela of prior surgery or trauma. Using generic joint pain codes (M25.56) without documenting stiffness creates a medical necessity denial—payers expect to see codes indicating functional limitation that warrants manipulation under anesthesia.
M25.661 (right knee) and M25.662 (left knee) are the primary diagnosis codes for knee stiffness not elsewhere classified. This code applies when the patient presents with reduced range of motion but no specific underlying cause is documented beyond post-surgical or post-traumatic scarring. Most payers accept M25.66x as a standalone justification for CPT 27570 when paired with documentation showing failed conservative treatment.
M24.661 (right knee) and M24.662 (left knee) describe complete or near-complete joint immobility—a more severe presentation than stiffness. Ankylosis codes support medical necessity for manipulation in cases where the knee has minimal or no functional range. Documentation must quantify preoperative range (e.g., “flexion 10–20 degrees, extension to 5 degrees”) to justify the diagnosis.
M67.461 (right knee) and M67.462 (left knee) apply when the manipulation addresses tendon or sheath contracture contributing to joint stiffness. This code works when physical exam findings identify specific tendon involvement rather than generalised intra-articular adhesions.
M96.89 covers postoperative complications of the musculoskeletal system, including arthrofibrosis following knee surgery. When manipulation addresses stiffness that developed specifically as a surgical complication, this code (paired with a more specific stiffness code like M25.66x) strengthens the medical necessity argument by linking the current condition to a prior procedure.
Listing multiple diagnosis codes that reflect the full clinical picture reduces denial risk. Example: M25.662 (left knee stiffness) as primary diagnosis, with Z98.89 (other specified postprocedural states) as secondary diagnosis, documents both the current symptom and its post-surgical context. Adding a historical code (e.g., S83.202A for prior meniscus tear, status post-repair) provides the backstory payers expect when reviewing manipulation claims.
Run a quarterly report comparing CPT 27570 claims to their paired ICD-10 codes—flag any claims using only joint pain codes (M25.56x) without stiffness codes (M25.66x). These are high-risk denials. Update diagnosis code sets in your EMR templates to auto-populate stiffness codes when CPT 27570 is selected.
Pre-authorization (PA) policies for CPT 27570 vary dramatically across payers, with some requiring PA for all manipulation procedures and others exempting it entirely. Medicare does not require prior authorization for CPT 27570 in most regions, but Medicare Advantage plans often impose stricter PA rules than traditional Medicare. Commercial payers frequently require PA to verify medical necessity before approving payment, particularly for procedures performed within six months of the initial knee surgery.
PA submissions must include physical therapy progress notes, range-of-motion measurements documented over multiple visits, and a narrative explaining why continued conservative treatment is unlikely to improve function. Payers typically require proof of at least 6–8 weeks of supervised therapy before approving manipulation. Missing PT records or insufficient therapy duration are the most common PA denial reasons. Practices using integrated claims management platforms that track PA status alongside scheduling prevent revenue delays from expired or pending authorizations.
Blue Cross, Aetna, and UnitedHealthcare publish payer-specific medical policies outlining PA criteria for joint manipulation procedures. These policies define acceptable conservative treatment timelines, range-of-motion thresholds that trigger manipulation consideration, and documentation requirements. Reviewing the relevant medical policy before submitting PA requests reduces back-and-forth appeals and speeds authorization turnaround. Some payers grant retroactive PA for emergency manipulations performed without prior approval, but relying on retroactive review introduces payment uncertainty—always submit PA when time allows.
CPT 27570 reimbursement reflects geographic practice cost differences, facility type, and payer mix. According to FastRVU’s 2026 data, the national average Medicare payment for CPT 27570 ranges from $450 to $550 before locality adjustments, with high-cost areas (e.g., New York, San Francisco) seeing adjustments up to 130% of the base rate. Private payers typically reimburse 120–180% of Medicare rates, pushing contracted rates to $540–$900 depending on negotiation strength and regional market dynamics.
Facility setting impacts reimbursement structure. When performed in an ambulatory surgery center (ASC), practices receive a professional fee for the manipulation itself while the ASC receives a separate facility fee. In a hospital outpatient department (HOPD), the hospital bills the facility component and the surgeon bills the professional component—total system reimbursement is higher in HOPD settings, but the surgeon’s take-home payment often remains similar. ASC settings reduce overhead for the practice but may introduce scheduling constraints if the ASC’s anesthesia team availability is limited.
Commercial payer reimbursement variation is significant. Some regional Blue Cross plans pay CPT 27570 at 150% of Medicare rates, while others cap payment at 110% regardless of contract terms. Bundled payment models (e.g., episode-based payments for knee replacement) may include manipulation as part of the surgical episode, eliminating separate reimbursement entirely. Practices participating in bundled payment arrangements should verify whether CPT 27570 is included in the bundle before billing separately—duplicate billing triggers recoupment demands.
CPT 27570 denials fall into three categories: anesthesia type mismatches, insufficient medical necessity documentation, and bundling conflicts with other procedures. Understanding denial patterns allows practices to implement front-end edits that prevent claim submission errors before they reach the payer. Orthopedic groups using practice management systems with built-in coding rules can flag high-risk claims during charge entry, reducing denial rates by 30–40%.
The most frequent denial reason is documentation showing an anesthesia type other than general anesthesia. If the anesthesia record lists “MAC” or “spinal block,” the payer denies CPT 27570 as medically unnecessary or requests downcoding to a code that does not specify anesthesia type. To prevent this denial, surgical schedulers should confirm anesthesia plans match CPT 27570 requirements before booking the case. Post-procedure, coders must cross-check anesthesia records against the operative note before finalising the claim.
Payers deny claims when medical records fail to show adequate conservative treatment before manipulation. Acceptable evidence includes dated physical therapy visit notes (minimum 6–8 weeks), home exercise logs, anti-inflammatory medication trials, and imaging reports showing no surgical correction is needed. A claim submitted without attached PT records generates an automatic medical necessity denial. Practices should append PT summaries or progress note excerpts directly to the claim at submission to bypass this denial trigger.
When CPT 27570 is billed alongside other knee procedures (e.g., arthroscopy codes), NCCI edits may bundle the manipulation into the primary procedure unless modifier 59 is appended correctly. Payers deny the manipulation as “included in the primary procedure” if documentation does not demonstrate the manipulation addressed a pre-existing condition separate from the primary procedure’s indication. To prevent bundling denials, operative notes must clearly state the manipulation was performed for stiffness unrelated to the day’s surgical intervention—phrases like “manipulation performed for chronic post-surgical stiffness predating today’s arthroscopy” establish the distinction.
Claims submitted without LT or RT modifiers are rejected as “incomplete” by most payers. This administrative denial is easily prevented by implementing coding rules that require laterality modifiers on all orthopedic procedure codes before claim release. Missing modifiers delay payment by 30–45 days while the claim cycles through rejection, correction, and resubmission.
When a CPT 27570 claim is denied, the appeals process requires submitting additional documentation that directly addresses the stated denial reason. Generic appeal letters (“Please reconsider this claim”) have low overturn rates—successful appeals include specific clinical details and cite payer policy language that supports the claim. Most payers allow 90–180 days from the initial denial date to file an appeal, with shorter windows for Medicare Advantage and Medicaid plans.
For anesthesia type denials, the appeal should include both the anesthesia record (highlighting “general anesthesia” documentation) and the operative report (confirming the manipulation was performed under GA). If the anesthesia record is ambiguous, a letter from the anesthesiologist clarifying the anesthesia level may resolve the dispute. For medical necessity denials, append complete physical therapy records showing treatment dates, range-of-motion measurements, and therapist notes confirming minimal progress despite compliance. Quantitative data (e.g., “flexion improved from 80° to 85° over 10 PT visits”) strengthens the appeal more than qualitative statements.
Bundling denials require operative note excerpts proving the manipulation was a distinct service. Highlight phrases that establish the manipulation addressed chronic stiffness separate from the primary procedure’s indication. If the payer’s medical policy lists specific criteria for unbundling (e.g., “manipulation may be billed separately when performed for stiffness predating the primary procedure by at least 30 days”), cite those criteria directly in the appeal letter and attach documentation meeting each criterion.
Second-level appeals (filed after a first appeal denial) typically require peer-to-peer review—a phone conversation between the treating surgeon and the payer’s medical director. During peer-to-peer discussions, surgeons should reference the payer’s published medical policy, cite clinical guidelines supporting manipulation timing, and describe the patient’s functional limitations in concrete terms (“unable to climb stairs, cannot sit in standard chair due to flexion limitation”). Documenting the peer-to-peer conversation outcome in the patient’s chart creates an audit trail if the claim proceeds to external review or litigation.
Track CPT 27570 denial reasons in your claims management dashboard to identify patterns—if 80% of denials cite anesthesia type conflicts, implement a scheduling protocol requiring anesthesia plan confirmation before case booking.
Build a CPT 27570 appeal template that includes placeholders for PT records, anesthesia documentation, and operative note excerpts—this reduces appeal preparation time from 45 minutes to 10 minutes per claim.
For orthopedic practices handling complex post-surgical cases, integrated EMR systems that pull therapy notes directly into the surgical record streamline documentation workflows and reduce missing-record denials.
Billing CPT code 27570 successfully depends on three documentation pillars: proving conservative treatment failure, verifying general anesthesia use, and quantifying pre- and post-manipulation range of motion. Orthopedic practices that implement pre-submission checklists for these elements reduce claim denials by 40–50%, accelerating cash flow and minimising administrative burden. Pre-authorization tracking, modifier accuracy, and bundling rule awareness prevent the most common payment delays.
Understanding payer-specific policies—particularly regarding PT duration requirements and anesthesia type verification—allows practices to tailor documentation before submitting claims, rather than scrambling to respond to denial requests weeks later. Practices using clinic management software designed for orthopedic workflows benefit from automated coding checks, PA status tracking, and denial pattern reporting that surface billing issues before they impact revenue cycles. CPT 27570 reimbursement is predictable when documentation aligns with payer expectations, making front-end process discipline the highest-leverage intervention orthopedic billing teams can implement.
No. CPT 27570 specifically requires general anesthesia per its code descriptor. If spinal anesthesia or regional block was used, a different code must be selected. Billing 27570 with non-general anesthesia documentation triggers automatic denial.
Most payers require documentation of 6–12 weeks of supervised physical therapy showing minimal improvement before approving manipulation under anesthesia. Check your payer’s medical policy for specific duration requirements, as some plans mandate longer trials.
Use modifier 50 to indicate a bilateral procedure. Reimbursement is typically 150% of the unilateral rate, not 200%, because anesthesia and facility costs are shared. Some payers require two line items (27570-LT and 27570-RT) with modifier 50 on the second line.
Only if the manipulation addresses pre-existing stiffness unrelated to the arthroscopy. Append modifier 59 to CPT 27570 and document that the stiffness predated the arthroscopy. If the manipulation is performed to address acute surgical changes from the arthroscopy itself, it is considered part of the primary procedure and should not be billed separately.
CPT 27570 has a 10-day global period. Post-manipulation follow-up visits within 10 days are included in the procedure payment and should not be billed separately unless unrelated services are provided (use modifier 24 for unrelated E/M visits during the global period).
Reduce CPT 27570 denials and speed reimbursement with automated coding checks, pre-authorization tracking, and integrated documentation. See how Pabau helps orthopedic practices improve cash flow.