Musculoskeletal & Pain Management Physical Therapy
Berg Balance Scale Template
What Is the Berg Balance Scale Template? The Berg Balance Scale Template is a fr...
March 10, 2026
Discover free eBooks, guides and med spa templates on our new resources page

Buy now, pay later is now available in Pabau
Read case studies from our satisfied clients
Compare Pabau with alternative systems

Learn why this holistic care and aesthetic medicine clinic chose Pabau to power patient care and performance.
Read moreTroponin is a cardiac-specific biomarker that rises within 2-4 hours of myocardial injury and remains elevated for up to 14 days.
High-sensitivity troponin assays detect lower concentrations than conventional tests, enabling earlier MI detection but requiring careful interpretation to avoid false positives.
Serial troponin testing at 0 and 3 hours (or 0 and 1 hour with HS assays) is essential for ruling in or ruling out acute myocardial infarction.
Elevated troponin levels can occur in non-cardiac conditions including sepsis, renal failure, pulmonary embolism, and strenuous exercise.
Our free Heart Attack Troponin Levels Chart helps clinicians track serial results, interpret reference ranges, and document clinical assessment during cardiac evaluation.
A clinical reference chart with troponin reference ranges, serial results log, trend graph, and clinical assessment sections for cardiac evaluation.
Troponin is a regulatory protein complex found in cardiac and skeletal muscle that plays a crucial role in muscle contraction. When heart muscle cells are damaged during a heart attack, cardiac troponin molecules leak into the bloodstream where they can be measured.
Heart attack troponin levels are the gold standard biomarker for diagnosing acute myocardial infarction (MI). Unlike older cardiac markers such as creatine kinase-MB (CK-MB) or myoglobin, cardiac troponins (specifically troponin I and troponin T) are highly specific to heart tissue and remain elevated for an extended period.
According to the American Heart Association, troponin testing has revolutionised cardiac care by enabling clinicians to detect even small amounts of myocardial damage. This sensitivity is critical because prompt intervention can save lives and preserve heart function.
The timing of troponin release follows a predictable pattern. Levels typically begin to rise 2-4 hours after the onset of chest pain, peak at 24-48 hours, and can remain elevated for 7-14 days depending on the extent of damage. This extended elevation window makes troponin particularly useful for patients who present late after symptom onset.
Always document the exact time of symptom onset and sample collection. The troponin trend over time is more diagnostically valuable than a single measurement, as some patients with MI may have normal troponin on initial presentation.
Understanding cardiac troponin levels requires familiarity with the different assay types and their respective reference ranges. Normal values vary depending on whether conventional or high-sensitivity (HS) troponin assays are used, and some HS assays have sex-specific cutoffs.
Conventional Troponin I:
Conventional Troponin T:
High-Sensitivity Troponin I:
High-Sensitivity Troponin T:
These reference ranges represent the 99th percentile upper reference limit in healthy populations. Values above these thresholds indicate myocardial injury, but the clinical context determines whether the cause is acute MI, chronic cardiac conditions, or non-cardiac pathology.
It’s essential to verify the specific reference ranges for your laboratory, as different manufacturers and assay platforms may have slightly different cutoff values. The trend of rising or falling troponin levels over serial measurements is often more diagnostically significant than the absolute value.
Track troponin results, interpret levels, and assess cardiac risk
Enter a troponin result to see its clinical interpretation and category
Track multiple troponin measurements to identify rising or falling patterns
Normal and elevated troponin values by assay type
| Assay Type | Normal Range | Elevated | MI Threshold |
|---|---|---|---|
| Conventional Troponin I | 0–0.04 ng/mL | >0.04 ng/mL | ≥0.40 ng/mL |
| Conventional Troponin T | 0–0.10 ng/mL | >0.10 ng/mL | — |
| Assay Type | Sex | Normal Range | 99th Percentile |
|---|---|---|---|
| HS Troponin I | Male | 0–20 ng/L | 20 ng/L |
| HS Troponin I | Female | 0–15 ng/L | 15 ng/L |
| HS Troponin T | Male | 0–15 ng/L | 15 ng/L |
| HS Troponin T | Female | 0–10 ng/L | 10 ng/L |
Troponin levels typically begin to rise 2–4 hours after chest pain onset, peak at 24–48 hours, and remain elevated for 7–14 days depending on the extent of myocardial damage.
Testing at 0, 3, and 6 hours achieves sensitivity exceeding 99% for detecting MI when used with clinical assessment and ECG findings.
The European Society of Cardiology recommends 0/1-hour or 0/2-hour protocols for faster rule-out of acute MI in low-risk patients.
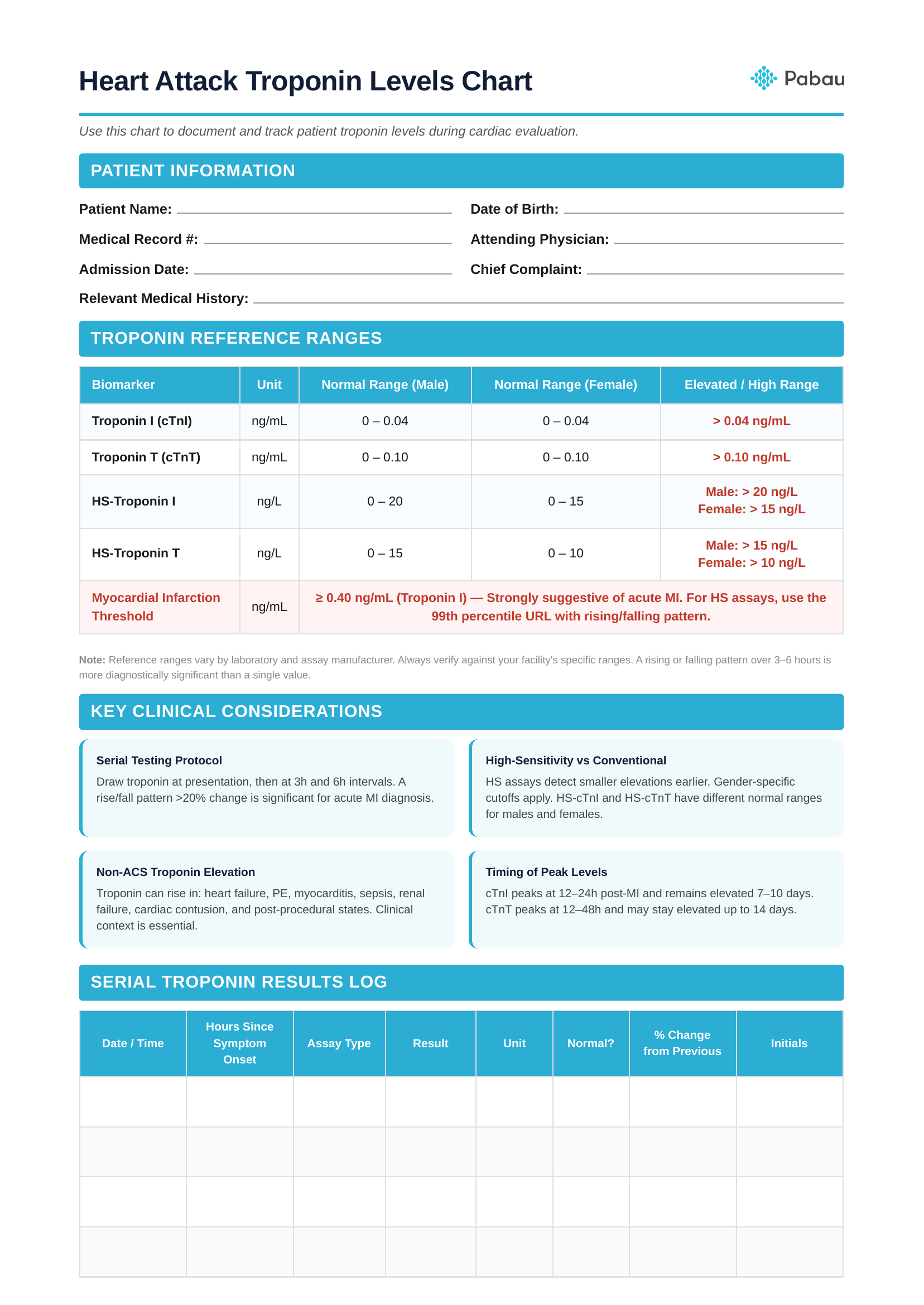
The Heart Attack Troponin Levels Chart is designed to streamline cardiac evaluation in emergency and inpatient settings. This comprehensive template helps clinical teams track serial troponin results, plot trends, and document the complete assessment process in one centralised location.
Patient Information Section: Begin by completing all demographic and clinical fields including patient name, date of birth, medical record number, attending physician, admission date, chief complaint, and relevant medical history. Accurate documentation of symptom onset time is critical for interpreting troponin kinetics.
Troponin Reference Ranges Table: Review the included reference ranges for your specific assay type. This quick-reference table displays normal and elevated values for conventional and high-sensitivity troponin I and T, helping you rapidly assess whether results fall within normal limits.
Serial Troponin Results Log: Record each troponin measurement in chronological order. For each sample, document the date and time of collection, hours elapsed since symptom onset, assay type used, numerical result, units, whether the value is normal or elevated, percentage change from the previous measurement, and your initials. This structured approach enables pattern recognition and supports clinical decision-making.
Troponin Trend Graph: Plot each troponin value on the graph to visualise the trend over time. The graph includes a marked 99th percentile upper reference limit line, making it easy to identify when values cross the diagnostic threshold. A rising pattern supports acute MI, whilst a falling pattern may indicate resolving injury or a non-ACS cause.
Clinical Assessment Section: Complete the holistic assessment by documenting ECG findings, presenting symptoms, cardiac risk factors, additional biomarkers (such as BNP or CK-MB), your clinical impression, and the management plan. This ensures all team members have access to the complete clinical picture alongside the troponin data.
Practitioner Sign-Off: Both the attending physician and the nurse or technician should sign and date the chart to verify accuracy and accountability. Proper documentation supports continuity of care and meets clinical documentation and HIPAA compliance standards.
Serial troponin testing is the cornerstone of ruling in or ruling out acute myocardial infarction. A single troponin measurement has limited diagnostic value because levels may be normal early in the course of an MI before sufficient cardiac damage has occurred.
The standard protocol for conventional troponin assays involves testing at presentation (0 hours) and repeating at 3 hours and sometimes 6 hours if clinical suspicion remains high. This approach has sensitivity exceeding 99% for detecting MI when both time points are used in conjunction with clinical assessment and ECG findings.
High-sensitivity troponin assays enable faster rule-out protocols. Many institutions use 0-hour and 1-hour testing algorithms that can safely discharge low-risk patients much sooner. The European Society of Cardiology recommends 0/1-hour or 0/2-hour protocols depending on the specific HS assay used.
When interpreting serial results, focus on both the absolute value and the delta change. A rise or fall of more than 20% between serial measurements suggests an acute process rather than chronic elevation. The magnitude of elevation correlates with infarct size and prognosis.
Document the exact troponin assay name and manufacturer in your clinical notes. Different HS-troponin tests have different validated algorithms and cutoff values, and this information is critical if the patient transfers to another facility or requires comparison with historical results.
Patients with unstable angina may have normal troponin levels despite active coronary ischaemia. Always integrate troponin results with clinical presentation, risk scores, and other diagnostic modalities. Troponin elevation confirms myocardial injury but doesn’t specify the mechanism or guide treatment alone.
The transition from conventional to high-sensitivity troponin assays represents one of the most significant advances in cardiac biomarker testing over the past decade. Understanding the differences between these technologies is essential for proper interpretation and clinical application.
High-sensitivity assays can detect troponin concentrations 10-100 times lower than conventional assays. This increased analytical sensitivity allows HS assays to measure troponin in the majority of healthy individuals, whereas conventional assays typically report “undetectable” or “<0.01 ng/mL" for normal patients.
The primary advantage of HS assays is earlier detection of myocardial infarction. Studies show that HS troponin can identify MI 1-2 hours earlier than conventional assays, enabling faster triage decisions. This capability supports rapid rule-out protocols that can safely discharge low-risk patients within 1-3 hours rather than 6-12 hours.
However, increased sensitivity comes with the challenge of decreased specificity. HS assays will detect small amounts of troponin release from non-cardiac causes, chronic stable cardiac disease, and even normal physiological variation. This means more patients will have detectable or mildly elevated troponin without acute MI.
Sex-specific cutoffs improve the diagnostic accuracy of HS troponin. Women typically have lower baseline troponin concentrations than men, and applying sex-specific 99th percentile values increases sensitivity for MI in women whilst maintaining specificity. Not all HS assays provide sex-specific reference ranges, so verify what your laboratory uses.
The universal definition of myocardial infarction requires troponin elevation above the 99th percentile plus either symptoms of myocardial ischaemia, new ECG changes, imaging evidence of new loss of viable myocardium, or identification of an intracoronary thrombus. Troponin elevation alone is insufficient for MI diagnosis.
When implementing HS troponin in your practice, ensure your digital forms system clearly distinguishes between conventional and HS assay results to prevent confusion. Educational initiatives for clinical staff are essential to prevent inappropriate troponin ordering and misinterpretation of results. Robust clinic management software can help standardise these workflows across your practice.
Elevated troponin levels do not always indicate acute coronary syndrome. Numerous cardiac and non-cardiac conditions can cause troponin release, and distinguishing these from acute MI is a common clinical challenge that requires careful assessment of the complete clinical picture.
Cardiac Causes (Non-ACS): Myocarditis and pericarditis cause troponin elevation through inflammatory damage to myocytes. Takotsubo cardiomyopathy (stress-induced cardiomyopathy) produces modest troponin elevation despite dramatic wall motion abnormalities. Heart failure, both acute decompensation and chronic stable disease, commonly causes mild troponin elevation. Cardiac contusion from trauma, cardioversion, ablation procedures, and cardiac surgery all release troponin into circulation.
Systemic Conditions: Sepsis and septic shock cause troponin elevation in up to 85% of critically ill patients through a combination of supply-demand mismatch, inflammatory mediators, and microvascular dysfunction. Renal failure reduces troponin clearance, leading to chronic mild elevation that may be the patient’s baseline. Pulmonary embolism causes right ventricular strain and troponin release, with elevation correlating with clot burden and prognosis.
Neurological Events: Subarachnoid haemorrhage and ischaemic stroke, particularly when involving the insular cortex, can cause dramatic troponin elevation through catecholamine surges and autonomic dysfunction. These patients may show ECG changes mimicking acute MI despite normal coronary arteries.
Other Causes: Strenuous exercise, particularly ultra-endurance events, causes transient troponin elevation in healthy individuals. Hypothyroidism, infiltrative diseases such as amyloidosis and sarcoidosis, and certain chemotherapy agents (especially anthracyclines) can elevate troponin. Rhabdomyolysis occasionally causes false-positive troponin results through cross-reactivity with skeletal muscle troponin.
The pattern of troponin elevation helps distinguish acute MI from other causes. Acute MI typically shows a rising pattern with levels that peak and then fall, whereas chronic conditions cause stable mild elevation. The magnitude also provides clues: levels above 10 times the upper reference limit strongly suggest acute MI, whilst mild elevations (1-3 times normal) are more likely from non-ACS causes.
Always correlate troponin results with clinical presentation, ECG findings, imaging, and other biomarkers. A patient with septic shock and mildly elevated troponin likely has supply-demand mismatch rather than plaque rupture, even though both technically cause myocardial injury.
Recognising when elevated heart attack troponin levels indicate acute MI rather than alternative causes requires integration of clinical history, physical examination, ECG findings, and biomarker kinetics. The Fourth Universal Definition of Myocardial Infarction provides clear criteria to guide diagnosis.
Clinical Presentation: Classic symptoms include chest pain or pressure, often radiating to the left arm, jaw, or back, associated with dyspnoea, diaphoresis, nausea, or light-headedness. However, up to 30% of MIs are “silent” or present with atypical symptoms, particularly in elderly patients, women, and those with diabetes. Any unexplained acute deterioration in a patient with cardiac risk factors warrants troponin testing.
ECG Findings: ST-segment elevation (STEMI) or new left bundle branch block in the appropriate clinical context indicates acute MI requiring immediate reperfusion therapy. Non-ST elevation MI (NSTEMI) may show ST-segment depression, T-wave inversion, or be entirely normal on initial ECG. Dynamic ECG changes (evolving over serial tracings) support acute ischaemia.
Troponin Kinetics: A rising and/or falling pattern of troponin with at least one value above the 99th percentile supports acute injury. Stable mildly elevated troponin suggests chronic myocardial disease rather than acute MI. The magnitude of change matters: a delta of >20% between serial samples (or absolute change >10 ng/L for HS assays) indicates an acute process.
Risk Stratification: High-risk features include ongoing chest pain, haemodynamic instability, life-threatening arrhythmias, mechanical complications, or markedly elevated troponin (>10x upper reference limit). These patients require urgent cardiology consultation and consideration for invasive coronary angiography.
The client record should document the decision-making process, including why acute MI was suspected or excluded. This supports continuity of care and meets regulatory requirements for cardiac event documentation.
Troponin testing should be reserved for patients with a reasonable pre-test probability of acute coronary syndrome. Indiscriminate screening of all emergency department patients or asymptomatic individuals leads to false positives, unnecessary downstream testing, and patient anxiety without improving outcomes.
Safer Clinical Notes best practices ensure troponin results and cardiac assessments are properly documented and accessible across care settings.
Client Record Systems with integrated lab result tracking help clinics maintain organised cardiac biomarker data and support longitudinal patient monitoring.
HIPAA Compliance requirements apply to all cardiac biomarker data, requiring secure storage, access controls, and audit trails for sensitive health information.
## Frequently Asked Questions
See how clinics reduce admin, improve clinical outcomes, and increase revenue with Pabau.

Normal troponin levels vary by assay type. For conventional troponin I, normal is 0-0.04 ng/mL. For high-sensitivity troponin I, normal is 0-20 ng/L for males and 0-15 ng/L for females. During a heart attack, troponin rises above these reference ranges, typically exceeding the 99th percentile cutoff within 2-4 hours of symptom onset. Serial testing is essential because early presentations may show normal troponin before sufficient cardiac damage has occurred.
Cardiac troponin remains elevated for 7-14 days following a heart attack, depending on the extent of myocardial damage. Troponin I and troponin T have similar kinetics, typically rising within 2-4 hours, peaking at 24-48 hours, and gradually declining over the subsequent week or two. This extended elevation window makes troponin useful for diagnosing MI in patients who present days after symptom onset, unlike older markers such as CK-MB which normalise within 48-72 hours.
Yes, numerous cardiac and non-cardiac conditions cause elevated troponin without acute myocardial infarction. Common causes include heart failure, myocarditis, pulmonary embolism, renal failure, sepsis, and strenuous exercise. Chronic stable cardiac disease may produce mildly elevated baseline troponin. The key to distinguishing acute MI from other causes is assessing the pattern of troponin change over serial measurements, correlating with clinical symptoms, ECG findings, and imaging studies rather than relying on a single elevated value.
Troponin I and troponin T are both cardiac-specific regulatory proteins used to diagnose myocardial injury, but they are encoded by different genes and detected by different assays. Troponin I is absolutely cardiac-specific, whilst troponin T may show very slight expression in skeletal muscle, though this rarely causes clinical confusion. Both have similar diagnostic accuracy for acute MI. The main practical difference is that individual laboratories use one or the other, so clinicians should familiarise themselves with whichever assay their institution employs and its specific reference ranges.
For suspected acute MI, troponin should be measured at presentation (0 hours) and repeated at 3 hours for conventional assays or 1-2 hours for high-sensitivity assays. If clinical suspicion remains high despite negative results, a third measurement at 6 hours may be warranted. Serial testing is essential because troponin may be normal very early in the course of MI. The trend of rising or falling values, along with the percentage change between measurements, provides critical diagnostic information beyond what a single value can offer.