Mental Health Mental Health & Therapy
CRAFFT Screening Tool Template
The CRAFFT Screening Tool Template is a clinically validated instrument designed...
March 17, 2026

Buy now, pay later is now available in Pabau
SOAP notes are a core part of social work documentation, providing a clear and structured way to record clinical encounters.
When written effectively, they support continuity of care, guide treatment decisions, and improve communication across care teams.
SOAP notes are a structured method for documenting client sessions in social work and mental health.
The acronym stands for Subjective, Objective, Assessment, and Plan.
This framework ensures that every session note captures not just what a client says, but also what the clinician observes, assesses, and plans to do next.
For social workers, SOAP notes bridge empathy with accountability. They provide a clear, standardized format for recording interventions and outcomes, helping ensure consistent and legally defensible documentation.
In mental health settings, SOAP notes are more than administrative requirements—they are clinical tools.
Accurate SOAP documentation improves client outcomes, facilitates continuity of care, and supports multidisciplinary collaboration.
For example, if a client’s therapist, case manager, and psychiatrist all access the same record, SOAP notes allow them to see progress in a unified language.
| Benefit | Impact on Social Work Practice |
|---|---|
| Structured communication | Improves clarity between professionals |
| Accountability | Supports legal and ethical standards |
| Efficiency | Reduces time spent documenting cases |
| Continuity of care | Ensures seamless information sharing |
This part records the client’s subjective experience—their emotions, self-reported issues, and insights.
Social workers should capture the client’s words as accurately as possible, often using direct quotes.
This part covers observable facts—things you can measure or verify, such as physical presentation, attendance, or mood indicators. Here, you should stick to objective data and avoid any kind of interpretation.
The Assessment part integrates subjective and objective data.
Here, the social worker identifies patterns, progress, or risk factors and offers professional insight.
The Plan outlines the next steps, including follow-ups, interventions, or referrals. It keeps the treatment goal-oriented and trackable.
Here are some examples of better alternatives to common mistakes:
| Common Error | Better Alternative |
|---|---|
| “Client doing better.” | “Client demonstrated improved coping by identifying three triggers for anxiety.” |
| “Session went well.” | “Client was engaged throughout session; reported decreased panic frequency from five to three times per week.” |
| “Will continue.” | “Plan to continue weekly CBT with focus on relapse prevention.” |
The structured SOAP format isn’t just clerical—it originated in medicine to make complex patient cases easier to understand and communicate across clinicians, and now it’s widely adopted in social work to standardise progress tracking.
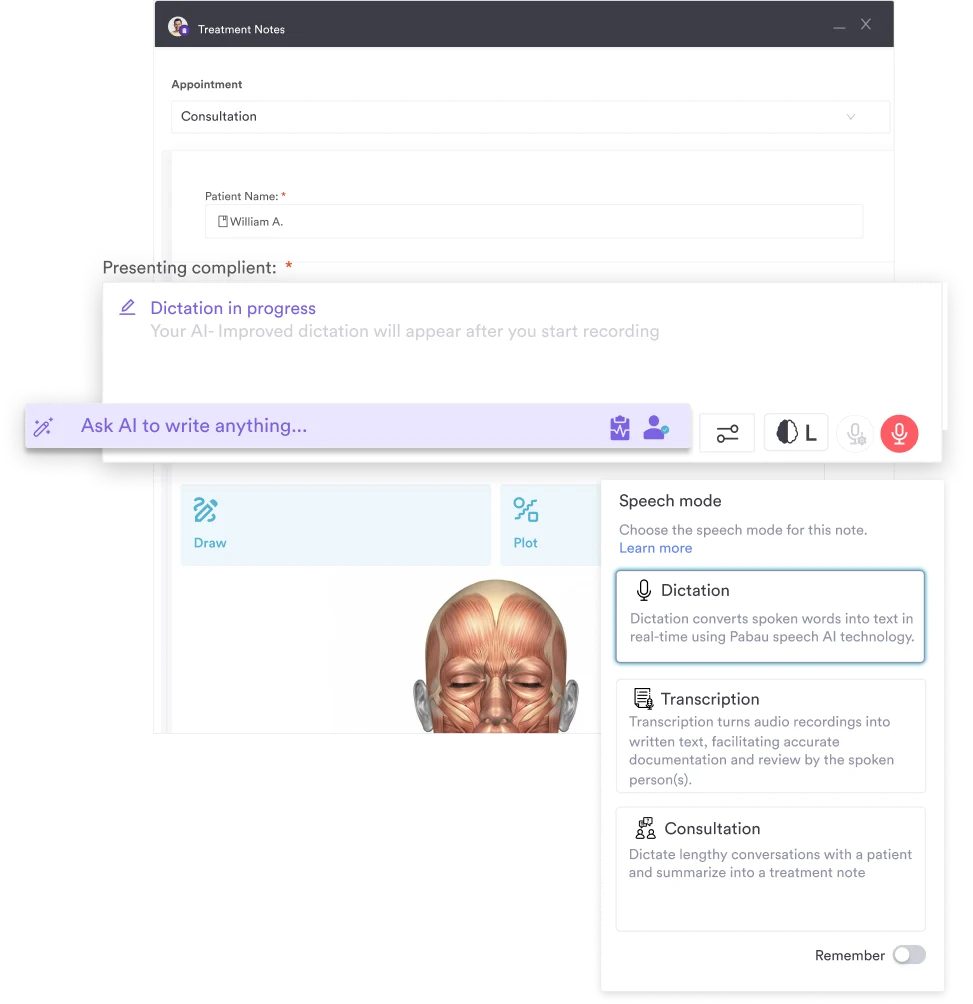
To support these practices, Pabau’s AI scribe tool can automatically capture key details during client appointments and generate structured notes, helping clinicians ensure nothing important is missed while reducing documentation time.
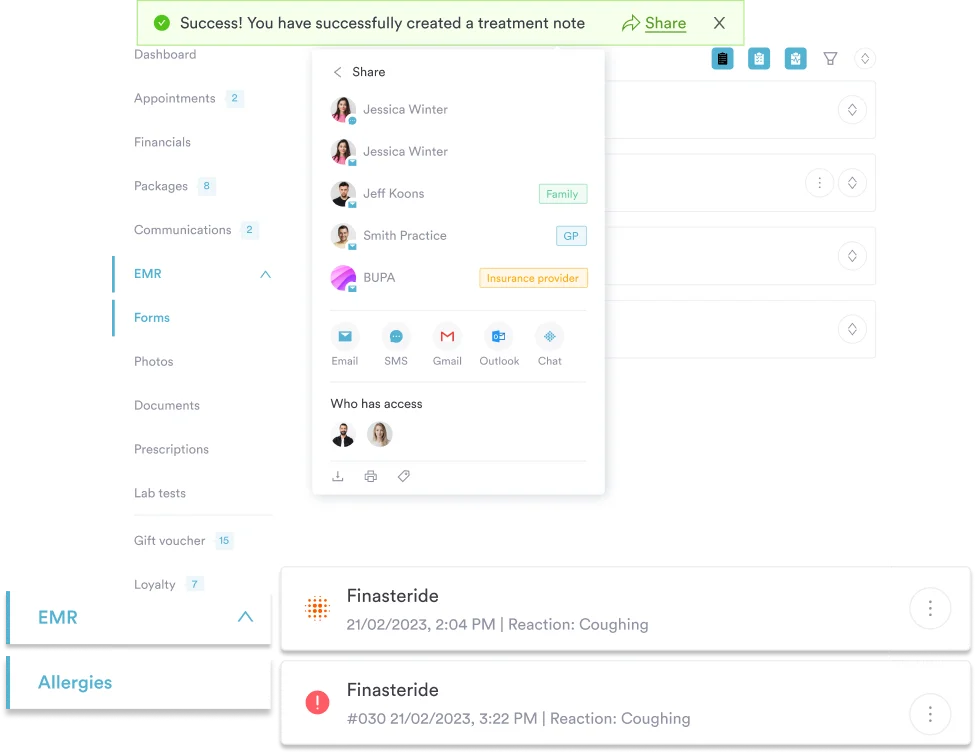
Modern practice management software simplifies documentation through digital templates and secure storage. These tools reduce administrative burden and improve data accessibility across teams.
With platforms like Pabau, social workers can manage digital client records, automate reminders, and standardize note formats—all while maintaining confidentiality and compliance.
SOAP notes remain one of the most efficient, professional, and defensible methods for documenting social work sessions. By adhering to a structured process—focusing on subjective insights, objective data, assessment synthesis, and actionable plans—social workers ensure their documentation is accurate, ethical, and client-centered.
So, if your mental health clinic manages therapy sessions, social care services, or interdisciplinary teams, Pabau can help you maintain clarity and consistency across all clinical documentation.
It offers a comprehensive, medical-grade documentation and records suite for 2026, functioning as a unified platform—so clinicians don’t need multiple systems for progress notes, follow-ups, and reports.
Request a live demo with Pabau today.