Protocol vs Procedure: Key Differences in Healthcare
Protocol vs Procedure: Understanding the Difference in Healthcare Settings A pro...
March 11, 2026
Discover free eBooks, guides and med spa templates on our new resources page

Buy now, pay later is now available in Pabau
Read case studies from our satisfied clients
Compare Pabau with alternative systems

Learn why this holistic care and aesthetic medicine clinic chose Pabau to power patient care and performance.
Read moreProtocols define clinical decision-making frameworks; procedures specify task execution steps
Protocols guide when and why to act; procedures detail how to perform specific actions
Healthcare facilities use protocols for treatment pathways and procedures for technical tasks
Regulatory bodies like CQC and Joint Commission require documented protocols and procedures
Effective clinics maintain both protocol libraries and procedure manuals for operational clarity
A protocol vs procedure distinction shapes how clinical teams make decisions and execute tasks. Protocols establish the clinical reasoning framework – when to act, which pathway to follow, what criteria trigger specific interventions. Procedures document the mechanical steps – how to insert an IV line, how to sterilise instruments, how to document a consultation. Both are essential. Neither is interchangeable.
Industry surveys suggest that mid-sized UK private practices typically maintain dozens of documented protocols and well over a hundred standard procedures across clinical, administrative, and safety domains. US multi-specialty clinics report similar ratios: roughly three procedures for every protocol. The distinction matters because regulatory audits assess whether your clinic applies the right tool to the right situation. A protocol answers “should we?”. A procedure answers “how do we?”.
This guide clarifies when each document type applies, how to structure them for compliance management, and why confusing the two creates operational friction. You’ll learn the functional differences, see real clinic examples, and understand how practice management systems organise both.
A protocol is a clinical decision-making framework. It defines the conditions under which specific actions should occur, the clinical criteria that must be met, and the treatment pathways available based on patient presentation. According to the National Institute for Health and Care Excellence (NICE), protocols serve as evidence-based guides that standardise clinical judgement without removing clinician autonomy.
Protocols address questions like: When should a physiotherapist escalate a patient to secondary care? What blood pressure threshold triggers immediate GP review? Which contraindications prevent Botox administration? They contain conditional logic – if X, then Y – and often reference multiple procedures within a single pathway.
A dermatology clinic’s acne treatment protocol might specify: patients with moderate-to-severe cystic acne and no contraindications receive oral isotretinoin, patients with mild comedonal acne receive topical retinoids, patients with suspected rosacea receive azithromycin pending biopsy. Each decision branch then links to the relevant administration procedure. The protocol guides the “what” and “when”. The procedures handle the “how”.
Regulatory bodies define protocols as living documents. The Care Quality Commission (CQC) expects UK clinics to review clinical protocols annually and update them when new evidence emerges. The Joint Commission in the US mandates that protocols align with current clinical guidelines and reflect the scope of practice for each professional category. A protocol that contradicts NICE guidance or FDA labelling creates liability exposure.
Effective protocols include: clinical indications, exclusion criteria, decision trees with clear branch points, references to supporting evidence, and version control metadata. They do not include step-by-step task instructions – that’s the procedure’s role. A mental health clinic might have a crisis intervention protocol that specifies when to activate emergency services, but the procedure for documenting the crisis contact sits separately.
A procedure is a step-by-step instruction set for completing a specific task. It eliminates ambiguity by documenting the exact sequence, required materials, safety checks, and completion criteria. Procedures assume the decision to act has already been made – they focus solely on execution.
Procedures answer: How do you calibrate a laser device? How do you collect a blood sample? How do you document a consent form in the EHR? They are linear, prescriptive, and often include photos or diagrams. A single clinical protocol might reference five separate procedures depending on the treatment pathway selected.
Consider a medical spa’s dermal filler administration. The procedure specifies: clean injection site with alcohol swab, allow 30 seconds drying time, draw product into 1ml syringe using 18-gauge needle, switch to 27-gauge needle for injection, inject slowly at 45-degree angle, massage area gently for 10 seconds, apply ice pack for 2 minutes, document batch number and injection sites in patient record. Each step follows a fixed order. Deviation requires documented justification.
Procedures serve three functions: training standardisation, quality assurance, and liability protection. A new team member follows the procedure to learn the task. An auditor compares actual practice to the documented procedure. A legal review confirms that the clinic followed its own stated process. Team management systems often embed procedures into onboarding checklists and competency assessments.
Unlike protocols, procedures rarely require clinical judgment. They assume a qualified professional is performing the task and focus on operational consistency. A sterilisation procedure for surgical instruments applies identically whether the clinic is treating acne or performing hair transplants. The protocol determines which instruments are needed; the procedure ensures they are prepared correctly.
The protocol vs procedure distinction operates across five dimensions: purpose, structure, flexibility, authorship, and review cycles. Understanding these differences prevents documentation confusion and improves operational clarity.
Protocols guide clinical reasoning. They help practitioners decide which intervention to apply based on patient presentation, test results, and risk factors. Procedures eliminate task variability. They ensure a specific action is performed the same way every time, regardless of who executes it.
A chronic pain clinic’s opioid prescribing protocol assesses addiction risk, reviews state prescription monitoring databases, and determines appropriate dosing limits. The procedure for entering the prescription into the prescription management system documents the software steps, required fields, and verification checks. The protocol requires clinical judgment; the procedure requires operational consistency.
Protocols contain conditional logic and decision trees. They branch based on patient variables – age, comorbidities, contraindications, treatment history. A fertility clinic’s IVF protocol might have separate pathways for patients under 35, patients 35-40, and patients over 40, with different stimulation protocols and transfer strategies for each group.
Procedures follow linear sequences. Step 1 leads to Step 2, which leads to Step 3. Branching is rare and usually limited to error handling – “if equipment fails, switch to backup device”. A blood draw procedure lists materials, skin preparation, needle insertion technique, tube labelling, and disposal steps in fixed order. No patient-specific customisation occurs.
Protocols allow clinical judgment within defined boundaries. A prescribing protocol might specify dose ranges, monitoring intervals, and discontinuation criteria, but the clinician selects the exact dose based on patient response. The protocol sets guardrails; the practitioner navigates within them.
Procedures demand strict adherence. Deviating from a sterilisation procedure or skipping steps in a consent documentation procedure creates compliance risk. CQC inspections specifically check whether staff follow documented procedures during observed tasks. A procedure that is never followed signals either poor training or an unrealistic process.
Protocols require clinical expertise and regulatory alignment. A medical director or lead clinician typically authors clinical protocols, with input from specialty practitioners. Approval often involves a clinical governance committee and periodic review against updated guidelines from NICE, the American Academy of Dermatology, or other authoritative bodies.
Procedures can be written by operational staff with task-specific knowledge. An office manager might document the appointment booking procedure. A senior nurse might write the vaccine administration procedure. Clinical oversight ensures safety, but the authorship threshold is lower. Procedures focus on operational consistency, not clinical reasoning.
Protocols require annual reviews at minimum, with interim updates when new evidence emerges. A longevity clinic’s hormone replacement therapy protocol must reflect FDA safety communications, NICE technology appraisals, and emerging research on cardiovascular risk. The review cycle matches the pace of clinical evidence.
Procedures update less frequently unless equipment changes or regulatory requirements shift. A consent form completion procedure might remain stable for years. When digital forms replace paper, the procedure updates to reflect the new workflow, but the content remains operationally similar.
Clinical decision-making requires protocols. Task execution requires procedures. The boundary is clear when you ask: “Does this document help someone decide what to do, or does it help them do it correctly?”
Use a protocol when the situation demands clinical judgment, risk assessment, or pathway selection. Examples include: anticoagulation management, pain escalation pathways, adverse reaction responses, treatment modification criteria, referral triggers. Each scenario involves evaluating patient-specific variables and selecting the appropriate intervention.
Use a procedure when the task follows a repeatable sequence with minimal variation. Examples include: equipment calibration, sterile field preparation, medical record documentation, appointment confirmation calls, insurance verification steps. These tasks require operational precision, not clinical reasoning.
A physical therapy clinic demonstrates the distinction clearly. The return-to-sport protocol for ACL reconstruction patients outlines assessment criteria at weeks 6, 12, 16, and 20, with progression requirements for strength, range of motion, and functional testing. The protocol determines whether a patient advances. The procedure for performing a single-leg hop test documents the exact testing setup, measurement technique, and scoring method. The protocol decides when to test; the procedure ensures the test is performed consistently.
Hybrid documents sometimes emerge – standard operating procedures (SOPs) that blend both elements. A medical spa’s patient intake SOP might include protocol elements (contraindication screening, consent requirements) and procedure elements (how to enter data into the client record system). Clear section headings prevent confusion: “Clinical Assessment Protocol” and “Data Entry Procedure” separate the decision-making from the task execution.
Three clinic scenarios illustrate how protocols and procedures interact in daily operations.
The suspicious lesion protocol guides the clinician through risk assessment using the ABCDE criteria, dermoscopy findings, and patient history. It specifies: lesions with 3+ high-risk features require biopsy within 2 weeks, lesions with 1-2 features require photography and 3-month review, benign-appearing lesions receive patient education and annual skin checks.
Once the protocol determines biopsy is needed, three procedures activate: the biopsy consent procedure (verbal explanation script, written form completion, documentation fields), the shave biopsy procedure (local anaesthesia technique, blade selection, specimen handling), and the pathology submission procedure (form completion, courier scheduling, result tracking). The protocol made the clinical decision; the procedures ensure consistent execution.
The crisis intervention protocol assesses suicide risk using validated screening tools, determines whether the patient can remain in outpatient care or requires psychiatric admission, and specifies follow-up intervals. It addresses clinical questions: Is the patient safe? What level of care is appropriate? Who needs to be notified?
The safety planning procedure documents how to complete the crisis plan template, which client portal fields to populate, how to assign check-in reminders, and when to schedule the next appointment. The procedure handles administrative execution after the protocol establishes the clinical plan.
The dehydration treatment protocol stratifies patients by severity (mild, moderate, severe), determines appropriate fluid type and volume based on weight and symptoms, and identifies contraindications (heart failure, renal impairment). A patient with moderate dehydration, normal cardiac function, and no contraindications receives 1000ml normal saline over 60 minutes.
The IV insertion procedure documents: skin preparation steps, catheter size selection, insertion angle, securement technique, and line patency checks. The infusion monitoring procedure specifies: vital sign intervals, site inspection frequency, completion documentation. The protocol selected the treatment; the procedures ensure safe delivery.
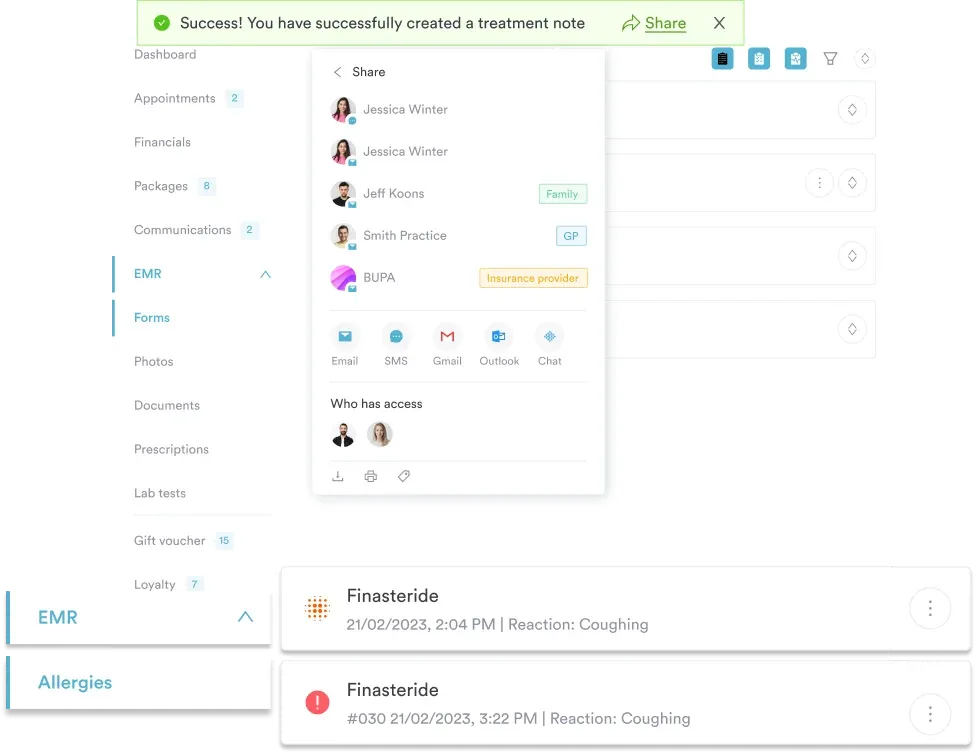
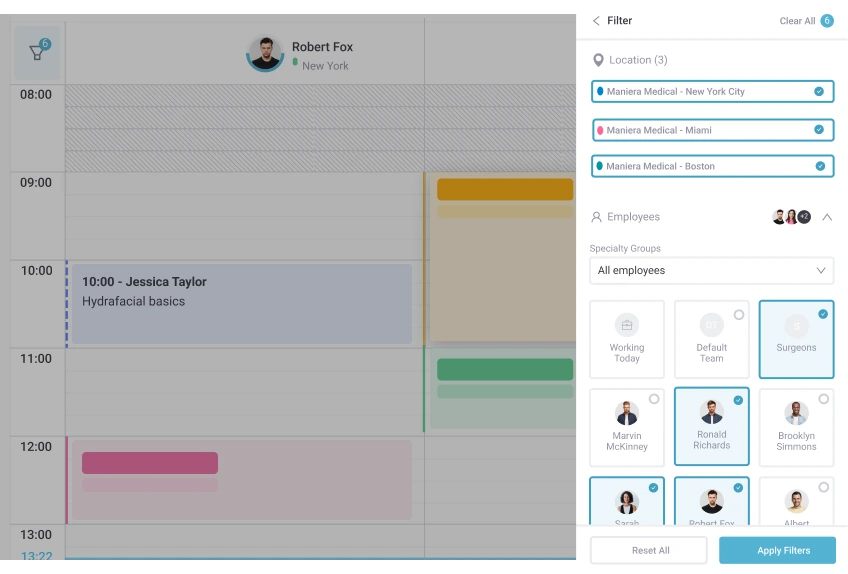
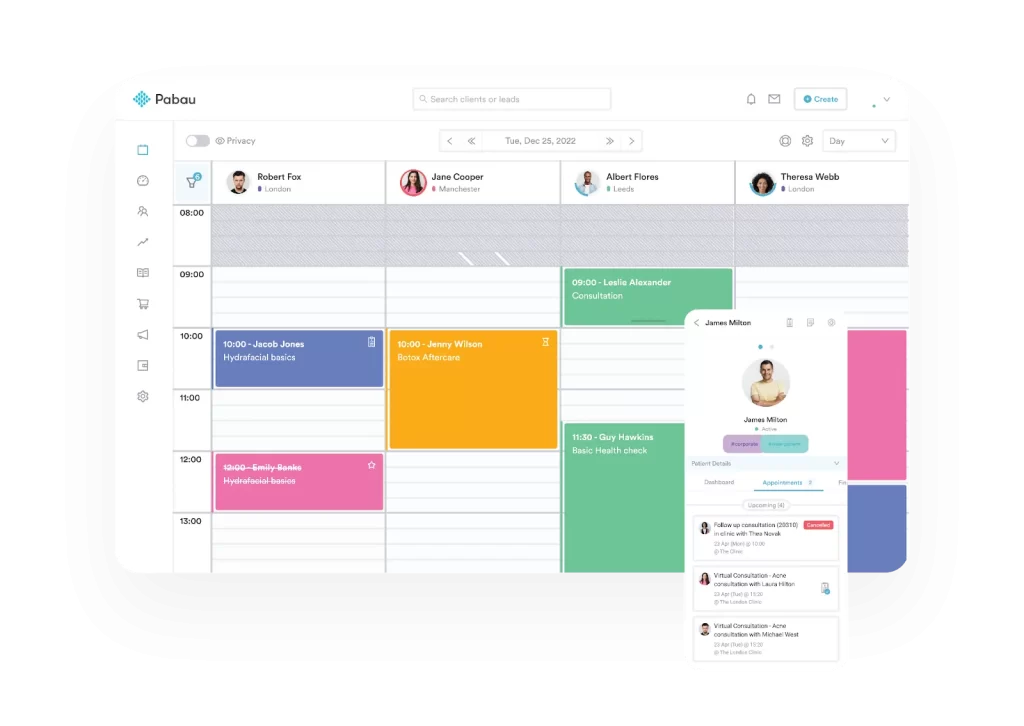
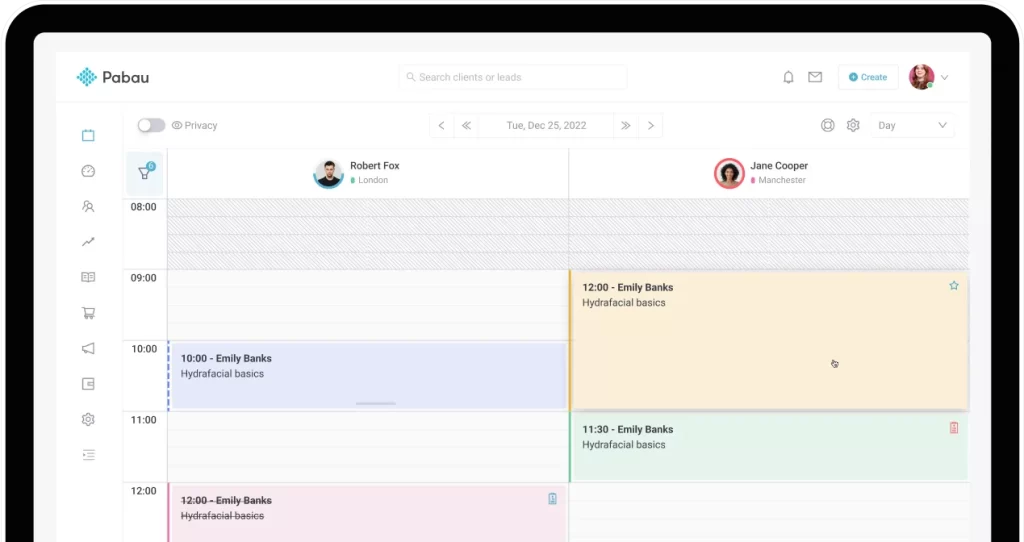
See how Pabau helps healthcare practices manage protocol libraries, procedure checklists, and compliance documentation in a centralised platform that supports consistent clinical workflows across multiple locations.

Regulatory compliance depends on documented evidence that protocols and procedures exist, are current, and are followed. The CQC’s fundamental standards require “persons employed by the service receive appropriate support, training, professional development, supervision and appraisal as is necessary to enable them to carry out the duties”. That support includes access to current protocols and procedures.
Both document types require version control. Each protocol and procedure needs: a unique identifier, version number, effective date, review date, author name, approver name, and change history. Industry analyses suggest that a significant proportion of UK private clinics fail compliance audits due to outdated protocols still in active use, despite newer versions existing. Version control prevents this.
Protocols must reference their evidence base. A prescribing protocol cites relevant NICE guidelines, British National Formulary entries, or specialty society recommendations. Procedures document the rationale for each step when the reason is not immediately obvious. “Allow alcohol to dry for 30 seconds” followed by “(prevents injection site burning and ensures antiseptic effectiveness)” turns a task step into an educational tool.
Training records link staff competencies to specific protocols and procedures. A new nurse practitioner signs off on the anticoagulation protocol after supervised application with three patients. A receptionist completes the appointment booking procedure during onboarding and demonstrates proficiency before handling real bookings. GP clinic software often tracks which team members have been trained on which documents and flags required refresher training.
Accessibility matters as much as existence. Protocols and procedures stored in a filing cabinet do not support real-time decision-making. Cloud-based practice management systems make documents searchable, mobile-accessible, and linked to relevant workflows. When a clinician opens a patient chart, the applicable protocols appear contextually. When staff begin a task, the procedure is one click away.
Five errors undermine the effectiveness of clinical documentation.
A document titled “Patient Intake Procedure” that includes sections on consent assessment, contraindication screening, and treatment selection is actually a protocol with embedded procedures. Separate them. The “New Patient Assessment Protocol” guides clinical decisions. The “Patient Check-In Procedure” documents administrative steps. Mixing them creates confusion about whether the document requires clinical judgment or operational consistency.
Protocols that specify every possible scenario become unreadable. A 47-page wound care protocol that addresses every wound type, location, and comorbidity is too complex for real-world use. Effective protocols cover the 80% of cases that follow predictable patterns and include an escalation pathway: “For complex presentations, consult wound care specialist.”
A procedure that says “Clean the treatment area” without specifying cleaning agent, contact time, or acceptable surfaces leaves too much open to interpretation. Procedures assume the reader has basic competence but needs exact specifications. “Apply Clinell Universal Wipes to all non-porous surfaces, allow 30-second contact time, wipe dry with disposable paper towel” eliminates ambiguity.
Protocols written by medical directors who do not perform front-line care often miss practical constraints. Procedures written by administrators who do not execute the tasks include steps that are impossible in real workflows. Effective documentation includes input from the people who will use it. A reception procedure written without receptionist input is likely to fail.
A protocol that references a medication withdrawn from the market creates liability. A procedure that describes software screens from three versions ago wastes staff time. Documentation must be living. Quarterly reviews for high-use documents, annual reviews for everything else, and immediate updates when external changes (new regulations, equipment changes, safety alerts) occur.
Embed protocol and procedure links directly into your practice management system workflows. When a clinician selects a treatment in the EHR, surface the relevant protocol as a pop-up reference. When a staff member begins a task, display the procedure steps as a checklist. Contextual access reduces the gap between documentation and practice.
Modern practice management systems organise clinical and operational documentation in ways that support real-time decision-making and compliance tracking. Three capabilities distinguish effective systems.
Protocols and procedures appear when and where they are needed. A clinician reviewing a patient with chronic pain sees the opioid prescribing protocol linked from the medication screen. A front desk staff member checking in a new patient sees the intake procedure embedded in the appointment workflow. The system matches documents to tasks.
Every protocol and procedure update creates a version history. Staff always access the current version. Administrators see who approved changes and when. Auditors verify that outdated documents are archived, not deleted. A CQC inspector can confirm that the catheterisation procedure in use during a January incident matched the version approved in December.
Staff competency tracking links to specific documents. A new hire’s onboarding checklist includes: read the medical emergency protocol, complete the consent procedure training module, demonstrate the blood pressure measurement procedure under supervision. Automated workflows assign refresher training when protocols update or annual competency renewals are due.
The integration reduces administrative overhead while improving compliance. Rather than maintaining separate policy manuals, training logs, and competency records, the practice management system unifies them. A single source of truth for what should happen and evidence that it did.
Building consistent clinical workflows? Compliance Management Software helps practices organise protocols, track procedure adherence, and maintain audit-ready documentation across all service lines.
Need staff training tracking? Team Management Software links protocol training to competency assessments and flags required refresher courses when documents update.
Looking for standardised patient documentation? Digital Forms embeds consent procedures and assessment protocols directly into the patient intake workflow.
Different healthcare sectors emphasise protocols and procedures differently based on clinical complexity and regulatory requirements.
Medical aesthetics practices rely heavily on treatment protocols. Botox protocols address contraindications, dosing guidelines, and injection site selection. Laser protocols specify skin type classifications, fluence settings, and cooling parameters. Each protocol links to multiple procedures: consent documentation, device calibration, treatment execution, post-care instructions. A single aesthetic consultation might reference five protocols and twelve procedures.
Primary care practices balance protocol-driven care with individualised treatment plans. Chronic disease management protocols for diabetes, hypertension, and COPD guide initial assessment, medication selection, and monitoring intervals. Wellness clinics implementing preventive care programmes use protocols to stratify patients by risk level and procedures to standardise screening workflows.
Allied health practices focus on assessment protocols and treatment progression procedures. A physical therapy clinic’s return-to-work protocol evaluates functional capacity, determines restrictions, and sets rehabilitation goals. The therapeutic exercise procedure documents setup, dosage, progression criteria, and documentation requirements. Sports medicine practices layer injury-specific protocols over standardised testing procedures.
Mental health services distinguish between clinical protocols (suicide risk assessment, crisis intervention, medication management) and administrative procedures (appointment scheduling, insurance verification, treatment plan documentation). The boundary is particularly important when non-clinical staff handle tasks that intersect with patient care. A scheduling procedure might include a section on recognising and escalating urgent requests – operational guidance without clinical decision-making.
The protocol vs procedure distinction is not semantic. It reflects fundamental differences in how healthcare teams make decisions and execute tasks. Protocols provide clinical frameworks that guide when and why to act. Procedures ensure tasks are performed consistently, safely, and in compliance with standards.
Effective healthcare practices maintain both. They document protocols for clinical decision points – treatment selection, risk assessment, pathway escalation. They document procedures for repeatable tasks – equipment operation, record keeping, administrative workflows. They keep both current, accessible, and integrated into daily operations.
The distinction matters because regulatory bodies assess whether clinics apply the right tool to the right situation. A task that requires clinical judgment but is treated as a rote procedure creates safety risk. A straightforward task that is documented as a complex protocol creates operational inefficiency. Clear boundaries improve both patient outcomes and staff effectiveness.
As healthcare becomes more complex, the need for structured decision-making and consistent execution grows. Practices that master the protocol vs procedure balance create operational clarity, reduce compliance risk, and support team members in delivering high-quality care. The documentation exists to serve the work, not the other way around.
Protocols guide clinical decision-making by defining when and why specific actions should occur based on patient presentation and clinical criteria. Procedures document the step-by-step execution of specific tasks, ensuring consistent performance regardless of who completes them. A protocol determines what treatment to provide; a procedure specifies how to administer it safely and correctly.
Hybrid documents sometimes combine protocol and procedure elements, often called standard operating procedures (SOPs). However, best practice separates them with clear section headings to distinguish clinical decision-making content from task execution steps. This prevents confusion about whether the document requires clinical judgment or operational consistency.
Clinical protocols require annual reviews at minimum, with interim updates when new evidence emerges or regulatory guidance changes. Procedures typically update less frequently unless equipment changes or workflow modifications occur. High-use documents benefit from quarterly reviews to ensure they remain practical and aligned with actual practice patterns.
Protocols require clinical expertise and are typically authored by medical directors, lead clinicians, or specialty practitioners, with approval from a clinical governance committee. Procedures can be written by operational staff with task-specific knowledge, such as nurses for clinical procedures or administrative staff for booking workflows, with clinical oversight ensuring patient safety.
Yes. The Care Quality Commission in the UK and the Joint Commission in the US expect healthcare facilities to maintain documented protocols for clinical decision-making and procedures for task execution. Both document types must be current, accessible to staff, and evidence-based. Audits assess whether practices follow their documented protocols and procedures during care delivery.